











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
The COVID-19 pandemic is one of the greatest public health challenges in human history (Tandon, 2020). Therefore, it is essential to investigate psychological variables associated with the adoption of behaviors that contribute to the functional coping with this disease. For this study, the beliefs of efficacy were chosen because they are crucial for the objectives that a person adopts; the amount of effort undertaken in activities; perseverance when obstacles are encountered to reach these goals and resilience in the face of adversities, etc. (Bandura, 2000).
For the Social Cognitive Theory (SCT), the beliefs of efficacy represent an essential component for the exercise of human agency (Bandura, 1999); in other words, the ability to have influence over one's own life and environment. The beliefs of efficacy are the basis of human motivation and action (Bandura, 2004). From this perspective, people only engage in actions, such as those needed to mitigate COVID-19, when they believe they can produce the desired effects.
The SCT proposes three distinct but related types of efficacy beliefs (Bandura, 2000; Caprara et al., 2004): individual (self-efficacy), collective and proxy. Self-efficacy refers to the individual's beliefs about their own ability to perform tasks or achieve established goals. Collective efficacy is the belief shared by members of a group about their ability to, acting collectively, perform certain tasks or achieve group goals. Proxy efficacy refers to the individual's beliefs about the ability of others, who have the necessary influence, power and/or knowledge, to act in their favor so that their goals are achieved.
In a health emergency, such as the COVID-19 pandemic, individual actions, like hand hygiene and controlling touches on the face, mouth and nose, are not enough. Pandemic mitigation depends on collective efforts. For example, other people in the family and community have also to adopt behaviors that prevent the spread of the virus and governments must implement health measures to protect the population (Airhihenbuwa et al., 2020; Anderson et al., 2020; Prime et al., 2020). Achieving and/or maintaining health states requires individual, collective and proxy agency (Li, 2018; Thaker et al., 2019; Webster et al., 2020).
It is important to reiterate that understanding the beliefs of efficacy to deal with the COVID-19 pandemic can contribute to the comprehension and prediction of individual and collective behavior and, therefore, to plan public policies that aim to mitigate this disease. It should also be stated that publications that have investigated these three forms of efficacy together have not been identified in the scientific literature, regardless of whether their object is a serious health crisis or not. In addition, although there are scales that measure efficacy beliefs in health-related contexts (e.g., Li, 2018), none have been related to COVID-19 in any of the three spheres (individual, collective and proxy). It should also be mentioned that the efficacy beliefs are object-specific (Bandura, 2006): they are specific for coping with each particular health condition.
Therefore, the present study aimed to analyze the psychometric properties of six efficacy beliefs to cope with COVID-19 scales, specifically the evidence of validity based on the internal structure and the reliability estimates. Additionally, it aimed to compare the levels of efficacy to face this disease in a Brazilian sample.
Method
Participants
Participants were recruited in a non-probabilistic manner through social networks on the Internet and “Snowball” with instant messaging applications and email. The inclusion criteria were living in Brazil, being able to read and having a device with an Internet connection. There were no exclusion criteria.
Instruments
Based on guidelines from the World Health Organization (WHO) (e.g., United Nations Children's Fund, WHO & International Federation of Red Cross and Red Crescent Societies, 2020; WHO, 2020) and Bandura (2006), six efficacy beliefs to cope with COVID-19 scales were built (see Supplementary Material): Autoeficácia para Enfrentamento da COVID-19 (AE-C19) (Self-efficacy for Coping with COVID-19); Eficácia Familiar para Enfrentamento da COVID-19 (EFam-C19) (Family Efficacy for Coping with COVID-19); Eficácia Comunitária para Enfrentamento da COVID-19 (ECom-C19) (Community Efficacy for Coping with COVID-19); Eficácia Delegada para Enfrentamento da COVID-19 - Governo Municipal (ED-C19-Municipal) (Proxy-Efficacy for Coping with COVID-19 - Municipal Government); Eficácia Delegada para Enfrentamento da COVID-19 - Governo Estadual (ED-C19-Estadual) (Proxy-Efficacy for Coping with COVID-19 - State Government); and Eficácia Delegada para Enfrentamento da COVID-19 - Governo Federal (ED-C19-Federal) (Proxy-Efficacy for Coping with COVID-19 - Federal Government). Thus, the three forms of agency - individual, collective and proxy (Bandura, 1999) - were contemplated.
