











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
PermalinkIntroduction
Health professionals are known to be disproportionally affected during public health emergencies 1), (2),(3. In the COVID-19 pandemic, they represent a non-negligible proportion of all cases 4), (5), (6), (7), (8. Particularly in the early phase of the pandemic, the risk of exposure and transmission to health professionals has been fuelled by uncertainty around the characteristics of this new virus, prolonged and close exposure to patients, inadequate use of personal protective equipment (PPE), sudden increased workload, and shortages of PPE 9), (10), (11), (12), (13), (14), (15. In Portugal, health professionals evaluated themselves at high risk and estimated to be poorly prepared to respond to the COVID-19 pandemic 16.
While studies that investigate the burden of the COVID-19 pandemic on health professionals and risk factors associated with SARS-CoV-2 infections in health professionals have multiplied over the past year of the pandemic, few have addressed the risk to health professionals compared to the general population. It was suggested that infections in health professionals followed the same trends as in patients 17. Transmission probability in the primary care setting, characterized by short periods of contact with patients, was also estimated to be lower than transmission in household settings with prolonged close contacts, and to be efficiently addressed by adequate use of PPE 18. Furthermore, despite a higher risk associated with specific care 19, various studies showed that the proportion of cases did not differ significantly between health professionals providing care and non-medical staff 17), (20. Yet, in a cohort study conducted in the UK 21, healthcare workers were found to be at a 7-fold higher risk of severe COVID-19 compared to other occupational groups classified as non-essential workers.
In Portugal, the risk of COVID-19 in health professionals compared to those who are not health professionals have not been well described. We conducted a test-negative case-control study using national surveillance data to estimate the risk of COVID-19 in health professionals compared to non-health professionals.
Materials and Methods
Study Design
We conducted a test-negative case-control study to assess whether being a health professional was associated with a positive COVID-19 test. The test-negative case-control study design follows the same principle as a standard case-control study but differs in the way cases and controls are selected 22. Indeed, cases are individuals who test positive for the outcome (i.e., SARS-CoV-2), whereas controls are individuals who are also tested but with a negative result. The study population is not necessarily representative of the whole population of cases (e.g., mild or asymptomatic cases are less likely to be tested), but both confirmed cases and negative cases belong to the same source population with similar factors and criteria leading them to be tested. Indeed, testing rates are expected to be similar among cases and controls, since the “selection forces” (i.e., testing criteria, access to test, etc.) apply consistently to all individuals who undergo testing. By its very nature, the test-negative case-control design provides relevant insights for the epidemiological knowledge and public health practice, while reducing the costs, data-collection efforts, and duration associated with other types of studies 23.
Setting
The first confirmed case of COVID-19 was reported in Portugal on March 2, 2020, and the first peak occurred on March 23-25, 2020. From January 2020, a case-report form was available through the electronic platform of the National Epidemiological Surveillance System (SINAVE). A confirmed case was an individual with a positive test (RT-PCR) for SARS-CoV-2, independently of clinical presentation.
Study Population
The study population comprised all notifications with a laboratory result reported through SINAVE between January 27 and June 6, 2020. We excluded notifications of individuals <18 years or >69 years old to retain the main working-age groups. Observations without information on the health professional status were excluded (n = 11,264, 7%), as well as observations with missing data on any of the other variables of interest (n = 82,885, 63%).
Variables
The variables of interest were those reported in the case-report form from SINAVE. The primary exposure was health professional/non-health professional status. Health professional designates any professionally active worker in the health sector, including medical and non-medical staff who provide care (e.g., doctors, nurses, auxiliaries, etc.) or not (e.g., pharmacists, health technicians, radiologists, etc.), and other professionals in healthcare settings (e.g., security guards, cleaners, receptionists, etc.).
