











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
PermalinkIntroduction
The International Health Regulations (IHR) were created by the World Health Organization (WHO) in 1969 with the purpose of controlling the international spread of six diseases (cholera, plague, relapsing fever, smallpox, typhoid, and yellow fever). The Regulations outline the responsibilities of states regarding the notification of communicable diseases and are designed to maintain the highest level of security against the global spread of diseases with the least amount of disruption to global trade 1. The most recent version of the IHR is from 2005. The changes in the IHR(2005) made it so that the spectrum of diseases it aims to prevent was broadened over the years. To this day, it remains a part of international law that binds 196 countries. The primary goal now is to prevent the spread of any disease that could potentially become a Public Health Emergency of International Concern (PHEIC). Each country is responsible for the national implementation of the IHR (2005). The role of the WHO is to assist countries with the implementation at the national level and to coordinate the response at the international level. Countries should be able to detect, assess, and respond to public health events, as well as report them to the WHO 2.
Vector-borne diseases (VBD) are diseases spread by “vectors”, which are living organisms that can transmit infectious pathogens between humans, or from animals to humans, and cause illnesses 3. These diseases include several mosquito-borne viral infections with a significant public health impact, such as West Nile, Dengue, Chikungunya, Japanese encephalitis, Yellow fever, Rift Valley fever, and Zika virus, as well as parasitic infections such as Malaria and Lymphatic filariasis. Other well-established and important VBD are those transmitted by ticks, such as Lyme Borreliosis, Crimean-Congo hemorrhagic fever, Tick-borne encephalitis, and Typhus (the last, also transmitted by mites, lice, and fleas). Other relevant vector-borne diseases include those transmitted by triatomine bugs (Chagas disease), by flies (Onchocerciasis and Human African Trypanosomiasis), by snails (Schistosomiasis), or by phlebotomine sandflies, such as cutaneous, mucocutaneous, and visceral Leishmaniasis. Vector avoidance strategies are therefore critical to the prevention of these infections. According to the WHO’s Global Vector Control Response 2017-2030, 80% of the world’s population is at risk of one VBD, and more than half are at risk of two or more VBD. Additionally, VBD account for 17% of the global burden of communicable diseases, with over 700,000 deaths annually. VBD has recently expanded into new regions, with illnesses that were previously only seen in tropical and subtropical regions becoming prevalent in temperate regions. Climate and environmental changes, increased worldwide travel and trade, changes in land use patterns such as deforestation, unplanned urbanization, inadequate solid waste management, and lack of piped water are all major factors contributing to the emergence or re-emergence of VBD 4.
The interplay between demographic, social, and environmental factors has resulted in the geographic dispersion and extended duration of transmission seasons for VBD, emphasizing the immediate need for a comprehensive approach to vector control. In this article, we aim to perform a scoping review of the literature on the implementation and operationalization of measures to control the spread of VBD within the scope of the IHR. The focus of this article was specifically on surveillance at Points of Entry (PoE), epidemic intelligence, entomological surveillance, and control of the vaccination status of travelers at airports, ports, and ground crossings 5. We searched for articles within the scope of the implementation of such measures at both the continental and national levels. The purpose was to understand how these measures are being implemented and shed light on the successes and struggles of these implementations in different countries around the globe.
Materials and Methods
Review Question
The specific review question aimed to characterize the evidence of the IHR measures implemented to control the occurrence of VBD worldwide.
Objectives
To identify the effects of existing IHR strategies and interventions that have been developed for monitoring, restricting, and controlling the occurrence of VBD.
To classify strategies and interventions that have been implemented, according to their suitability and efficacy in controlling and preventing the development of VBD in human populations.
Type of Review and Justification
We conducted a scoping review as the body of literature concerning the implementation of the IHR on VBD has not yet been comprehensively reviewed. A second reason was the heterogeneous nature of content and measures found, which was not amenable to a more precise systematic review. Therefore, the authors opted for a scoping review as it provides a preliminary assessment of the potential scope and size of the available literature, allowing for the identification of the nature and extent of research evidence.