Each of the first three scales have 15 items conceived to reflect the main tasks required to mitigate the coronavirus pandemic (e.g., “Hand hygiene correctly and several times a day.”) randomly organized. The items were generated following WHO guidelines to encourage the adoption of behaviors to mitigate COVID. The instructions presented at the beginning of each scale ask the participant to answer about what they think they are capable of doing (AE-C19), that their family is capable of (EFam-C19) or that their community is capable of (ECom-C19). The ECom-C19 instructions ask the participant to consider “community” as the people who live nearby and/or with whom they have a close relationship.
Each proxy-efficacy scale has 10 items randomly organized that reflect the main tasks of the different levels of government related with COVID-19 coping (e.g., “Use scientific knowledge to combat COVID-19.”). The instructions to fill in each scale ask respondents to assess how much they believe that the respective level of government (municipal, state, or federal) is capable of performing the activities described in each item.
In all scales, the items were randomly arranged and had to be answered on a ten-point Likert scale adapted from the guide for constructing efficacy scales (Bandura, 2006). The higher the score, the greater the belief in the individual, family, community, or governmental capacity to cope with the pandemic.
In addition to the efficacy scales, a demographic questionnaire was used. This measure and the scales were used on a pilot application with three school-level people that were equivalent or less than that of the target sample and were selected for convenience. This procedure aimed to verify the comprehensibility and the time required to answer the questionnaire, and revealed that the instruments (questions, instructions, etc.) did not require changes.
Procedures
After being approved by the National Commission for Ethics in Research (CONEP - CAAE 30689820.0.0000.5147), a form containing the term of acquiescence and consent, the demographic questionnaire and the efficacy scales was made available on the Internet. There was no time control for filling it out.
The data were treated quantitatively using descriptive statistics (mean, etc.) and inferential statistics (significance level of 5%). Exploratory Factor Analysis (EFA) was performed using the Factor 10.10.03 software. The adequacy of the data matrix for factoring was assessed based on the Kaiser-Meyer-Olkin (KMO) criterion and Bartlett's Sphericity Test (χ2). The Hull method was used to determine the number of factors, the ULS (Unweighted Least Squares) method for factoring, the Robust Promin rotation method to achieve factor simplicity and polychoric correlations or Pearson were also used, depending on the results.
Based on Damásio and Dutra (2017), the following model adequacy indicators were used: Non-Normed Fit Index (NNFI) (≥ .90); Comparative Fit Index (CFI; ≥ .90); Goodness of Fit Index (GFI; ≥ .90); Adjusted Goodness of Fit Index (AGFI) (≥ .90); Root-Mean-Square Error of Approximation (RMSEA; <.10) and H-Latent (> .80). The plausibility indices of a unidimensional solution were also evaluated: Unidimensional Congruence (UniCo; > .95); Explained Common Variance (ECV; > .85); and Mean of Item Residual Absolute Loadings (MIREAL; < .30). Internal consistency was assessed using Cronbach's alpha and item-total correlation. As a cutoff point, the authors used the factor load of .30 (Field, 2013), so that the items were included in each factor. This, however, took into account the weightings of Lambert et al., (1991) on the adoption of cutting point values for factor loads to determine the factorial structure.
Since there was no normal distribution, the Friedman test (χ²) with multiple comparisons Stepwise Step-down was used to compare the scores of the efficacy scales. The Spearman test was used to correlate these measures.
Results
This study involved 518 participants who lived in Brazil, in 14 of the 27 federative units. Table 1 shows the sample characterization.