The other variables of interest were demographic and geographical characteristics, clinical presentation, and epidemiological characteristics. Demographic and geographical characteristics were sex, age groups, and region. The clinical presentation referred to the clinical signs or symptoms at the time of notification, classified in two categories: “main symptoms” that designates any of the symptoms of the testing criteria (i.e., fever and/or cough and/or shortness of breath and/or acute respiratory distress), and “other symptoms” when none of the main symptoms was reported but any other symptoms from the list of symptoms available in the case-report form (e.g., runny nose, odynophagia, headache, abdominal pain, chest pain, joint pain, muscular pain, nausea/vomiting, diarrhoea) or no symptoms at all. The epidemiological characteristics were international travel history during the potential incubation period (i.e., 14 days before symptoms onset, or before testing if no symptoms), and self-reported epidemiological link (i.e., self-reported contact with a COVID-19 case or a person with COVID-19-like symptoms). The variables are further described in the online supplementary material 1 (for all online suppl. material, see www.karger.com/doi/10.1159/000519472).
Data Collection
Pre-processed data were extracted from SINAVE on June 22, 2020. They consisted of de-duplicated medical and laboratory notifications for each individual, such that only one record per individual was kept even if multiple tests were conducted during the study period. More precisely, the data contained the record associated with the first positive laboratory result (if any), or the most recent negative result (if no positive test result was ever reported). Consequently, an individual could only be counted once in the study as either a case (at least one positive test result) or a control (only a negative test result).
Statistical Analysis
We performed χ2 tests to investigate the difference in the distribution of health professionals, demographics, and clinical and epidemiological characteristics among cases and controls (p < 0.05). We used a multivariable logistic regression model to estimate the odds ratio and 95% confidence interval of a positive COVID-19 test (primary outcome) in health professionals compared to non-health professionals (primary exposure), adjusted for age, sex, region, symptoms, international travel history, and with an interaction term for the self-reported epidemiological link. The covariates included in the analysis were considered based on prior knowledge of COVID-19 epidemiology and potential confounders. We adopted a stepwise backward selection method, including all these relevant covariates at the start of the analysis, and removing successively the non-significant covariates, if any.
To further assess the robustness of our findings, we conducted a sensitivity analysis with different health professional groups (i.e., doctors, nurses, clinical support staff, health technicians [including first responders/paramedics], administrative staff, and unspecified occupation) compared to non-health professionals (see online suppl. material 2).
Results
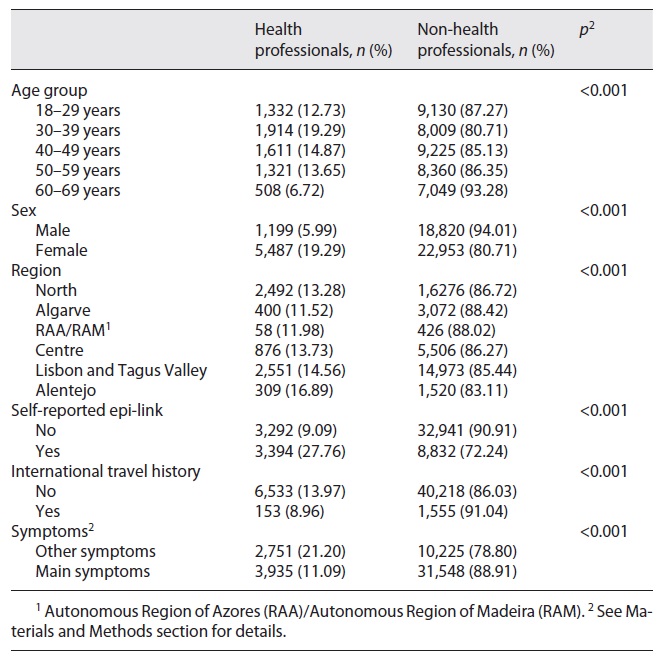
A total of 48,459 observations were included, of which 6,611 (13.64%) were confirmed cases. Health professionals represented 6,686 (13.80%) of all observations, and 20.27% of all confirmed cases (Table 1). The proportion of cases was higher in health professionals (20.04 vs. 12.62%, p < 0.001). The sex distribution was different between cases and controls (p = 0.013), although the difference was negligible (cases were 14.10% among men and 13.32% among women). Age groups were unequally distributed (p < 0.001), with the highest proportion of cases among 50-59 year olds. An epidemiological link and international travel history were associated with cases: 29.32% of individuals with an epidemiological link and 19.91% with travel history tested positive (p < 0.001). The proportion of cases was slightly higher among individuals with symptoms other than the main symptoms (15.81 vs. 12.85%, p < 0.001).
