










Services on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkGE-Portuguese Journal of Gastroenterology
Print version ISSN 2341-4545
GE Port J Gastroenterol vol.27 no.2 Lisboa Apr. 2020
https://doi.org/10.1159/000502359
CLINICAL CASE STUDY
Ruptured Hemorrhagic Hepatic Cyst: An Unusual Case Report
Quisto hepático complicado por ruptura e hemorragia: um caso raro
Maria João Amarala, Marco Serôdioa,c, Maria João Kocha, Rui Almeidab–d, José Carlos Camposa, José Guilherme Tralhãoa,c,e
aGeneral Surgery Unit, Centro Hospitalar e Universitário de Coimbra, Coimbra, Portugal; bAnatomical Pathology Unit, Centro Hospitalar e Universitário de Coimbra, Coimbra, Portugal; cFaculty of Medicine, University of Coimbra, Coimbra, Portugal; dInstitute of Anatomical and Molecular Pathology (IAP-PM), Faculty of Medicine, University of Coimbra, Coimbra, Portugal; eCoimbra Institute for Clinical and Biomedical Research (iCBR) Area of Environment Genetics and Oncobiology (CIMAGO), Faculty of Medicine, University of Coimbra, Coimbra, Portugal
* Corresponding author.
ABSTRACT
Background: Hemorrhagic rupture of a hepatic cyst is rare. To date, very few cases have been reported in the literature. Case Report: A patient with a history of a suspected liver hydatid cyst presented to the emergency department with abdominal pain and fever. She was admitted with the presumptive diagnosis of acute cholecystitis. During hospitalization, the patient presented with hemodynamic instability and abrupt worsening of the abdominal pain. The abdominal angio- chemotherapy scan showed an abundant free peritoneal effusion and an apparent effacement of the anterior wall of a hepatic cyst of 16 cm. The patient underwent an exploratory laparotomy, deroofing of the cyst, and peritoneal lavage. The anatomopathological results showed a simple hepatic cyst. Discussion: Hemorrhagic rupture of simple hepatic cysts is a life-threatening complication and, although rare, should be included in the differential diagnosis of sudden abdominal pain in patients with a history of simple hepatic cysts.
Keywords: Hepatic cyst, Rupture, Abdominal pain, Peritoneal effusion, Surgery
RESUMO
Introdução: A ruptura hemorrágica de um quisto hepático é rara. Até à data, foram descritos poucos casos na literatura. Relato de caso: Uma doente com antecedentes de um provável quisto hidático hepático recorreu ao serviço de urgência por dor abdominal e febre. Foi internada com o diagnóstico presumível de colecistite aguda. Durante o internamento, a doente iniciou um quadro de instabilidade hemodinâmica e agravamento súbito da dor abdominal. A angio-TC abdominal revelou um volumoso derrame peritoneal livre e uma aparente efração da parede anterior de um quisto hepático com 16 cm. A doente foi submetida a uma laparotomia exploradora, excisão da cúpula saliente do quisto e lavagem peritoneal. O exame anatomopatológico foi concordante com um quisto hepático simples. Discussão: A ruptura hemorrágica de quistos hepáticos simples é uma complicação com risco de mortalidade, e, embora rara, deve ser incluída no diagnóstico diferencial de abdómen agudo em doentes com história de quistos hepáticos simples.
Palavras-Chave: Quisto hepático, Ruptura, Dor abdominal, Derrame peritoneal, Cirurgia
Introduction
Most simple hepatic cysts are benign and incidentally diagnosed, with an estimated prevalence ranging from 2.5 to 4.7% [1]. They occur more frequently in females, and their prevalence increases with age [2]. Hepatic cysts are usually solitary and asymptomatic, although larger ones may cause discomfort or abdominal pain [3], abdominal distension, nausea, vomiting, anorexia, and dyspnea [4]. Polycystic liver disease should be considered when the number of cysts is higher than three [2]. These cysts may have complications such as compression of adjacent organs in 3–9% of the cases, intracystic hemorrhage in 2–5% of the cases, infection in 1% of the cases, and, rarely, intra- or extraperitoneal cystic rupture [1].
We present the rare case of hemorrhagic rupture of a 16-cm simple hepatic cyst.