Table 1 Characterization of the sample and subsamples.
| Variable | |||
| Age (years) | M = 32.28 Minimum = 17 | SD = 12.669 Maximum = 72 | |
| Female | n = 365 | 70.5% | |
| Gender | Male | n = 151 | 29.2% |
| Non informed | n = 2 | .4% | |
| White | n = 347 | 67.0% | |
| Parda/mixed | n = 131 | 25.3% | |
| Race/skin color | Black | n = 35 | 6.8% |
| Yellow | n = 4 | .8% | |
| Indigenous | n = 1 | .2% | |
| None | n = 0 | .0% | |
| Elementary school | n = 3 | .6% | |
| High School | n = 178 | 34.4% | |
| Educational degree | College degree | n = 125 | 24.1% |
| Specialization degree | n = 88 | 17.0% | |
| Masters’ degree | n = 68 | 13.1% | |
| Doctorate | n = 56 | 10.8% | |
| Socioeconomic statusa | A (R$25,554.33) | n = 38 | 7.3% |
| B1 (R$11,279.14) | n = 106 | 20.5% | |
| B2 (R$5,641.64) | n = 134 | 25.9% | |
| C1 (R$3,085.48) | n = 120 | 23.2% | |
| C2 (R$1,748.59) | n = 71 | 13.7% | |
| D-E (R$719.81) | n = 49 | 9.4% |
Note: a During the month in which the data for the present study was collected R$ 1.00 (one Brazilian real) was equivalent to U$ 0.17 US dollar (source: http://www.ipeadata.gov.br).
Table 2 presents the scores and the results of the EFA of the six scales. The factorability of the correlation matrix between the items of the scales was confirmed by KMO and χ2, with values considered adequate for the six instruments. The Hull retention method indicated that each scale represents a unidimensional measure. The total variance explained was above 42% on all scales. The plausibility of unidimensionality was also confirmed by the UniCo, ECV and MIREAL indices. Higher than .915, the H-Latent index thus shows that the set of items on each scale represents a well-defined latent variable and is likely to remain stable between studies. Values greater than .90 obtained for NNFI, CFI, GFI and AGFI suggest, in isolation, the adequacy of the scales.
All items on the collective efficacy and proxy-efficacy scales saturated in the extracted factor and presented factorial loads between .445 and .960. In the AE-C19, only one item saturated below the borderline value of .30 (Field, 2013) but, even so, was very close to it (.296). Additionally, the communality was above the minimum value of .20 (Child, 2006) for almost all the items of the scales, except for the scales of self-efficacy, which showed lower values in two (.087 and .116), and family efficacy, which showed a lower value in one (.198) of the items. Analyzing the internal consistency considering Cronbach's alpha, the scales presented the following indices: .819 (AE-C19); .921 (EFam-C19); .968 (ECom-C19); .927 (ED-C19-Municipal); .957 (ED-C19-Estadual); and .962 (ED-C19-Federal).
Table 3 shows the corrected item-total correlation and alpha values if items were deleted. Two items (namely, items 1 and 2 of the AE-C19) did not reach the minimum acceptable value in the item-total correlation, i. e., greater than .30 (Kline, 2000) and, if excluded, would raise the values of Cronbach's alpha, but not significantly. The removal of other items would not contribute to substantially increase the alpha in any of the measures.
Table 2 Adequacy indicators of the unifactorial structure for the six efficacy for coping with COVID-19 scales.
| Autoeficácia para Enfrentamento da COVID-19a | Eficácia Familiar para Enfrentamento da COVID-19a | Eficácia Comunitária para Enfrentamento da COVID-19b | Eficácia Delegada para Enfrentamento da COVID-19 - Governo Municipalb | Eficácia Delegada para Enfrentamento da COVID-19 - Governo Estadualb | Eficácia Delegada para Enfrentamento da COVID-19 - Governo Federala | |
| χ2 (p < .001) | 3281.9c | 5548.2c | 5885.0c | 3632.4d | 5550.0d | 5904.2d |
| KMO | .90520 | .93850 | .96857 | .91479 | .93244 | .92512 |
| Explained Variance | .42175 | .55826 | .69075 | .60667 | .72477 | .82284 |
| UniCo | .951 | .965 | .995 | .972 | .973 | .972 |
| ECV | .870 | .897 | .947 | .878 | .895 | .912 |
| MIREAL | .199 | .198 | .158 | .255 | .241 | .203 |
| RMSEA | .049 | .075 | .055 | .140 | .171 | .152 |
| NNFI | .984 | .980 | .993 | .939 | .940 | .965 |
| CFI | .986 | .983 | .994 | .953 | .954 | .972 |
| GFI | .981 | .988 | .997 | .986 | .991 | .995 |
| AGFI | .978 | .986 | .997 | .982 | .989 | .993 |
| H-Latent | .915 | .954 | .971 | .936 | .965 | .985 |
| Factor loading e | .296 - .768 | .445 - .863 | .636 - .885 | .545 - .833 | .658 - .909 | .692 - .962 |
| Communality e | .087 - .589 | .198 - .745 | .404 - .783 | .297 - .695 | .433 - .826 | .478 - .925 |
Note: a During the month in which the data for the present study was collected R$ 1.00 (one Brazilian real) was equivalent to U$ 0.17 US dollar (source: http://www.ipeadata.gov.br).