Table 1 Univariable associations between the health professional status and variables of interest, Portugal, January to May 2020
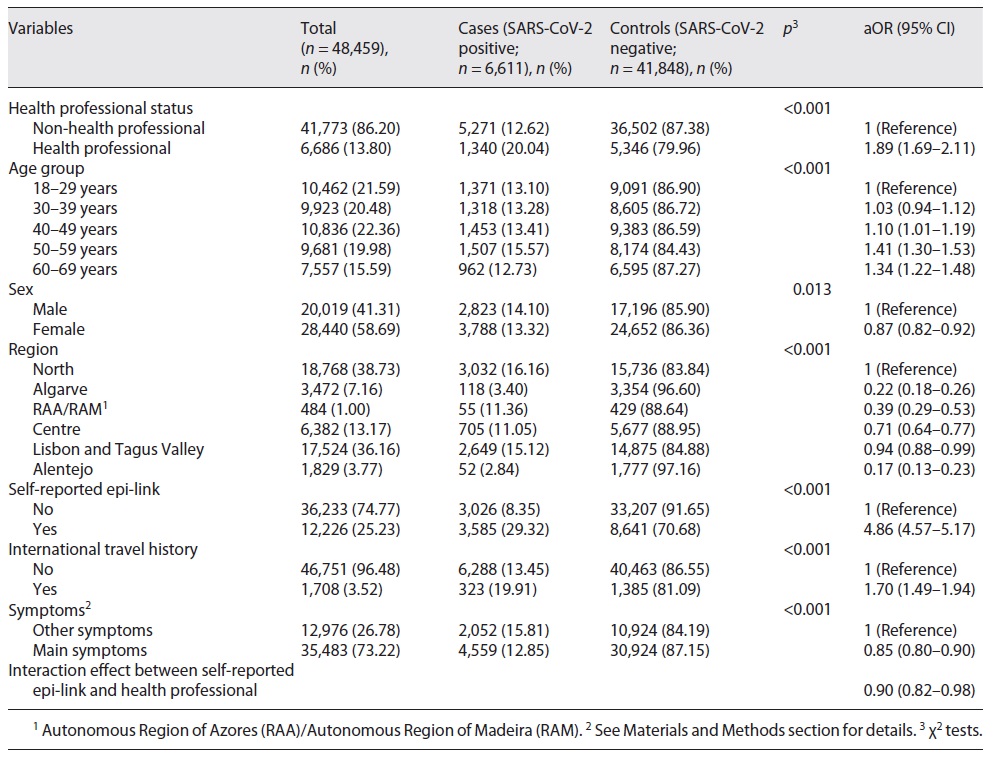
In the crude analysis, health professionals were significantly more likely to have had a positive COVID-19 test (OR = 1.74, 95% CI 1.62-1.86). The final model retained all covariates, controlling for the confounding effect of age, sex, region, travel history, symptoms, and the modification effect of the self-reported epidemiological link (Table 2). Health professionals were still strongly associated with a positive COVID-19 test (aOR = 1.89, 95% CI 1.69-2.11). However, this association was modified by the self-reported epidemiological link such that, among cases who did report an epidemiological link, being a health professional appeared significantly protective (aOR = 0.90, 95% CI 0.82-0.98). Findings from the sensitivity analyses were consistent with the previous observations, except results for administrative staff were non-significant due to the small strata sample size (<10% of health professionals; online suppl. material 2).
