











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
1.Introduction
Globally, diabetes is a prevalent chronic disease that can result in debilitating health consequences. The condition is a leading cause of significant health problems such as kidney failure, heart attacks, stroke and blindness, and was ranked the ninth leading cause of death in 2019 by the World Health Organization [WHO] (2021). Further, people living with diabetes are more likely to have mental health problems, such as depression, than individuals without diabetes (Centers for Disease Control and Prevention, 2021). Apart from the undeniable physical and mental health challenges associated with diabetes, there is the associated financial implication, described as a “substantial economic burden” to clients, families, and health systems across countries (International Diabetes Federation [IDF], 2021, p. 57).
The IDF (2021) indicates in the year 2021, about 537 million adults worldwide were living with diabetes [ages 20-79 years], with expectation the number will increase to 643 million people by 2030 and 783 million people by 2045. The number of those living with the condition does not include those who are at risk of developing it-541 million adults (IDF, 2021). Notably, Type 2 diabetes is the most prevalent form (approximately 90% of all incidents), which is most diagnosed in older adults (IDF, 2020); increasing age is a risk factor for diabetes (PHAC, 2020). In 2020, 18% of Canadians 65 years and older had diabetes; this was also the age group with the highest incidence (Statistics Canada, 2021a). In the same year, specifically in the province of Ontario [the most populated Canadian province with over 14 million people as based on the same timeframe (Statistics Canada, 2021b)], 19% of adults aged 65 years and older had diabetes, and similarly this was the age group with the highest incidence (Statistics Canada, 2021a).
In examining the health of populations, one must consider the social determinants of health (SDH) (e.g., housing, geography, income, food insecurity, etc.); their impact can be more significant than those associated with, as example, diet and physical activity (Raphael et al., 2020, p. 14). In the context of diabetes and as based on Canadian data, SDH such as lack of employment, lower attainment of formal education, and lower income are associated with an increased disease risk (Public Health Agency of Canada [PHAC], 2018). Collectively, for many reasons, diabetes care for the older adult has unique considerations compared to those in other age groups, including simultaneously managing other chronic conditions with those associated treatments and medications (Diabetes Canada Clinical Practice Guidelines Expert Committee [DCCPGEC], 2018). Additionally, and perhaps as a result of those considerations, older adults with diabetes often fail to achieve or maintain diabetes self-management (DSM) competencies, increasing their risk of complications (Agarwal et al., 2018; Costa et al., 2017). It remains those barriers to DSM in seniors is still not well studied by researchers (Saunders, 2019).
Diabetes self-management education (DSME)-an essential part of diabetes care with the aim of reducing the risk of complications and morbidity-is particularly important for older adults (DCCPGEC, 2018). DSME is about “…facilitating the knowledge, skill, and ability necessary for diabetes self-care” (Powers et al., 2016, p. 70). In a systematic review and meta-analysis of DSME programs for older adults, Sherifali et al. (2015) found “tailored interventions or psychological support” (p. 1412) were most effective, with indication further research is needed. More recently, in Markle-Reid et al.’s (2018) randomized control trial, they also saw effectiveness with an older adult intervention program that was “client-driven” and “customized” for improved self-management and quality of life (p. 263). Yet existing (Ontario) Canadian evidence indicates older patients, as well as those with a lower social economic status and medical co-morbidity are less likely to attend DSME programs; further evidence is needed to understand these results (Cauch-Dudek et al., 2013).
Given the lack of/limitations in the existing evidence, our study purpose was to deepen the understanding of the experience of DSM and DSME for seniors with diabetes, with a related aim of exploring how the SDH affect DSME for seniors with diabetes living rurally. The study contribution of better understanding seniors’ DSM, experiences of associated education, and the implication of SDH, is foundational for determining future improvement strategies specific to their context and preferences. Our research questions were: 1) How do seniors (aged 65 years or older), who have diabetes and live rurally, describe their experiences of diabetes self-management (DSM) and diabetes self-management education DSME)? and 2) What affect do the social determinants of health (SDH) have on DSME for seniors with diabetes living rurally?