Review Process
In order to seek and map the evidence in such a broader approach, the authors standardized the conduct and reporting of this review taking into account the guidance developed by the members of the Joanna Briggs Institute and Collaborating Centres and the Search, Appraisal, Synthesis and Analysis (SALSA) Framework 6,7. Prior to the review itself, a scoping review protocol was developed where the objectives and methods were predefined. The search strategy was comprehensive to identify both published and unpublished (grey literature) references. We searched relevant databases, namely SCOPUS™, Web of Science™, and PubMed™, to search for articles published since 1990.
Combinations of the terms: “International Health Regulations,” and “vector-borne diseases,” contained in the title, abstract, and index terms were searched. Our final queries for the search were: “vector-borne” AND (“international health regulations” OR “IHR”) on SCOPUS™, “vector-borne” AND (“international health regulations” OR “IHR”) on Web of Science™ and (“International Health Regulations” OR “IHR”) AND “Vector-borne”(Mesh) on PubMed™.
Articles and reports published in English or Portuguese were included. Studies written in other languages were identified and excluded during eligibility screening (see Table 1).
Table 1 Eligibility criteria for population, interventions, comparisons, outcomes, timing, setting, study design, and publication language
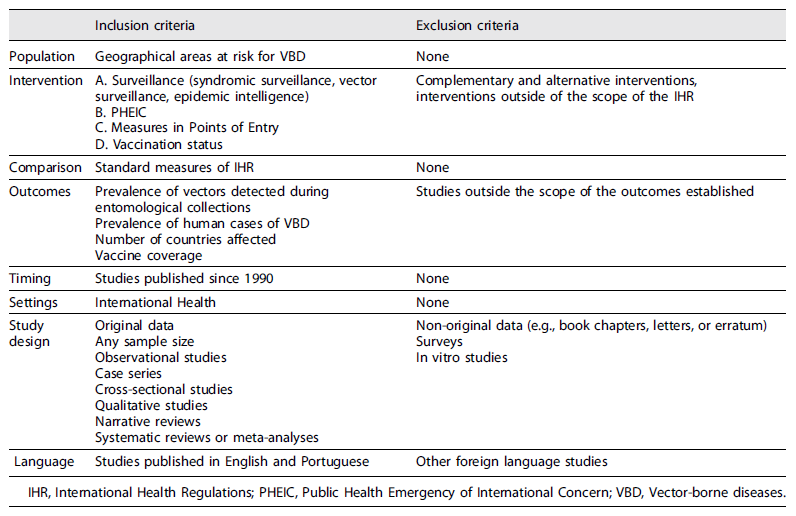
IHR, International Health Regulations; PHEIC, Public Health Emergency of International Concern; VBD, Vector-borne diseases.
The primary screening in PubMed™ yielded 60 articles, with 16 detected in SCOPUS™ and 11 in Web of Science™. All results were exported into a Microsoft Excel file. After removing duplicates, 75 results were considered. The primary screening was performed independently by two researchers and conducted on the title and abstract of each article. The answers were compared, and disagreements were discussed to solve any discrepancies through consensus or a third researcher. Articles that did not meet one or more of the inclusion criteria were excluded (n = 42). Articles that met any combination or were unclear to one of the listed criteria proceeded to secondary screening. Based on defined criteria, 33 articles were included for full-text assessment. The secondary screening was performed on the full-text articles independently by two researchers. The consensus was obtained using the same methods as on the primary screening. Full-text careful qualitative analysis was performed 8‒40, with 6 studies being excluded 9, 16, 17, 20, 29, 37. Overall, 27 articles met all the described criteria and were included in this scoping review (shown in Fig. 1).