Table 3 Adequacy indicators of the unifactorial structure for the six efficacy for coping with COVID-19 scales.
| Autoeficácia para Enfrentamento da COVID-19 | Eficácia Familiar para Enfrentamento da COVID-19 | Eficácia Comunitária para Enfrentamento da COVID-19 | Eficácia Delegada para Enfrentamento da COVID-19 - Governo Municipal | Eficácia Delegada para Enfrentamento da COVID-19 - Governo Estadual | Eficácia Delegada para Enfrentamento da COVID-19 - Governo Federal | ||||||||
| Item | ra | αb | ra | αb | ra | αb | ra | αb | ra | αb | ra | αb | |
| 1 | .230 | .831 | .387 | .924 | .625 | .968 | .781 | .916 | .850 | .951 | .895 | .956 | |
| 2 | .239 | .822 | .380 | .922 | .743 | .966 | .748 | .918 | .842 | .951 | .877 | .957 | |
| 3 | .508 | .805 | .594 | .917 | .804 | .965 | .716 | .919 | .788 | .954 | .877 | .957 | |
| 4 | .588 | .798 | .706 | .913 | .832 | .965 | .791 | .915 | .856 | .951 | .914 | .956 | |
| 5 | .473 | .806 | .690 | .914 | .845 | .964 | .750 | .918 | .886 | .950 | .894 | .956 | |
| 6 | .411 | .810 | .553 | .918 | .796 | .965 | .534 | .928 | .691 | .957 | .659 | .966 | |
| 7 | .548 | .802 | .749 | .912 | .870 | .964 | .742 | .918 | .830 | .952 | .866 | .957 | |
| 8 | .408 | .811 | .581 | .917 | .778 | .966 | .747 | .918 | .849 | .951 | .868 | .957 | |
| 9 | .593 | .802 | .707 | .913 | .813 | .965 | .786 | .916 | .869 | .950 | .899 | .956 | |
| 10 | .571 | .798 | .730 | .912 | .851 | .964 | .572 | .926 | .653 | .959 | .636 | .966 | |
| 11 | .546 | .809 | .719 | .913 | .822 | .965 | - | - | - | - | - | - | |
| 12 | .487 | .807 | .744 | .912 | .860 | .964 | - | - | - | - | - | - | |
| 13 | .474 | .806 | .717 | .913 | .833 | .965 | - | - | - | - | - | - | |
| 14 | .516 | .805 | .750 | .912 | .836 | .965 | - | - | - | - | - | - | |
| 15 | .400 | .813 | .545 | .918 | .721 | .967 | - | - | - | - | - | - | |
Note: a Corrected item-total correlation; b Alpha if item is deleted.