2.Social Determinants of Health Framework
As recommended based on evidence, we positioned this work within a SDH framework (Clark & Utz, 2014), specifically the SDH framework identified by Loppie-Reading and Wien (2013). They classify the SDH into distal (e.g., historic, political, social, and economic contexts), intermediate (e.g., community infrastructure, resources, systems, and capacities), and proximal (e.g., health behaviours, physical and social environment) categories (Loppie-Reading & Wien, 2013). It was central to our objectives, and pivotal in structuring analysis.
3.Description of the Study
In this qualitative study we used a combination of participatory (Etowa et al., 2007; Freire, 2013; Kidd et al., 2018), art-based (photovoice) (Wang & Burris, 1997), and hermeneutic phenomenology research (van Manen, 2014) methodologies to understand how the SDH affect DSME for older adults living with diabetes in rural Ontario, Canada. We believed it was important, in working with this specific community to address their needs, that a participatory approach be taken; photovoice, in complement to the participatory approach, is a way to ensure participants are empowered to focus on topics of their choosing and gives opportunity to unpack ideas that might otherwise be hard to describe during interview discussions. The hermeneutic phenomenology approach enabled our interpretations and was preferred given team expertise. Ethics approval was obtained from our university research ethics board (study#: 6024698).
3.1 Setting, Participants, & Recruitment
To align with our participatory approach, first we developed an Advisory Committee (AC) to involve community members, health-care providers, and decision-makers. The AC assisted in developing and implementing the best research processes for this study. Our community partner is a small, rural health service provider located in [placeholder] Canada; this location is the setting of our study. Health-care providers and AC members identified potential participants and provided them with study information. For individuals who expressed interest, our research team contacted them to provide detailed study information and obtain verbal informed consent. We recruited 14 participants (11 males, 3 females) of 15 who expressed interest, and their mean/median age is 74 years [age range 65-82 years]. Consenting participants were mailed iPads® to use as cameras, with step-by-step instructions and a follow-up email message to address questions.
3.2Data Collection
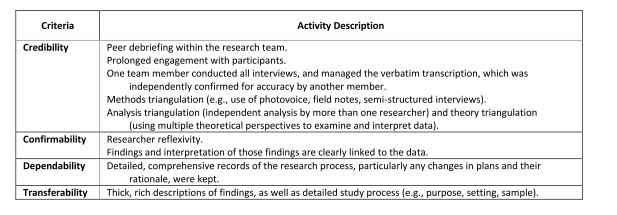
Data collection included photovoice and semi-structured one-to-one telephone interviews; the use of the telephone was a recommendation of the AC given the internet instability in this rural community, and the COVID-19 pandemic restrictions prohibiting in-person interviews. Participants were asked to take 15-20 photographs of images reflecting or representative in some way of their experiences living with diabetes, and then chose five photographs to discuss during their interview. Each participant had one telephone interview ranging from 31 minutes to 1 hour 20 minutes (average = 57 minutes), which was audio-recorded and transcribed verbatim using Otter.ai©. Participant pseudonyms are used in this article, and Table 1 is examples of our strategies to establish trustworthiness.
3.3Data Analysis
The SDH framework by Loppie-Reading and Wein (2013) underpinned the thematic analysis of data. Our analysis followed a hermeneutic phenomenological approach (van Manen, 2016), wherein interview transcripts were first read as a whole, and then each transcript was read in search of phrases particularly revealing of the experience of older adults with diabetes. This was followed by the development of thematic moments, and continued reflection and re-writing of essential themes (van Manen, 2016); this analysis was primarily conducted by two authors (MR, PC-P) and the AC was not involved, though received the findings.
4.Results
Based on the analysis, four themes were identified: 1) Health practices-The experience of living with diabetes; 2) Food and diabetes management; 3) Income-I can find myself, pretty regularly, on a basis of ‘what do I not pay for?’; and 4) Rurality-It’s harder to get medical attention.