Case Report
A 72-year-old female was admitted to the emergency department following 24 h of abdominal pain in the right quadrants, heartburn, and fever. She had a history of a suspected liver hydatid cyst (diagnosed about 5 years before, only by ultrasound), cholelithiasis, paroxysmal atrial fibrillation, and arterial hypertension, being medicated with apixaban and nebivolol. Physical examination revealed a soft but distended abdomen, with tenderness and guarding in the right upper quadrant, with a palpable phlegmon. Abdominal ultrasound showed a massive hepatic cystic formation, with echogenic content and solid-looking areas but without internal vascularity in Doppler mode, as well as another smaller cyst in the left lobe of the liver, adjacent to the first one; gallstones, sludge, and a small amount of peritoneal effusion were also found. To better clarify the clinical scenario, an abdominal computed tomography (CT) was performed and confirmed a cystic formation of about 16 cm in hepatic segment 4, with a discrete heterogeneous content and dense areas not suggestive of an abscess, and a leftlobe cyst of about 6 cm; the CT also confirmed cholelithiasis and peritoneal effusion. Biochemical blood analyses revealed a hemoglobin level of 11.7 g/L (n.v. 12–16), normal liver enzymes, a bilirubin level of 1.3 mg/dL (n.v. 0.2–1.2), 11.900 leukocytes/mm3 (n.v. 4–10), and a C-reactive protein level of 18.4 mg/dL (n.v. < 0.5). With the presumptive diagnosis of acute cholecystitis, a decision for conservative treatment was made, and the patient was admitted under empirical antibiotic therapy with piperacillin-tazobactam.
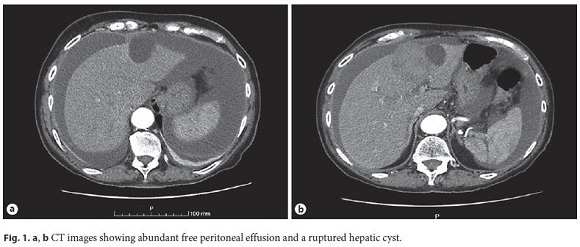
On the third day of admission, the patient presented with hemodynamic instability and abrupt worsening of the abdominal pain. The pain was generalized, and there was rebound tenderness. Therefore, the patient was submitted to a new abdominal angio-CT scan (Fig. 1) that showed an apparent effacement of the anterior wall of the larger cyst with an extension of about 1 cm, adjacent to which there was a contrast-enhanced area that was accentuated in the portal phase; an abundant, free peritoneal effusion, calcified cholelithiasis, and a small-volume bilateral pleural effusion were also observed. Blood tests showed a hemoglobin level of 9.5 g/L, an international normalized ratio of 1.32, and a C-reactive protein of 21.1 mg/dL.
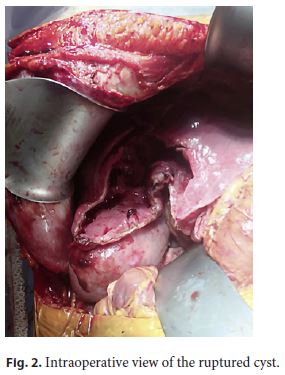
Faced with this worsening clinical state, the patient underwent an exploratory laparotomy with a reverse L incision. A large hemoperitoneum and the ruptured cyst were found, and, although not actively bleeding, it was unroofed (Fig. 2). A cholecystectomy and peritoneal lavage and drainage completed the intervention. The postoperative course of the patient was uneventful, and she was discharged on the fifth day of hospitalization with hemodynamic stability and without fever or any pain complaints.
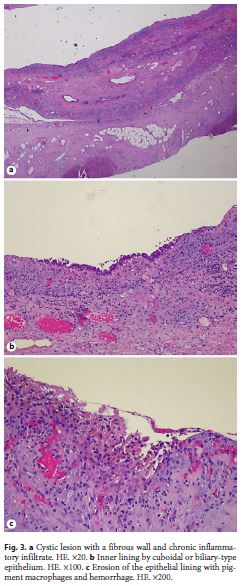
The anatomopathological examination showed a simple biliary cyst and cholelithiasis (Fig. 3).
