










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkGE-Portuguese Journal of Gastroenterology
versão impressa ISSN 2341-4545
GE Port J Gastroenterol vol.26 no.1 Lisboa fev. 2019
https://doi.org/10.1159/000487155
CLINICAL CASE STUDY
Auxiliary Liver Transplantation as a Transient Treatment for Acute Liver Failure: Two Cases
Transplante Hepático Auxiliar como Tratamento Temporário para a Falência Hepática Aguda: Dois Casos
David N. Perdigotoa, Luís Toméa,b, Dulce Diogob, José Ferrãob, Ricardo Martinsb, Pedro Oliveirab, Guilherme Tralhãob,c, Emanuel Furtadob
aGastroenterology Department, Coimbra University and Hospital Centre, Coimbra, Portugal; bAdult and Paediatric Liver Transplantation Unit, Coimbra University and Hospital Centre, Coimbra, Portugal; cGeneral Surgery Department, Coimbra University and Hospital Centre, Coimbra, Portugal
* Corresponding author.
ABSTRACT
Introduction: Acute liver failure is an uncommon condition associated with a high mortality. Most patients do not survive without liver transplantation. In the last decades, auxiliary liver transplantation has emerged as a therapeutic option. Clinical Case: The authors present two cases of acute liver failure that required liver transplantation. Given the patients’ young age and the preserved macroscopic liver pattern evaluated in surgery, auxiliary liver transplantation was executed using different surgical approaches. Afterwards, following confirmed full native liver regeneration, the patients were submitted to auxiliary liver hepatectomy, which was accomplished without complications. Conclusion: Auxiliary liver transplantation can be regarded as an effective temporary treatment for acute liver failure in selected cases, allowing an immunosuppression-free life.
Keywords: Acute liver failure, Liver transplantation, Auxiliary liver transplantation, Immunosuppression
RESUMO
Introdução: A falência hepática aguda é uma entidade clínica pouco comum, mas associada a elevada mortalidade. A maioria dos doentes não sobreviverá sem transplante hepático. Nas últimas décadas, o transplante hepático auxiliar tem sido utilizado como uma opção terapêutica valorizável. Caso clínico: Apresentam-se dois casos de falência hepática aguda tratados com transplante hepático. Tendo em conta a idade jovem dos doentes e a noção de preservação macroscópica do fígado, recorreu- se à opção de transplante hepático auxiliar utilizando técnicas diferentes. Posteriormente, após confirmação de regeneração hepática completa, procedeu-se à hepatectomia do fígado auxiliar. Conclusão: O transplante hepático auxiliar constitui uma terapêutica transitória eficaz em alguns casos de falência hepática aguda, permitindo um futuro isento de imunossupressão.
Palavras-Chave: Falência hepática aguda, Transplante hepático,·Transplante hepático auxiliar, Imunossupressão
Introduction
Acute liver failure (ALF) is an uncommon condition associated with a high mortality rate, reaching 80–85% in the pre-transplantation era [1]. While liver transplantation is often the only curative treatment, it is only performed in 18% of cases [2]. Auxiliary liver transplantation (ALT) has emerged as a valuable alternative to orthotopic liver transplantation in the ALF setting [3, 4]. The graft allows liver function support during the period of native organ failure, giving the necessary time frame to the injured liver to regenerate.
The process and specific potential for full native liver regeneration (NLR) are not entirely understood, but it is known that young age and non-drug aetiology may be predictive factors for native organ recovery [5]. Additionally, the time between transplantation and NLR is very variable and can take weeks to months depending on the aetiology [6].
Initially, ALT was performed using the heterotopic ALT technique. While this procedure has the advantage of avoiding a hepatectomy in the recipient, issues such as graft congestion, caused by compromised graft hepatic outflow, may cause complications [7]. In the last 2–3 decades, partial ALT has gained recognition [3]. However, there is no consensus regarding appropriate graft placement. Recently, a new technique using advanced renoportal anastomosis, designated reno-portal ALT (REPALT), was described [8].