Table 2 Results of the multivariable model measuring the association between health professional status and SARS-CoV-2 test positivity adjusted for age groups, sex, region, international travel history, symptoms, and with interaction between health professional status and self-reported epidemiological link, Portugal, January to May 2020 (n = 48,459)
To further assess the impact of missing data in our analysis, we compared the proportion of observations with missing data between cases and controls, and between health professionals and non-health professionals. The variables with missing data were the self-reported epidemiological link (37.01% of observations), symptoms (30.29%), and international travel history (2.45%). However, the differences in the overall proportion of observations with missing data between cases and controls (62 vs. 67%) or between health professionals and non-health professionals (61 vs. 72%) were relatively small, although statistically significant (p < 0.001), which is expected with such a large sample. The larger differences were observed for the “symptoms” variable, with a higher proportion of health professionals with missing data compared to non-health professionals (47 vs. 27%; online suppl. material 3).
Discussion
To our knowledge, this is the first study assessing the risk of COVID-19 in health professionals compared to non-health professionals in Portugal. In this study, we found that the proportion of confirmed cases in health professionals was double that of non-health professionals. After controlling for demographics and clinical and epidemiological confounders, we found that health professionals had a 2-fold higher risk of a positive COVID-19 test result, but this association was strongly modified by the self-reported epidemiological link. Indeed, among cases that did report an epidemiological link, being a health professional was a protective factor.
The higher risk of COVID-19 test positivity in health professionals is consistent with findings from other settings that reported a higher risk in essential workers 21. In this regard, it is worth noting that half of the health professionals reported an epidemiological link, whereas only 20% of non-health professionals did so. Considering that the proportion of self-reported epidemiological links could be a proxy for the opportunities of exposure, this supports the idea of a higher exposure of health professionals due to the nature of their profession.
However, the protective effect of the health professional status among cases who did report an epidemiological link appears counter-intuitive. Eventually, our results suggest that health professionals might be primarily infected by unknown contacts and that the occupational exposure of health professionals does not systematically translate into a higher risk of transmission. We discuss here some hypotheses to support the interpretation of these results.
First, the nature of contacts of health professionals might be different to that of non-health professionals and can yield different probabilities of transmission. In our study, the majority (87%) of health professionals reported an epidemiological link in healthcare settings, whereas half (47%) of non-health professionals referred to household contacts. Exposure in a household setting is likely to be characterized by a higher frequency, duration, and proximity with household contacts, which in turn might translate into a higher probability of transmission. In contrast, exposure of health professionals in healthcare settings might be of shorter duration and limited proximity with patients.
Most importantly, the timing of exposure might differ in household or healthcare settings. Indeed, exposure in household settings is likely to occur before knowing that the contact person is infected by COVID-19, and thus before any preventive measure can be taken (e.g., isolation, mask use, etc.). In contrast, exposure of health professionals in healthcare settings is likely to happen after a confirmed or suspected diagnosis of COVID-19 of the said contact person, and it is plausible to believe that the IPC (implementation of infection prevention and control) measures would explain the reduced risk in health professionals who reported an epidemiological link 24), (25. These measures include the use of masks and respiratory etiquette, which was generalized to all health professionals in a hospital or primary care setting on March 29, 2020 26, and the use of PPE, which followed recommendations by type of care (i.e., non-invasive or invasive care) and contact with patients 27,28. It is worth noting that during the study period no specific recommendations or legal obligations regulated the use of facemasks in the community.
Finally, the difference in risk for health professionals who did not report an epidemiological and those who did report an epidemiological link might also be interpreted as a proxy or as different risk perceptions and associated individual behaviours. In other words, health professionals who did not report an epidemiological link might have failed to identify a situation at risk of exposure and might have not used appropriate preventive measures, which would eventually translate into a higher risk of transmission.