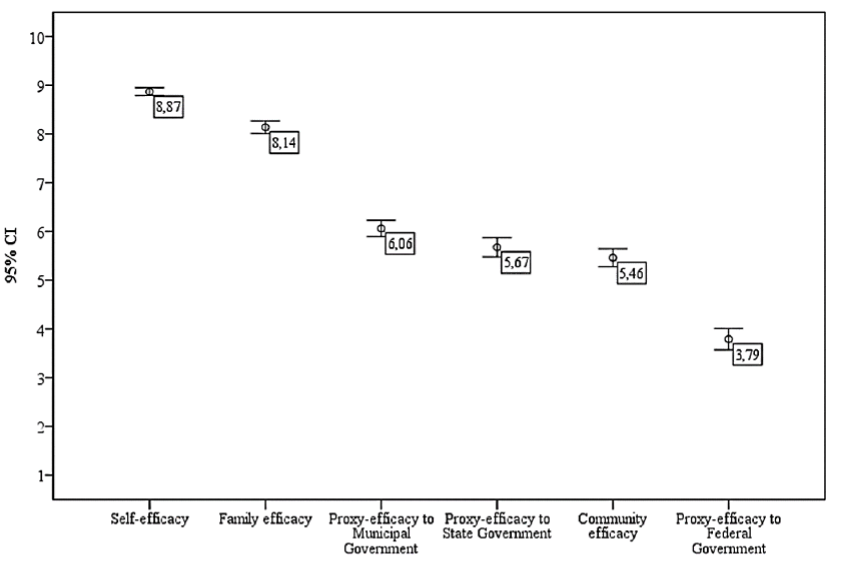
Friedman's test revealed that the mean scores (Figure 1) of the six instruments differed statistically, χ² (518; 5) = 1345,544; p < .001. Multiple comparisons formed five homogeneous subgroups (p < .05) in decreasing order of efficacy level: AE-C19; EFam-C19; ED-C19-Municipal; ED-C19-Estadual and ECom-C19 (p = .281); and ED-C19-Federal (Figure 1).
Among the 15 possible correlations between the scores of the efficacy scales, 12 were significantly positive, one strong, three moderate, eight weak and three null (Table 4). ECom-C19 and ED-C19-Municipal were the only measures that correlated with all the others. The three proxy-efficacy scales showed moderate or strong correlations between each other.
Table 4 Correlations between the efficacy scales scores.
| Efficacy for coping with COVID-19 scales | 1 | 2 | 3 | 4 | 5 | 6 |
| 1. Self-efficacy | 1 | |||||
| 2. Family efficacy | .510** | 1 | ||||
| 3. Community efficacy | .216** | .329** | 1 | |||
| 4. Proxy-Efficacy to Municipal Government | .186** | .185** | .391** | 1 | ||
| 5. Proxy-Efficacy to State Government | .098* | .050 | .355** | .716** | 1 | |
| 6. Proxy-Efficacy to Federal | -.058 | -.083 | .292** | .432** | .649** | 1 |
Note: *p < .05; **p <. 01.
Discussion
Individually and collectively, therefore, health behaviors can be understood and, in part, predicted by individuals’ beliefs of efficacy (Bandura, 2004). As a health behavior, mitigating the COVID-19 pandemic also evidently requires individual, collective (family, community, etc.) and proxy (governments, etc.) agency (Airhihenbuwa et al., 2020; Anderson et al., 2020; Prime et al., 2020). Therefore, building measures of beliefs of efficacy to cope with this disease that contemplate these different levels of agency, as well as analyze its psychometric properties have evident and high scientific and social relevance.
When analyzing the psychometric properties of the efficacy for coping with COVID-19 scales, all proved to have a unidimensional structure, showing that each of the six beliefs about COVID-19 coping efficacy investigated constitutes a single construct. This converges with Bandura (2006), who proposes that measures of efficacy should have a specific object.
However, unsatisfactory results were observed for the one-dimensional model in some of the indexes. For example, the RMSEA was above that recommended (Damásio & Dutra, 2017) in the three scales of proxy efficacy. Commonality, however, presented values below the minimum indicated (Child, 2006) for some items of the scales of self-efficacy and family efficacy, which indicates that these items may present problems. Despite this, the explained variance, the NNFI, CFI, GFI, AGFI and H-Latent adjustment indexes suggest the adequacy of the model.
Based on these results and additionally considering the theoretical contribution that supported the items’ generation and the propositions of the TSC, we would suggest that the six instruments be considered one-dimensional and that all items should be kept, as parsimonious indications of evidence of validity based on the internal structure for the efficacy scales for coping with COVID-19.
Regarding the reliability estimates, the internal consistency indexes were considered good or excellent. Although there are warnings in the literature (Taber, 2018) that very high Cronbach's Alpha values may denote redundancy between items, this does not seem to occur in the COVID-19 efficacy scales. The items were generated in such a way that, on the six scales, each item reflects a type of behavior necessary to cope with COVID-19. Thus, it is considered that the high correlation between them, which is reflected in the high internal consistency indexes, indicates that each scale actually measures a single construct.
