











 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
Primary cutaneous anaplastic large-cell lymphoma (C-ALCL) is a rare subtype of non-Hodgkin T-cell lymphoma with exclusively cutaneous onset and location1, composed of large, atypical lymphocytes of either pleomorphic, anaplastic or immunoblastic cytomorphology, and expression of the CD30 antigen by more than 75% of tumor cells2. It often occurs at a median age of 60, although it may occur at any age3, and it is the second most common manifestation of cutaneous T-cell lymphoma2. The clinical course of C-ALCL is predominantly indolent, distinct from the systemic anaplastic large-cell lymphoma3.
The rarity of primary C-ALCL justifies this case report, and the main goal is to emphasize the importance of considering this diagnosis as a possibility in large-cell cutaneous lymphomas. Therefore, the report presents the clinical identification of the lesion, anatomopathological findings, and a literature review on the theme, including pathophysiology, epidemiological aspects, clinical manifestations, and treatment.
Case report
Female, 58 years old, referred to the dermatology department after surgical resection of a nodular lesion with rapid growth on the right calf, performed 5 months earlier.
The pathology report indicated a malignant neoplasm of lymphoid/epithelioid atypical cells, ulcerated, infiltrating to the deep reticular dermis and hypodermis. Lateral and deep surgical margins were negative.
When the patient was examined, she presented new painful, violaceous papules, and nodules in the right lower limb (Fig. 1). Lymphadenopathy in the inguinal chain was absent. Thus, a biopsy of the new lesions was carried out, as well as an immunohistochemistry request for better diagnostic definition.

Figure 1 Large violaceous nodule in lower right limb, measuring 3.6 × 2.3 cm, accompanied by smaller papules below.
At a follow-up appointment 1 month later, the patient still had violaceous plaques on the right lower limb and no lymphadenopathy associated. The pathology reports were not available yet.
The patient was lost to follow-up and returned after approximately 1 year with the result of the immunohistochemical study of the first lesion resected from the right calf. The neoplasm was positive for CD45, CD30, and CD3 (Fig. 2). AE1AE3, S100, and CD20 antibodies, indicative of epithelial, melanocytic, and B-lymphoid lineage, were negative. The anaplastic lymphoma kinase (ALK) protein was also negative. The morphological features, combined with the immunohistochemical profile, revealed a CD30-positive lymphoproliferative disorder in the skin, consistent with C-ALCL.
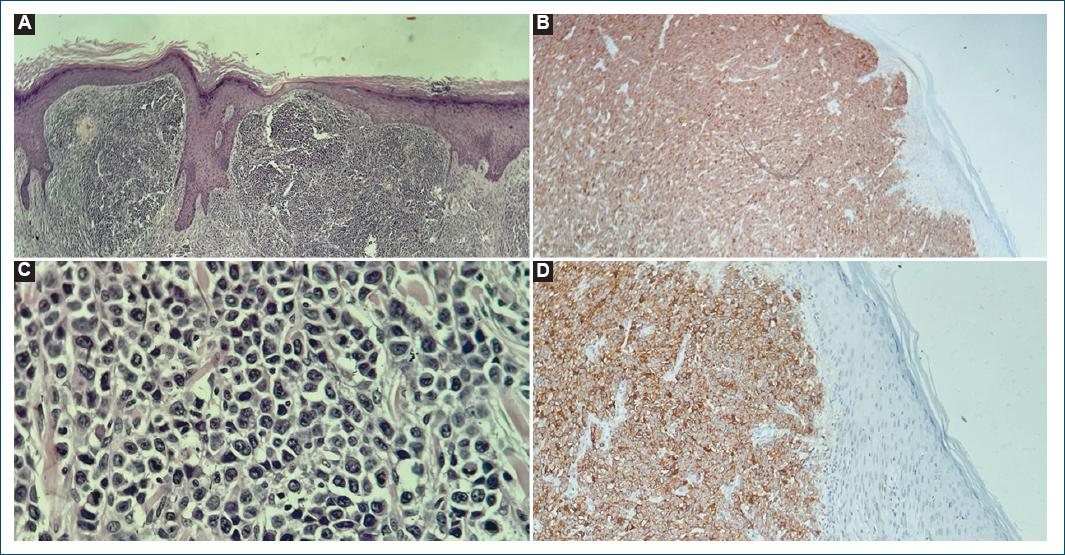
Figure 2 Histopathological and immunohistochemical (IHC) characteristics of skin neoplasm. A: panoramic view showing neoplasm infiltrating the dermis (×40, H&E). B: large cells with anaplastic features and mitosis in detail (×100, H&E). C: CD30 (×400, IHC). D: CD3 (×100, IHC).