This study has some limitations. The low completeness of the case-report forms, which lead to a high number of exclusions of observations, was an important issue. Complete case analysis was still preferred, based on the following considerations. First, due to the standardization of the reporting process and a large amount of data, we do not have any reasons to believe that there might be systematic differences in completeness or misclassifications of the variables of interest that would significantly affect the results. Additionally, medical case-report forms of suspected cases that contain information on the variables of interest (i.e., demographics, clinical presentation, travel history, and self-reported epidemiological link) are generally filled before knowing the laboratory result. Consequently, it is unlikely that the test outcome would have biased the reporting of the variables of interest leading to systematic differences between cases and controls. Despite this, one cannot completely exclude reporting bias between health professionals and non-health professionals. For instance, physicians could be more likely to report that a suspected case is a health professional or that a health professional has had contact with a COVID-19 case (self-reported epidemiological link). The analysis of the proportion of observations with missing data revealed minor differences between health professionals and non-health professionals. The larger differences observed for the “symptoms” variable, with health professionals having a higher proportion of missing data, could reflect a higher likelihood for health professionals to be reported as suspected cases, independently of symptoms or signs. Another hypothesis relates to the presence of lighter or atypical symptoms that were not included in the medical case-report forms in the early months of the epidemic, such as anosmia or ageusia. Such symptoms were also more prevalent in younger patients, and active health professionals being younger than non-health workers would have been more likely to experience those.
The validity of the test-negative case-control design relies on the assumption of a similar testing rate among participants 22), (23. Here we present arguments in favour of such an assumption. First, Portugal rapidly developed a high testing capacity. Laboratories, including hospital laboratories, private laboratories at universities and research centres, and other laboratories, were subjected to an expedited process of central authorization to qualify for the diagnosis of SARS-CoV-2. Despite a relatively limited number of authorized sites at the beginning of the pandemic, the list of authorized laboratories quickly scaled up in the country. Additionally, access to testing was facilitated by the multiplication of testing points and the removal of financial barriers as tests for suspected cases were fully subsidized by the NHS. This led to an early increasing and sustained high testing rate per capita 29),(30), (31 (online suppl. material 4)
Health professionals were encouraged to perform a daily self-monitoring of a limited set of symptoms suggestive of COVID-19 (e.g., fever, odynophagia, cough, rhinorrhoea, shortness of breath) 27. Thus, it is plausible that suspected and confirmed COVID-19 cases among health professionals would have been identified more promptly 32. Additionally, it is reasonable to believe that testing was performed more frequently among health professionals to prevent and control outbreaks among a highly exposed and/or vulnerable population in healthcare settings (i.e., health workers, patients). As such, we cannot exclude that asymptomatic cases would be more likely detected among health professionals, which would tend to slightly overestimate the effect of the health professional status on a positive test result. Nevertheless, at that time, there were no mandatory requirements of testing, neither a national strategy nor framework for testing of health professionals. Moreover, similar punctual testing strategies would have also occurred in other settings (e.g., comprehensive testing of company staff where a COVID-19 cluster was detected).
Finally, such a study design based on surveillance data has some limitations and we do not pretend to replace research studies that are based on a random sampling of the population and provide robust population estimates. It does, however, contribute to the effort to use and disseminate surveillance data to improve the epidemiological understanding and public health practice in the context of the COVID-19 pandemic response.
To our knowledge, this is the first study estimating the risk of COVID-19 in health professionals in Portugal. Efforts should be pursued to better protect health professionals who are working at the frontline of the COVID-19 response. Future research is needed to further investigate the risk differences between various occupational groups of health professionals, and their evolution over time concerning the epidemic dynamics and changes in preventive measures and policies, both in healthcare settings and the general population.
Acknowledgements
We acknowledge the hard work of all frontline workers and public health professionals involved in the response to COVID-19 in Portugal at the national, regional, and local levels, particularly the physicians and laboratory workers who participate in the surveillance, and the Directorate-General of Health COVID-19 Task-Force members. We thank Dr. Rodrigo Marques for his contribution to data collection. We extend our appreciation to Porto Public Health Institute (ISPUP) COVID-19 Task-Force for constructively criticizing this study.
Statement of Ethics
Pre-anonymized data were collected in the scope of national epidemiological surveillance, requiring no supplementary ethical approval by institutional bodies and preserving the confidentiality and anonymity of individuals. The study was in line with the World Medical Association Declaration of Helsinki.