Therefore, it can be said that, as a whole, the validity evidence based on the internal structure and the reliability estimates are satisfactory for the scales, although, as mentioned above, with parsimony for the former. Validity evidence and reliability estimates are considered minimum quality requirements for any psychological measure (American Educational Research Association, American Psychological Association, & National Council on Measurement in Education, 2014). Furthermore, in times of social distance due to COVID-19, online psychological instruments that allow remote application are essential (Wright, Mihura, Pade, & McCord, 2020).
It was observed that the levels of efficacy tend to decrease when the control of actions moves away from the individual. Self-efficacy was the highest, followed by family efficacy. The federal government’s proxy-efficacy had the lowest score. At the intermediate levels, however, the averages of ED-C19-Municipal and ED-C19-Estadual were slightly higher than that of ECom-C19. The lowest scores in federal proxy-efficacy may be related to the perception of the inadequacy of the posture adopted by this level of government, especially the executive, when facing COVID-19 (Campos, 2020). By disowning science, the federal executive opposed the mitigation measures adopted by states and municipalities, which culminated in the unanimous decision of the Brazilian Supreme Federal Court that states and municipalities have autonomy to determine measures of social isolation (Lima, Pereira & Machado, 2020).
The high level of self-efficacy accompanied by lower scores of beliefs of efficacy related to the community is worrying. Germani, Buratta, Delvecchio and Mazzeschi (2020) point out that shared goals, interdependence and sociability must be emphasized and promoted as a protective factor against COVID-19. The proxy agency, for example, played a major role in determining behavior in analogous situations, such as Ebola epidemics (Li, 2018; Webster et al., 2020). Thus, even if the level of self-efficacy is high, as observed in this study, the adoption of health behaviors may be at risk, as the belief in the community's ability to deal with the situation is low. Therefore, to increase adherence to COVID-19 mitigation measures, it is necessary to take actions that favor the increase of the governmental proxy-efficacy, especially at federal level.
The correlations between self-efficacy and other beliefs of efficacy also tend to weaken the further away control over the actions necessary to achieve the objective (mitigation of COVID-19) is from the individual. Thus, the moderate positive correlation between self-efficacy and collective family efficacy can be explained by the more intense and direct participation of the individual in this group. The significant positive correlations between the ECom-C19 and ED-C19-Municipal scores and those of the other instruments are possibly due to the fact that the community and the municipality are intermediate instances; in other words, contexts with easier participation or access. The moderate or strong positive correlations between the three proxy efficacy scales were expected and showed expressive convergence between them, despite the fact that the average beliefs in the ability of the three levels of government to mitigate COVID-19 were distinct.
The existence of positive correlations between most measures, although predominantly weak or moderate, indicates that, even though different, they are associated constructs. Thus, it corroborates Caprara et al. (2004) who obtained similar results in research into self-efficacy and collective family efficacy.
Among the limitations of this study, those related to external validity stand out. The sample, which is predominantly white, female, highly educated and with high income, differs from the Brazilian population. As for internal validity, the online collection strategy and the fact that confirmatory factor analysis have not been carried out are circumscriptions. Therefore, other studies are recommended to test the efficacy for coping with COVID-19 scales in more representative and randomized samples. We would also suggest that other evidence of validity (based on the relationship with other variables, etc.) and more estimates of reliability (stability, etc.) for them be obtained.
Despite those and other limitations, it is possible to state that the measures of efficacy for coping with COVID-19 have adequate psychometric properties. They therefore represent a contribution to further research on factors that influence behavior in health emergencies, such as the current one, generating fundamental knowledge for the development of evidence-based interventions to preserve health and lives.
Credit authorship contribution statement
Andrêze Cristine do Nascimento Silva: Conceptualization; Data Curation; Formal analysis; Funding acquisition; Investigation; Methodology; Project administration; Visualization; Writing - Original Draft; Writing - Review & Editing. Juliana Célia de Oliveira: Data Curation; Formal analysis; Methodology; Validation; Visualization; Writing - Original Draft. Altemir José Gonçalves Barbosa: Conceptualization; Data Curation; Formal analysis; Funding acquisition; Investigation; Methodology; Project administration; Supervision; Validation; Visualization; Writing - Original Draft; Writing - Review & Editing. Roseane Ribeiro Mendonça: Validation; Writing - Original Draft.