Case 1
An 18-year-old man presented to the emergency department complaining of abdominal discomfort, fatigue, and dark urine present during the past week. Acute hepatitis manifested itself through the laboratory results: alanine transaminase at 3,271 U/L (normal [N] < 34); aspartate transaminase at 2,627 U/L (N < 31); and alkaline phosphatase at 288 U/L (N 40–150). There was associated hepatic insufficiency with bilirubin at 12.1 mg/dL (N 0.3–1.2) and prothrombinaemia of 55% (N 70–120). The patient had no known past diseases. A detailed medical history revealed no past or current medication, no drugs or alcohol intake, and no consumption of other potential hepatotoxic components. A wide range of investigations including hepatitis virus A, B, C, and E, herpes simplex virus (HSV), Epstein-Barr virus, and cytomegalovirus, as well as autoimmune and Wilson disease tests did not allow the identification of a specific aetiology. Lastly, a liver biopsy showed acute hepatitis with multifocal necrosis and absence of other features.
Ten days after admission, the patient developed type A encephalopathy progressing to ALF. While the Clichy-Villejuif criteria were not matched (factor V of 46%), the King’s College criteria were fulfilled: a prothrombin time of 53.5 s (INR 5.13), bilirubin at 29.8 mg/dL, and the presence of jaundice for more than 7 days previous to encephalopathy development. Therefore, the patient required liver transplantation, which was done 3 days later.
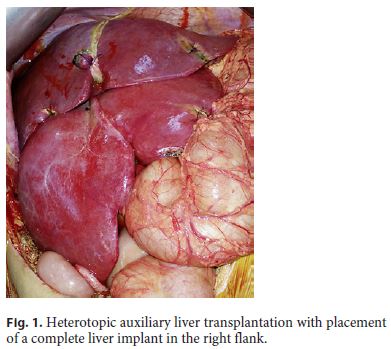
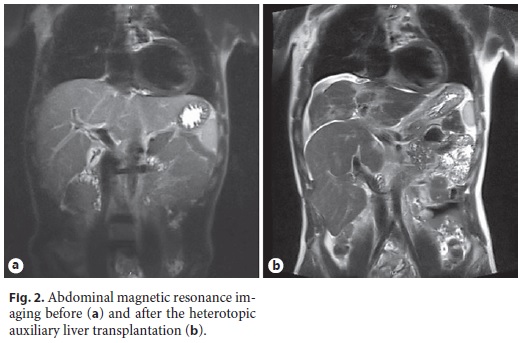
During transplantation, the native liver showed a preserved aspect macroscopically. Considering the patient’s young age and this surgical finding, an ALT was executed with inclusion of a complete liver implant in the right flank (Fig. 1, 2). Due to the graft’s apparently good quality, the entire liver was used for a heterotopic transplant. The graft’s hepatic artery was anastomosed to the aorta, the portal vein was anastomosed to the inferior vena cava requiring a special band on the cava to modulate the venous blood flow, and a hepaticojejunostomy was done for the biliary anastomosis.
Induction immunosuppression consisted of steroids and basiliximab. Subsequently, the patient received tacrolimus in combination with prednisolone (8 months) and mycophenolate mofetil (MM) for 5 months. Afterwards, treatment was limited to tacrolimus.
The hepatic encephalopathy rapidly ceased in the following days, and the patient’s global status gradually improved. Four days after transplantation, biopsies were performed in both livers. The native liver biopsy showed the presence of intranuclear inclusions that aroused suspicion of HSV infection, while the auxiliary liver only showed slight macrovesicular steatosis, but no other relevant findings. The patient was subsequently discharged in an improved condition.