Follow-Up
After discharge, the patient began follow-up with periodic ultrasound and blood biochemistry. About 1 year after admission, the abdominal ultrasound revealed only the already known homogeneous hepatic cystic formation, with about 6 cm of greater diameter.
To this date, the patient does not present any symptoms, and all her blood tests are within normal values.
Discussion
Intracystic hemorrhage, typically benign, has no biological consequences and may not be clinically detected. When it causes abdominal pain and imaging tests are performed, in rare cases, it may be difficult to distinguish this condition from a cystadenoma or a cystadenocarcinoma [1, 5]. On the other hand, cystic ruptures, which are rarer, are associated with an increase in volume of the cyst or with infection, which weakens its wall. The association of cystic hemorrhage with rupture is the rarest complication of hepatic cysts [1], and, to date, very few cases have been reported in the literature.
The pathogenesis of this complication is not yet clearly established [1], but bleeding that would increase the tension within the cyst would probably precede the rupture [6]. In the present case, the main risk factor identified for the hemorrhage was the chronic oral anticoagulant treatment.
In earlier reviews of the literature, it has been shown that hemorrhagic ruptures of simple hepatic cysts can be particularly severe [1]. Consequently, in case of hemodynamic instability that could lead to the death of patients, an emergent surgical intervention may be necessary. Asymptomatic cysts do not require treatment. Even larger cysts can be monitored by image examinations and, if left unchanged for 2 consecutive years, monitoring can be suspended. In case of complications, therapeutic options include conservative treatment, CT-guided needle aspiration with or without the injection of a sclerosing agent, internal drainage with cystojejunostomy, laparoscopic or open wide deroofing, liver resection, and liver transplantation [6].
Deroofing is a safe and definitive treatment for simple hepatic cysts. In the case of laparoscopic deroofing, the recurrence rate is low (0–20%), and the morbidity rate is almost 0%. More radical approaches such as complete excision of the cyst or a hepatectomy significantly increase morbidity and are almost unacceptable in patients with benign diseases, although the recurrence rate is 0% [6].
Conclusion
Hemorrhagic rupture of simple hepatic cysts is a lifethreatening complication and, although rare, should be included in the differential diagnosis of sudden abdominal pain in patients with a history of simple hepatic cysts. Rupture of such cysts may require surgical intervention.
References
1 Marion Y, Brevartt C, Plard L, Chiche L. Hemorrhagic liver cyst rupture: an unusual life-threatening complication of hepatic cyst and literature review. Ann Hepatol. 2013 Mar-Apr;12(2):336–9.
2 Di Biscegli AM, Befeler AS. Hepatic Tumors and Cysts. In: Feldman M, Friedman L, Brandt LJ, editors. Gastrointestinal and Liver Disease. 10th ed. Elsevier;2016. p. 1603–27.
3 Martin P. Approach to the Patient with Liver Disease. In: Goldman L, Schafer A, editors. Goldman-Cecil Medicine. 25th ed. Elsevier;2015. p. 976–83.
4 Simon T, Bakker IS, Penninga L, Nellensteijn DR. Haemorrhagic rupture of hepatic simple cysts. BMJ Case Rep. 2015 Feb;2015:bcr2014208676. [ Links ]
5 Wang SH, Liu CH, Lin YP, Chang WK. Hypovolemic shock caused by a ruptured hemorrhagic hepatic cyst. J Emerg Med. 2015 Sep;49(3):e93–4.
6 Miliadis L, Giannakopoulos T, Boutsikos G, Terzis I, Kyriazanos ID. Spontaneous rupture of a large non-parasitic liver cyst: a case report. J Med Case Reports. 2010 Jan;4(1):2. [ Links ]
Statement of Ethics
The authors declare that they have followed the protocols of their work center on the publication of patient data. Patient consente was obtained.
Disclosure Statement
The authors have no conflicts of interest to declare.
Funding Sources
The authors did not receive any funding.
* Corresponding author.
Maria João Amaral
General Surgery Unit, Centro Hospitalar e Universitário de Coimbra
Praceta Prof. Mota Pinto
PT–3004-561 Coimbra (Portugal)
E-Mail mariajoaoamaral@hotmail.com
Received: May 2, 2019; Accepted: July 22, 2019
Author Contributions
All authors have contributed significantly to the care of this patient and to the drafting of the manuscript.