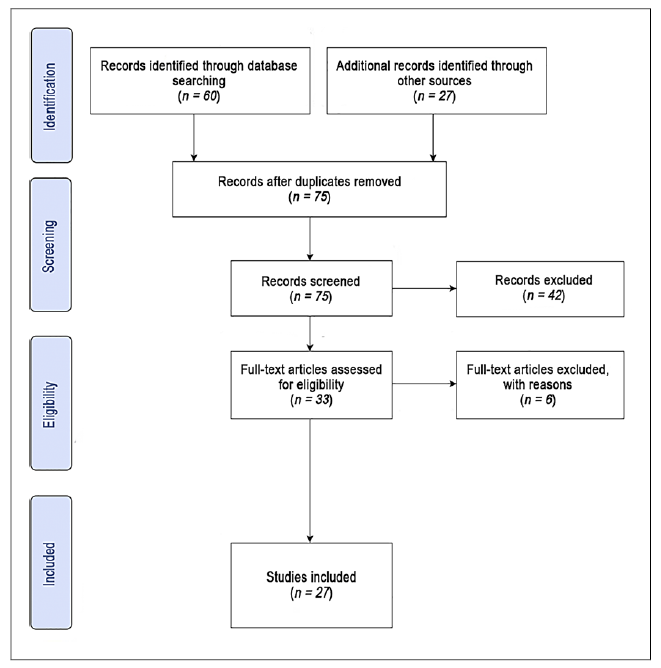
Fig. 1 Flow diagram describing the steps and number of studies selected for inclusion during the scoping review process.
For each included study, the following data were extracted:
Strategies/interventions on VBD applied in accordance with the IHR.
Effects of interventions directed toward the prevalence of human cases regarding VBD or toward the abundance of vectors.
Data related to other characteristics, study period, country of origin, study population, type of disease for which the IHR was applied.
Results
An overview of the selected articles is provided in Table 2. For each article, author, year of publication, category(ies) of IHR measures type of publication, diseases, and geographic area are indicated. A more detailed description according to each of the four IHR measures categories is highlighted in Table 3. For simplification, Table 3 lists results for the four most prevalent diseases (Yellow fever, Zika, Dengue, and Chikungunya) and groups the rest (Lyme disease, Tick-borne encephalitis, Crimean-Congo hemorrhagic fever, malaria, Japanese encephalitis, West Nile fever, and Leishmania) as others. A quotation is provided to exemplify each category.
Table 2 Overview of the selected articles included in this scoping review
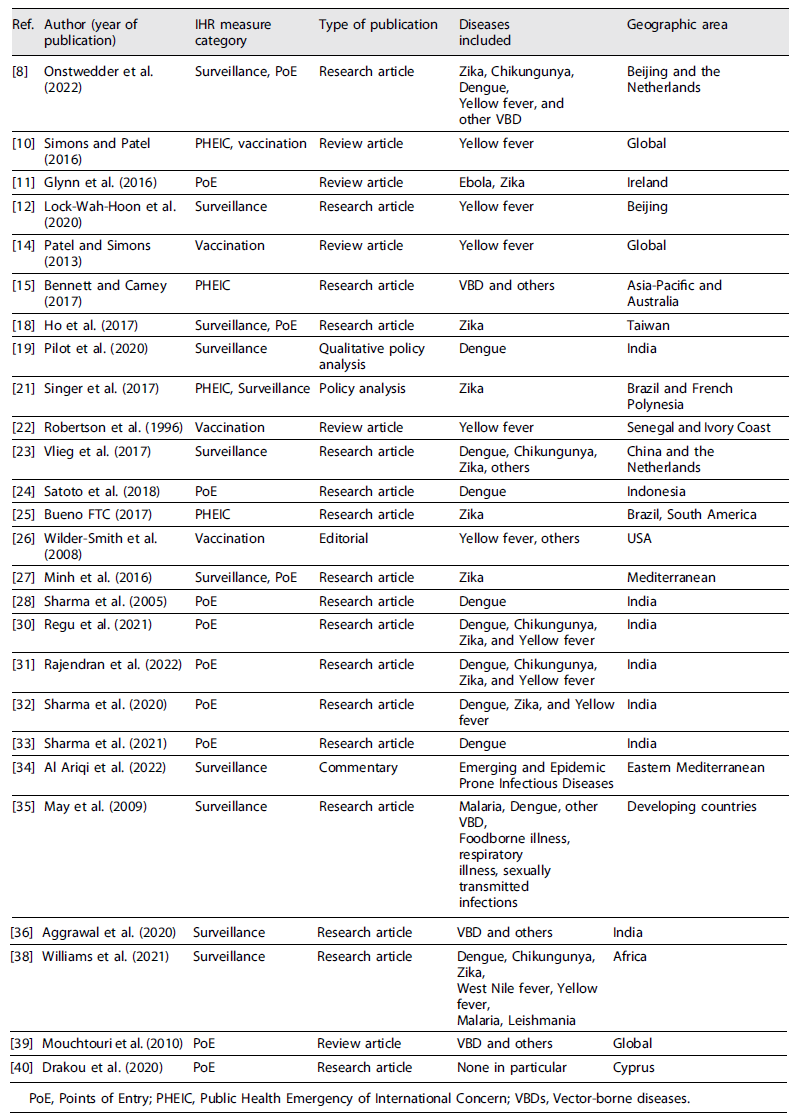
PoE, Points of Entry; PHEIC, Public Health Emergency of International Concern; VBDs, Vector-borne diseases.