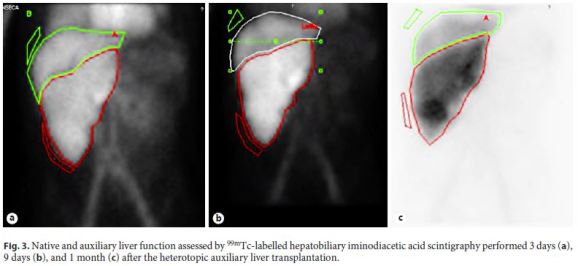
Sequential technetium-99m-labelled hepatobiliary iminodiacetic acid (99mTc-HIDA) scintigraphy was performed 3 days, 9 days, and 1 month after transplantation to evaluate both graft and native liver function. Both organs showed adequate function, elucidated by a homogeneous distribution in the first minutes of each scan, but there was a progressive decline in the native liver’s role after a favourable early NLR. The evolution of the functional proportion of native versus graft liver (35 vs. 65%, 25 vs. 75%, and 17 vs. 83%) demonstrates the increasing preponderance of the graft’s role in global function (Fig. 3). Additionally, the 1-month biopsy of the native liver still displayed a mild portal hepatitis, with the presence of hepatocytes with intranuclear inclusions. Despite these pathological findings, there was a noticeable improvement in the native liver.
Six months later, a histologic study of the liver identified no pathologic findings in the auxiliary liver, whereas the native organ still had mild alterations, namely, slight multifocal hepatitis and mild fibrosis (F = 1). A CT scan done 6 months after the surgery confirmed NLR through liver volume measurement.
Because of the ongoing minor hepatitis, the decision to remove the graft was delayed. Due to pathologic improvement, 1 year after transplantation it was decided to withdraw the immunosuppression. At this time, tacrolimus was slowly and progressively reduced. Ten months after removing the immunosuppression, biopsies showed a normal native liver, and the graft evidenced signs of an expected acute cellular rejection (Banff score of 9 [3 + 3 + 3]). Twenty-eight months after transplantation, the patient was scheduled for an elective auxiliary liver hepatectomy, which occurred with no associated issues. The patient had no later complications, and 6 months after the hepatectomy he is currently doing well.
Case 2
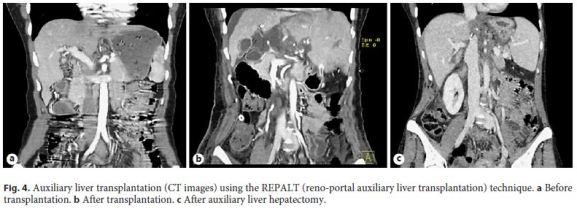
A 30-year-old, otherwise healthy woman was admitted due to malaise, abdominal discomfort, and nausea. The laboratory tests showed acute hepatitis with alanine transaminase at 4,307 U/L and aspartate transaminase at 1,906 U/L. The complementary investigation was notable for the presence of antimitochondrial antibodies (1/320 titre), with the anti-pyruvate dehydrogenase complex (PDC-E2) subtype positive but antinuclear antibodies negative. All the other tests revealed no relevant findings. One day after admission, the patient developed encephalopathy. Later, her biochemical tests deteriorated, matching the Clichy-Villejuif criteria: stage 3 encephalopathy and factor V of 28% (age ≥30 years). The King’s College criteria were also fulfilled, because the patient’s prothrombin time was 50.3 s (INR 4.76), bilirubin was at 25.7 mg/dL, and the cause of the liver failure was hepatitis of indeterminate aetiology. Afterwards, an urgent hepatic transplantation was done. During surgery, the liver showed a standard macroscopic pattern. An extemporaneous liver biopsy revealed severe centrilobular necrosis, with a preserved portal architecture and no other features. In this case, a more advanced and challenging technique, REPALT, was attempted, using a left liver implant after a segment I resection. The auxiliary liver was placed on the left flank according to the REPALT technique: the portal vein was anastomosed to the left renal vein, the left-medial hepatic vein branch to the inferior vena cava, and the hepatic artery directly to the aorta. The common biliary duct was anastomosed to the lesser curvature of the gastric body. Immunosuppression included basiliximab and steroids for induction, prednisolone (first 2 months), MM, and tacrolimus.