4.1Health Practices-The Experience of Living with Diabetes
Participants’ stories and photographs showed their life with diabetes and how they managed it in their own way. During the interviews, there was little laughter, and descriptions of events brought back the reality of living with a long-lasting condition. Overall, most participants described how life had changed for the worse after diabetes, while some said nothing changed after their diagnosis. Participants reflected how daily self-care practices are necessary to regulate their diabetes; Maggie noted: “I don’t think it’s changed my way of life very much. I’m certainly more careful about what I eat.” The process of managing diabetes happened over the years by learning how to control portions and select healthy food to avoid complications; Oscar described:
Over the years I’ve learned more [about] the effects of carbohydrates, alcohol, these types of things. I’ll still enjoy my spaghetti, but I’m not going to have a second bowl. I never was a big person on sweets, but I cut back on that, and I’ve been successful in controlling it fairly good.
Through time, they learned to manage their disease to the best of their ability. After Jonathan was diagnosed, he minimized the seriousness of his condition. However, through time he learned to accept his diagnosis; he recalled: “There was suggestions made, and I’m not sure that I took them all. I just kind of thought now she’s [health provider] crazy. She’s not right. But she was, and I’ve learned to adapt…Absolute denial.” Denial and adaptation were normal reactions when participants learned about their diabetes diagnosis and lifestyle changes; Harold stated: “I guess looking back over the last 40 years, I didn't treat it as the potential threat.” The diagnosis was not a total shock for others given they have relatives and friends living with diabetes. They knew all too well what the disease could do, as Mike revealed: “When I was diagnosed with diabetes it didn’t come as a total shock. I’m on the heavier side, and I knew that that’s always a possibility, although I don’t think there’s a lot of diabetes in the family.” Mike appreciated how he was made to feel diabetes is not the end of the world and does not define him. The goal of managing their diabetes is to avoid complications or the use of insulin as John described: “I’m really glad I don’t have to manage insulin, I just oh, just so glad [laughing]. I look at friends who’ve done it, you know, all their lives.”
Management of medications is another aspect participants described. Self-administration of medications is seen as a significant piece of their daily experiences with diabetes and self-management practices. Taking their medications is a routine process that helps them control their disease and avoid complications. However, other participants were taken back to their reaction to the diagnosis and to the first prescription for diabetes; Oscar explained:
It was surprising to be diagnosed. And I said I don’t want medication [to] control it, but it didn’t really get under control till I accepted it and started taking the medication and doing the exercise and watching what I eat and how much I eat, etc. I don’t like taking medication…. I’ve never been big on medication; you’re putting something into your body. That to me is not natural.
Participants who manage other chronic conditions could feel overwhelmed; Jane stated: “If you get some other condition and you're on-I just find having to take a lot of medications is one of the difficult things for me too.” When diet, treatment or blood tests are not followed, participants felt guilty; Wilson revealed: “Feeling guilty that I don’t do it [blood testing] as much as I should. Probably [I] can’t do everything.”
4.2Food and Diabetes Management
While for some participants access to healthy food did not seem to be a concern, others struggled to afford a well-balanced diet that would help to manage diabetes. For example, possessing a good income is linked to accessing healthy food, as stated by Mike:
I don't have to go in the grocery store and say, oh! I would love some of those clementines - but [the] price, there's [that is] too much, and I can't afford them this week. So, I'm very blessed in that way that I can purchase healthy food.
On the other hand, for Harold, buying food meant paying attention to the cost of it; he described: “I don’t really eat a lot of red meat. But the price [high cost] of beef [laughing], I eat a lot more chicken and pork chops and stuff like that now, than I used to.” Participants agreed food was an essential component of their diabetes management. They described how they thought about it and managed to have the food they need by changing their habits and growing their own vegetables. Harold stated: “I’ve changed my eating habits. I grow a lot of my own vegetables now, and I freeze them and can them. I eat a lot more vegetables than I used to 25 years ago.” Growing their vegetables is a way to save some money, keep them active and eat healthy food.