Table 3 Characterization of the studies included in this scoping review
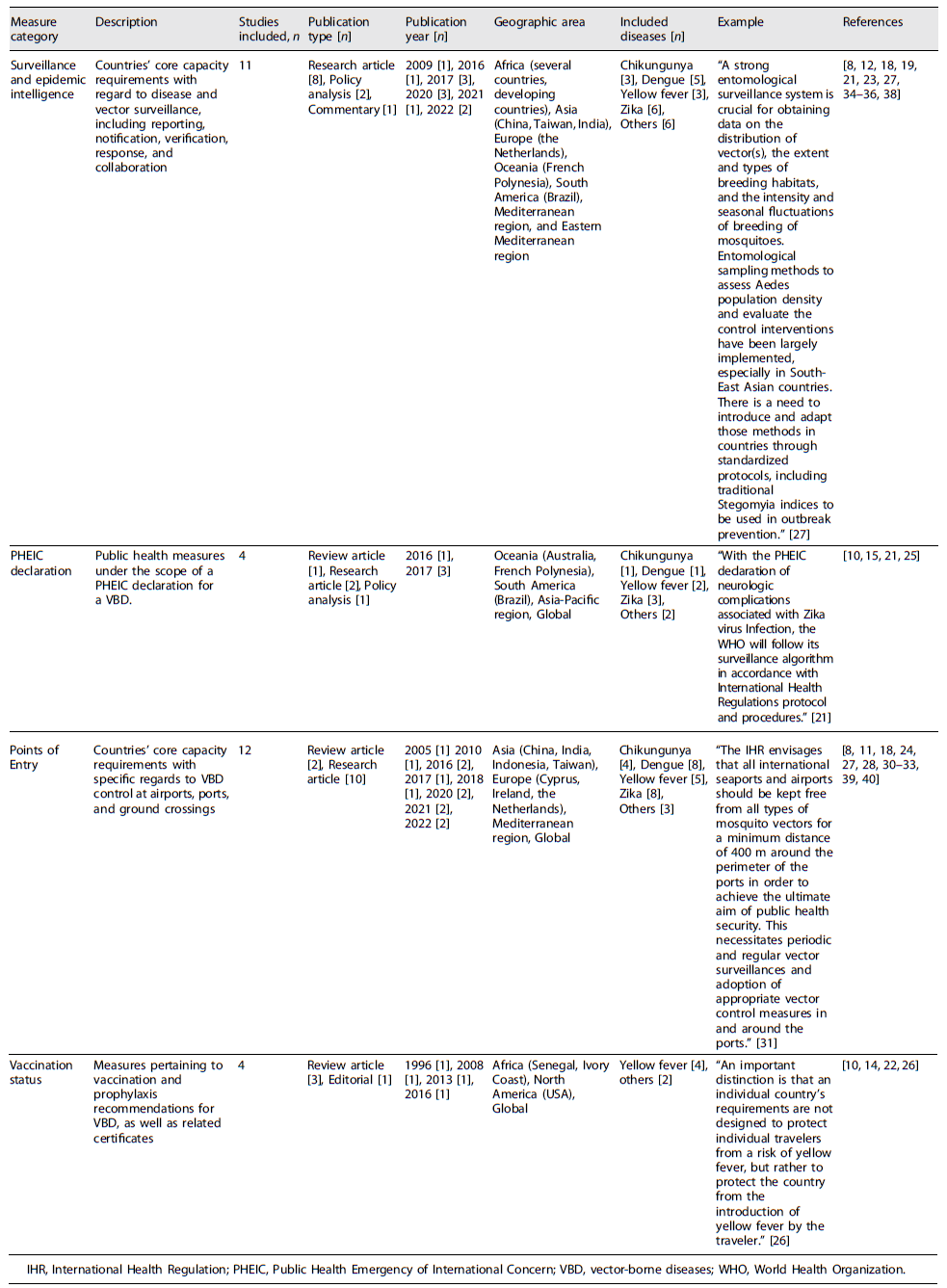
IHR, International Health Regulation; PHEIC, Public Health Emergency of International Concern; VBD, vector-borne diseases; WHO, World Health Organization.