The patient experienced rapid clinical improvement after the transplantation. 99mTc-HIDA scintigraphy done 5 days after transplantation demonstrated preserved function in both livers (homogeneous distribution), with a slightly inferior function in the native organ. The patient was discharged 14 days after the successful transplantation. The native and auxiliary organs were subsequently studied in sequential biopsies performed 1, 4, and 6 months after the procedure. The native liver first showed unspecific hepatitis and a complete absence of pathologic findings at the 4-month control. Additionally, a CT scan corroborated the NLR by confirming an adequate liver volume. Therefore, MM was stopped and tacrolimus was progressively decreased. A planned successful auxiliary liver hepatectomy took place 7 months after transplantation (Fig. 4).
One month after the hepatectomy, the patient presented to the emergency department with jaundice and fatigue. A complementary investigation showed acute hepatitis and coagulopathy: prothrombinaemia of 40% and factor V of 35%. During admission, the patient was submitted to a transjugular liver biopsy that revealed the presence of severe interface hepatitis and bridging necrosis. Following these findings, she was treated with endovenous corticotherapy that allowed a fast clinical and laboratory improvement. One week later, the patient was discharged with oral corticotherapy. Her clinical and laboratory status improved substantially after the introduction of treatment, and 5 months later, she is still in excellent condition.
Discussion
ALF is an uncommon but severe and usually lifethreatening condition. A high percentage of patients will not survive without liver transplantation. Nevertheless, if the vital liver functions are preserved during a given period, NLR can occur in a particular number of patients. The growing rate of ALT adoption worldwide shows that this approach can be a good alternative treatment for ALF [3].
Herein, we report two cases of successful ALT applying different surgical procedures. Generally, immunosuppression can be gradually weaned off after confirmation of NLR, resulting in progressive atrophy of the implant [3, 9]. However, in these two cases, regardless of the hypothetic atrophy of the auxiliary liver, the decision to remove the graft was appropriate. In the first case, due to vascular competition, the graft assumed a predominant functional role that could have led to a certain degree of native liver atrophy. In addition, the patient required complementary surgery due to the non-standard abdominal closure with a prosthesis in the ALT. In the second case, hepatectomy was regarded as the correct procedure because of the specific vascular anastomosis created, namely, a left kidney venous drainage through the auxiliary liver. Additionally, because the REPALT procedure potentially allows using the graft for future transplantation [10], auxiliary liver hepatectomy is considered convenient. Besides, the lifelong presence of an atrophic allogenic organ can lead to potential future complications that have not been entirely studied.
Notably, in these two cases, the aetiology of the ALF became clearer after ALT. In the first case, the presence of intranuclear inclusions in two liver biopsies after transplantation allowed the diagnosis of probable HSV infection. In the second case, the patient presented with an autoimmune hepatitis (AIH) flare 1 month after the hepatectomy. At that time, the pathologic liver study revealed typical AIH features that were not present before. In the first biopsy during transplantation, the patient had only had centrilobular necrosis. These findings are consistent with the known idea that centrilobular necrosis can be the only pathologic feature in up to 2–3% of patients presenting with AIH flares [11–13]. Moreover, the patient had positive antimitochondrial antibodies, which, while being more specific for primary biliary cholangitis, might be associated with AIH [14]. In these ALF cases, liver support systems were not used, since they were unavailable.
In conclusion, ALT is a complex and challenging surgical technique that has the significant advantage of providing life-saving treatment to patients with ALF with the perspective of an immunosuppression-free life. The REPALT approach has the benefit of potentially making the graft available for future procedures.