Although most participants noted eating healthy was vital, many said diabetes changed how they approached food, such as learning to read labels. Jane shared her learning over time, saying: “When I shop, I’m always looking at labels. Like I love cereal in the morning, like crunchy cereal, and honest to God, it is so hard to find a cereal that isn’t packed with sugar.” Participants suggested education about reading food labels and food purchase decision-making would be a helpful strategy to promote diabetes prevention. For other participants, eating healthy meant learning how to control behaviors. Harold said: “I basically, I don’t buy foods specifically made for diabetics. Over the course of a day, I have one spoonful of sugar in my morning coffee, and as the only sugar, any sugar, that I eat.”
4.3Income-I Can Find Myself, Pretty Regularly, on a Basis of ‘What Do I Not Pay For?’
For some participants, having the financial means to manage their diabetes is problematic; income and employment competes with diabetes care-related expenses, and paying house expenses competes with glucose monitoring equipment. John commented: “I have a very small chunk of Canada Pension, and I have old age security, and then I have the money I make [job]. And so, I can find myself, pretty regularly, on a basis of ‘what do I not pay for?’” Likewise, Kevin described: “When you're taking your sugar, two or three times a day, it gets to be expensive after a little bit, and that's hard.” Monitoring one’s diabetes on a daily basis and maintaining healthy habits is challenging when living on a low income, as sometimes the only option is to travel long distances for affordable food; John stated: “There are no real options that are affordable, and I don’t have a lot of money. So, there are no real affordable options other than driving yourself.” For other participants like Mike, being financially secure is a blessing for someone living with diabetes; he related: “I'm financially secure enough that when I go [to] the grocery store, I don't have to look at something and say, ‘Oh, dear, I can't afford that, it would be good for me’.”
Employment is also perceived as important by participants; with recognition some types of jobs can impact their health if they have diabetes. Jane, a retired teacher, commented how her last five years of teaching were stressful, and as such, she was not surprised by her diagnosis; she recounted:
So, I wasn’t surprised. I was diagnosed with diabetes, high blood pressure and high cholesterol all at the same time. And once I retired, I started having a healthier lifestyle and a lot less stress in my life. And I didn’t have to take any medications for almost 10 years.
For others, working and managing diabetes is not an easy task. Wilson claimed: “So maybe it’s much harder, it’s much harder to have a job and be diabetic.” For other individuals, employment is a fulfilling part of their lives, and includes the benefit of seeing other people and socializing.
On the other hand, for some participants having diabetes did not prevent them from working. Joel described his experience of having diabetes while being a bus driver: “If you have it, you don’t have to stop what you were doing…There’s no reason to lay at home and feel bad.” John echoed a similar sentiment, saying: “I think the social aspect [of work is good] because it doesn't come easily for me to be social.”
4.4Rurality-It’s Harder to Get Medical Attention
Rurality is a critical aspect in the stories and photographs of participants. Individuals mentioned it was challenging to access services in rural areas. This could be difficult in the best of circumstances, but as well it had specific implication for participants in managing their diabetes; driving long distances to the medical center, as well as larger grocery shops and pharmacies was the norm. John said: “I live in a situation where I have to drive 18 to 20 kilometers just to buy groceries.” Similarly, Harold mentioned living rurally makes selection and access to healthy food difficult; he said:
They’re not huge shops. It’s not like you go into [name of large supermarket chain] you’ve got a huge selection. But I basically, I don’t buy foods specifically made for diabetics. Getting access to the medical center when you live out in…a thinly inhabited area…Yeah, I’d say it’s harder to get medical attention.
Joel also revealed how difficult it was to access DSME for seniors living rurally, saying: “It’s 45 minutes to an hour to the nearest place where there’s any education.” Mike felt the same, describing: “I think here, it's our isolation and our small [town]. It's certainly better if we can have programs that are here as opposed to driving to [city].” However, participants recognized the efforts of the health-care practitioners in their rural medical center to address their health needs, including education, and were perhaps resigned to their circumstance; “I think because we're a small community, and we're more isolated, it means that they're more limited in terms of what of they can offer compared to a larger center, but I think they do their best [Mike].”