General Characteristics of the Studies Included
Of the included articles, sixteen were research articles 8,12,14,15,17,23,25,27,30-33,35,36,38, 40, five were review articles 10,11,14,22,39, and six were other types of publications (policy analysis, commentaries, and editorial) 19,21,24,26,28,34. The year of included articles ranged from 1996 22 to 2022 8,31,34 with 74% (n = 20) being published in 2016 or after 8,10-12,15,18,19,21,23,24,27,30-34,36,38,40. Seven studies were conducted in India 19,28,30-33,36, three in China 8,12,23, three in the Mediterranean area 27,34,40, two in Brazil 21,25, two in Africa 22,38, two in the Netherlands 8,24, and two in Asia-Pacific, Australia, and French Polynesia 15,21. There was also one study from Ireland 11, one from the USA 26, one from Indonesia 24, one from Taiwan 18, and another one from several developing countries 35. Three studies/articles had no specific geographic focus 10,14,39.
Some of the articles were related to specific diseases, mainly Yellow fever 8,10,12,22,26,30-32,38, Zika 8,11,18,21,25,27,30-32,38, Dengue 8,19,24,28,30-33,35,38, and Chikungunya 8,19,24,28,30-33,35,38. All the selected articles included IHR implementation measures to strengthen prevention and response to public health events. The main categories of measures were related to surveillance (whether syndromic or vector surveillance or epidemic intelligence), Declaration of PHEIC, measures in Points of Entry (PoE, such as ports and airports), and vaccination status.
Surveillance and Epidemic Intelligence
It is emphasized in the IHR that epidemiological and syndromic surveillance of VBD is crucial to expedite national and international reporting. There are risk characterization guidelines in place for several vectors which help countries identify specific triggers for scaling up or down surveillance and public health activities, such as monitoring geographic spread and distribution and detecting changing transmission patterns or atypical clinical presentations 21. However, there have been reported operational difficulties due to barriers within countries. Among these barriers, one should consider factors such as poor data quality and poor information flow, political barriers, and weak surveillance infrastructure 12. International cooperation and sharing of best practices can be of the utmost importance for the implementation of the IHR. Comparing surveillance systems allows each country to learn valuable lessons and effectively address international challenges 8. These recommendations are in accordance with Articles 5-10 of the IHR, 2005.
Declaration of PHEIC
The Emergency Committee of the WHO may declare a PHEIC under the IHR. In May 2014 this was the case for the wild poliovirus following the acknowledgment that travelers contributed to the spread of the virus. Recommendations were made to the affected countries, and measures were taken to reduce the potential spread 10. A PHEIC declaration coordinates timelines and mechanisms for international response, including protocols for an outbreak and case limitation 21. These recommendations are in accordance with Articles 12-14 of the IHR, 2005.