A positron emission tomography-computed tomography scan was performed, and no signs of systemic disease were found. The final diagnosis was primary C-ALCL.
Thus, the patient was referred to the hematology department. Radiotherapy was then administered for 4 weeks.
Lesions regressed but recurred about 1 year after treatment. The patient is currently undergoing a new cycle of radiotherapy.
Discussion
Primary cutaneous lymphomas are a heterogeneous group of non-Hodgkin lymphomas of the skin that does not have extracutaneous manifestations at the time of diagnosis. They mainly originate from T cells, even though they can also originate from B cells4.
Approximately 6.4 million people worldwide are affected by primary cutaneous lymphomas4. The World Health Organization-European Organization for Research and Treatment of Cancer classification subdivides these types of lymphomas. According to this classification, among the subtypes of primary cutaneous lymphoma are primary cutaneous CD30+ lymphoproliferative disorders, in which CD30+ anaplastic large-cell lymphoma stands, also known as primary C-ALCL2.
Anaplastic large-cell lymphoma is the second most common skin T-cell neoplasm after mycosis fungoides, accounting for approximately 30% of primary cutaneous lymphomas5. The group with the highest incidence is adults between 45 and 60 years old, with a slight predominance in males6.
C-ALCL is mostly asymptomatic3. The presence of solitary papules or nodules, mainly located on the trunk or extremities, characterizes the disease7. These nodules persist for 3-4 weeks, tend to ulcerate over time, and show spontaneous regression (20-42% of cases) followed by relapses5. On average, 20% of patients present multifocal lesions, even though extracutaneous involvement rarely occurs2.
Diagnosis occurs through clinical findings, laboratory tests, skin biopsy with anatomopathological analysis, and complementary immunohistochemical evaluation. At this stage, it is significant to ensure that in addition to positivity for CD30, negativity for ALK-1 is required to exclude the possibility of systemic ALCL with cutaneous involvement since this manifestation is more aggressive than C-ALCL8.
Histological examination reveals a neoplastic proliferation of large lymphocytes in the dermis and subcutaneous cellular tissue. The epidermis is not usually involved, although epidermotropism is occasionally present9. The lymphocytes are of anaplastic appearance, with irregular and prominent nuclei, abundant cytoplasm, atypical mitoses, and some cells with plasmacytoid appearance7.
The prognosis depends on multiple clinical and histopathological factors, with a median survival of 5 years in 97.5% of cases in the early stage7. Patients over 60 years old, absence of spontaneous regression, presence of extracutaneous dissemination, and extensive limb disease are related to an unfavorable prognosis5.
As for treatment, it is mainly performed by local surgical excision. Radiotherapy is reserved for cancers with high tumor mutational burden and systemic chemotherapy is typically reserved for cases with a greater extent of disseminated disease5.
In addition, when the lymphoma is refractory to main therapies, there is the possibility of performing autologous or allogeneic stem cell transplantation. However, due to the high morbidity and mortality associated with this therapy, it is reserved for stable patients with risk-benefit assessments10.
Conclusion
Primary C-ALCL is an uncommon subtype of T-cell lymphoma. It is an exclusively cutaneous neoplasm and is distinguished by the presence of CD30-positive cells. Upon diagnosis of cutaneous ALCL, it is necessary to confirm the negativity for ALK-1 protein, to exclude the possibility of cutaneous manifestation of the systemic ALCL, which has worse prognosis.