References
1 Bernuau J, Rueff B, Benhamou JP: Fulminant and subfulminant liver failure: definitions and causes. Semin Liver Dis 1986;6:97–106. [ Links ]
2 Bernal W, Hyyrylainen A, Gera A, Audimoolam VK, McPhail MJ, Auzinger G, et al: Lessons from look-back in acute liver failure? A single centre experience of 3,300 patients. J Hepatol 2013;59:74–80. [ Links ]
3 Rela M, Kaliamoorthy I, Reddy MS: Current status of auxiliary partial orthotopic liver transplantation for acute liver failure. Liver Transpl 2016;22:1265–1274. [ Links ]
4 Belghiti J, Sommacale D, Dondéro F, Zinzindohoué F, Souvanet A, Durand F: Auxiliary liver transplantation for acute liver failure. HPB (Oxford) 2004;6:83–87. [ Links ]
5 Chenard-Neu MP, Boudjema K, Bernuau J, Degott C, Belghiti J, Cherqui D, et al: Auxiliary liver transplantation: regeneration of the native liver and outcome in 30 patients with fulminant hepatic failure – a multicenter European study. Hepatology 1996;23:1119–1127. [ Links ]
6 Quaglia A, Portmann BC, Knisely AS, Srinivasan P, Muiesan P, Wendon J, et al: Auxiliary transplantation for acute liver failure: histopathological study of native liver regeneration. Liver Transpl 2008;14:1437–1448. [ Links ]
7 van Hoek B, de Boer J, Boudjema K, Williams R, Corsmit O, Terpstra OT: Auxiliary versus orthotopic liver transplantation for acute liver failure. EURALT Study Group. European Auxiliary Liver Transplant Registry. J Hepatol 1999;30:699–705. [ Links ]
8 Ringers J, Baranski AG, Dubbeld J, Sarton E, Veenendaal RA, Schaapherder AF, et al: A novel technique for auxiliary partial liver transplantation with reno-portal anastomosis and avoidance of the hepatoduodenal ligament. Am J Transplant 2006;6:2802–2808. [ Links ]
9 Dokmak S, Aussilhou B, Durand F, Paradis V, Belghiti J: Complete spontaneous liver graft disappearance after auxiliary liver transplantation. Hepatology 2014;60:1104–1106. [ Links ]
10 Ringers J, Dubbeld J, Baranski AG, Coenraad M, Sarton E, Schaapherder AF, et al: Reuse of auxiliary liver grafts in second recipients with chronic liver disease. Am J Transplant 2007;7:2615–2618. [ Links ]
11 Hofer H, Oesterreicher C, Wrba F, Ferenci P, Penner E: Centrilobular necrosis in autoimmune hepatitis: a histological feature associated with acute clinical presentation. J Clin Pathol 2006;59:246–249. [ Links ]
12 Miyake Y, Iwasaki Y, Terada R, Onishi T, Okamoto R, Takaguchi K, et al: Clinical features of Japanese type 1 autoimmune hepatitis patients with zone III necrosis. Hepatol Res 2007;37:801–805. [ Links ]
13 Tiniakos DG, Brain JG, Bury YA: Role of histopathology in autoimmune hepatitis. Dig Dis 2015;33(suppl 2):53–64. [ Links ]
14 Tomizawa M, Shinozaki F, Fugo K, Motoyoshi Y, Sugiyama T, Yamamoto S, et al: Antimitochondrial M2 antibody-positive autoimmune hepatitis. Exp Ther Med 2015;10:1419–1422. [ Links ]
Statement of Ethics
This study did neither require the patients’ informed consent nor approval from the appropriate ethics committee. The patients’ anonymity was maintained.
Disclosure Statement
The authors have no conflicts of interest to declare.
* Corresponding author.
Dr. David N. Perdigoto
Gastroenterology Department, Coimbra University and Hospital Centre
Praceta Prof. Mota Pinto
PT–3000-075 Coimbra (Portugal)
E-Mail davidperdigoto@gmail.com
Received: December 15, 2017; Accepted after revision: January 25, 2018