Measures at PoE
The outbreak of the Ebola Virus Disease in 2014-2015 and the emergence of Zika in 2016, both considered PHEIC, provided an impetus for countries to review their PoE preparedness 11. Given the rapid global growth of human connectivity, the entry and establishment of VBD in seaports and airports pose a potential threat of disease outbreaks and epidemics. To address this, the IHR recommends sanitary standards at international borders and PoE, including knowledge awareness for PoE authorities, early detection of potentially infected persons, dissemination of health information for travelers and protocols for assessment and case management 11. Vector surveillance at these sites includes specific parameters. For instance, the IHR specifically states that if specific vectors are found within a 400-m range of PoE sites, public health authorities must be notified so that control measures may be applied 8,31,32. These recommendations are in accordance with Articles 19-29 of the IHR, 2005.
Vaccination Status
Some VBD are vaccine-preventable. Yellow fever is one of those examples. This vaccine can be recommended for personal protection or it may be a mandatory requirement for entry into certain country. The WHO keeps a record of the at-risk countries and the national requirements for entry. As proof of vaccination under the IHR, an International Certificate of Vaccination or Prophylaxis (ICVP) is issued at the time of vaccination 10. Policymakers at a national level are sometimes faced with the lag that happens between new scientific evidence and the lack of concurrent amendments to the IHR, such as with the shift from the 10-yearly revaccination to the declaration of life-long protection from a single dose of the Yellow fever vaccine. Nevertheless, risk assessment and risk management should always be considered by health practitioners 12. The implementation of the IHR and the ICVP is crucial to prevent the international spread of infectious diseases and for the coordinated global response to public health events 26. These recommendations are in accordance with Articles 18, 23, and 31 of the IHR, 2005.
Discussion
Literature reviews play a significant role in healthcare practice. Evidence-based practice is gaining recognition as the benchmark for care 6. Consequently, reviews of primary research are becoming more frequent as a useful tool for researchers, clinicians, and decision-makers. Scoping reviews are a relatively new methodology, generally performed to synthesize research evidence, and clarify definitions and conceptual boundaries within a determined field or topic, particularly when the body of certain literature has not yet been comprehensively reviewed. They allow one to perform a summary of research findings (quantitative and/or qualitative), identify research gaps, and make recommendations for future research topics.
The perceived strengths of a scoping review are the characteristics they share with the systematic reviews, namely their systematic, replicable, and transparent methodology. On the other hand, the perceived weaknesses and limitations of scoping reviews are the fact that they cannot be regarded as a final output due to potential limitations in their rigor and duration. Typically, they do not include a process of quality assessment, and consequently, there is the risk of including studies by their existence and not exactly by their intrinsic quality. Subsequently, their findings cannot be used to recommend policy/practice, as a formal assessment of the methodological quality of the included studies is generally not performed 7.
Overall, this scoping review stresses the relevance of IHR in a world increasingly susceptible to VBD. It is expected that VBD outbreaks will become more common and that new PHEIC will be declared as a result of climate change, globalization, tourism, and increased movement of goods across international borders. This will require a high level of preparedness from all countries, which should ensure that their core capacities are updated and robust.
Vaccination is the mainstay for the prevention of events caused by vaccine-preventable VBD (e.g., Yellow fever), and the main purpose of requiring travelers to be vaccinated is for public health benefit, i.e., to prevent the introduction of the pathogen in the destination country 10. There is potential for improvement in keeping the IHR in accordance with the best available evidence and allowing the law to reflect the best clinical practice 14.
The formal declaration of a PHEIC constitutes an important tool for international cooperation and coordinated response to events and allows the countries to follow procedures already in place for incident response. There are, however, other interests influencing the implementation of the IHR and a general need to strengthen and build capacity in the institutions responsible for responding to public health threats at a national, regional, and global level 15. State Parties do not always follow WHO recommendations with regard to a PHEIC, such as when countries like Russia and China ceased pork meat imports from countries affected by Influenza H1N1 in 2009, despite no evidence linking pork to the pathogen. Likewise, several countries imposed considerable travel barriers contrary to WHO guidelines during the Ebola outbreak in 2014, with the USA, for example, applying 21-day quarantines on healthcare workers returning from afflicted countries 15. Modifications to the formal processes described in the IHR may also be relevant to respond to specific and emerging threats in a scalable, adaptable, and flexible way 21.
Surveillance and epidemic intelligence are mandated by the IHR as important tools for the early detection of outbreaks. Syndromic surveillance extends the detection capability beyond confirmed cases of specific diseases characteristic of typical epidemic surveillance and should be built on existing public health surveillance infrastructure 35. Across countries, epidemic surveillance varies in capabilities according to the resources available to each country and is not uniformly applied. For example, clinical surveillance in mass gathering events enables early disease detection and response 36 as well as provides early detection, even if the causative agent is yet unknown 35. Comparing surveillance systems allows each country to learn valuable lessons. Nevertheless, differences in preparedness and response are rooted in specific national VBD epidemiology and surveillance structure. China, for instance, relies on syndromic surveillance first, while the Netherlands focus on laboratory-confirmed diagnosis 8.
Vector surveillance at PoE encompasses the most common implementation measures found in literature, with clear standards required by the IHR. These provide early warnings for the introduction of vectors or diseases at critical points (e.g., airports and seaports) 30-32.
An important gap found in the literature that runs across different studies is the systematic underinvestment in the necessary infrastructure to conduct the activity required to uphold the IHR. From lack of dedicated transport for field teams to insufficient information technology IT equipment, underfunded laboratories, and not enough human resources, or financial support to conduct surveillance activities, there is a clearly identified need to strengthen the institutions responsible for the implementation of the IHR at all levels of governance. This systemic lack of investment inevitably leads to marked differences in the implementation of the IHR across countries, with North America and Europe investing more heavily in syndromic surveillance. Member states of the WHO African and Southeast Asia regions, on the other hand, face logistical, human, and financial challenges that countries from richer regions do not face, which can undermine efforts to adequately respond to such threats 15,38.
Thus, this scoping review highlights the persistent and stark asymmetries between countries with regard to the full implementation of IHR. The fact that most of the vector-borne pathogens are endemic to the global south may be a limitation to the scope of this review. Moreover, the restriction of sources to the English and Portuguese languages may explain the relative lack of coverage of certain geographic regions, such as Southeast Asia. This could also be a reason why India is overrepresented in the literature selected in this review.
To conclude, this scoping review offers a summary of research findings regarding the implementation of the IHR to control the occurrence and transmission of VBD worldwide. To the authors’ knowledge, this review represents the first assessment of available literature on this topic, as the implementation of the IHR on VBD has not yet been comprehensively reviewed. Indeed, the relative lack of robust, systematic literature found on this topic is cause for alert. The IHR measures are inconsistently referenced across pathogens, diseases, countries, and continents, often with different outcomes and reporting standards. Whether concerning surveillance, vaccination status, PoE, or PHEIC declaration, the IHR effectively lays the groundwork, albeit in need of a careful revision, and those tools and know-how should be approached in a consistent, responsible way, regardless of location and politics. Considering global phenomena, like climate change, and the consequent increasing spread of vectors and VBD to new geographical areas (especially higher latitudes and altitudes), adopting IHR is essential to ensure the highest level of protection against the spread of diseases with the least amount of disruption to the global movement of goods and people.
Further studies should focus on the preparedness level of countries in the northern hemisphere, as they are likely to face an increased risk of VBD outbreaks. Specifically, surveillance systems should not only reflect the recommendations stated by the IHR but must allow for a flexible and continuous flow of information across borders, so that an international response can quickly and effectively be implemented between governments.
The continued relevance of the IHR was widely acknowledged during the COVID-19 pandemic, an event that strained State Parties’ core capacities to their limits and allowed for successes and shortcomings of the IHR to be better identified. The continued sense of urgency regarding recent outbreaks of Poliomyelitis, Dengue, Malaria, and Ebola, as well as the unavoidable recognition of the interdependency of nations regarding their populations’ health, should be the driving force behind an effective implementation of IHR measures.