For participants, transportation is a key necessity for living rurally and attending diabetes education. For those who do not have a car, moving around and getting to appointments can be difficult; Wilson reflected: “For most people here, it’s transportation, getting people to appointments. I mean, I have a car, so I don’t have a problem with that, but I’m sure there’s people who find it difficult.” Individuals explained how they had adapted to living rurally, accommodating their needs to the environment; Rose described: “We pick up our groceries, we try and get in only once a week. We try and keep a good stock of stuff. We’re food hoarders.”
5.Discussion
Our aim was about exploring the experiences of DSM and DSME for seniors with diabetes. In our study, an important illumination from participants was diabetes did not define them, rather it was something to attend to while navigating their daily living. This is also described by other Canadian researchers conducting qualitative research (21 participants; age range 19-71 years) (Ndjaboue et al., 2020), and it is significant when considering how care and education is delivered. As providers, there may be a tendency to ‘place’ the disease as central, when individuals clearly wish to be treated as a whole person and have their care shaped with the person in mind-this has application to educational programs.
A related goal was also to understand how the SDH affect DSM and DSME for seniors with diabetes in rural Ontario. Our findings substantiate how fundamental the SDH are in supporting and sustaining DSM practices and education in rural settings. Health practices, and food and diabetes management, financial hardships, and the effects of rurality were some of the key SDH reported by our participants. This aligns with other researchers who demonstrated how the SDH are central to the development and progression of diabetes in vulnerable populations (Chard et al., 2021; Clark & Utz, 2014; Hill-Briggs et al., 2021).
For some of our participants, the decision to engage in healthy self-management habits was based on their determination to prevent health complications, as well as avoid the use of insulin and its perceived intrusiveness in their lives, especially on their independence. Adu et al. (2019) and Tong et al. (2015) similarly described how individuals with diabetes engaged in healthy behaviors and activities to maintain their quality of life and avoid complications. Further, other researchers have also found participants were concerned about their diabetes and its complications (Carolan-Olah et al., 2014; Park & Wenzel, 2013). However, some participants in our study were not concerned about diabetes, seeming to accept it as a condition they anticipated, such as when diabetes is in their family or there are no upsetting symptoms. Regarding managing the disease, our results are consistent with Speight and Singh (2013), who found individuals with diabetes interpret a lack of identifiable symptoms as a signal their diabetes is controlled. Learning to identify and interpret symptoms leads to understanding health/illness behavior and promotes better self-management practices (Kirk et al., 2015), and leads them to take action after understanding their illness and role in self-management (Costa et al., 2021).
The second theme was food and diabetes management. Our results align with Beverly et al. (2018), who found sociocultural beliefs toward food need to be integrated into DSME. Our participants described growing their vegetables as a foundational element to control diabetes, being active, and eating healthy under budget. Those aspects also need to be considered when developing DSME programs. Further, the barriers resulting from the intersection of rurality, access to food, and DSM were especially evident for participants living on a low income. Some participants, living rurally, could not afford foods appropriate for their DSM. For them, being able to always buy healthy food in the community was an unrealistic expectation. They traveled long distances to buy food less expensive. Similarly, Chan et al. (2015) established how food insecurity negatively affects DSM in individuals living in Ontario. Chan and colleagues found factors such as living on a low income, lack of knowledge about healthy food choices, multimorbidity, social isolation, and inadequate cooking facilities affect food acquisition, selection, and preparation for individuals with diabetes.
Finances was also foremost for participants, even if they were retired [which does not equate to a good income], and income was identified as a critical element in DSM; in Saunders’ (2019) integrative review regarding older adults with diabetes, they also identified cost of care as a self-management challenge. Individuals living on a low income have a higher incidence of poorer glycemic control, more diabetes complications, and higher mortality (Chan et al., 2015; Hsu et al., 2012; Seligman et al., 2012; Tanaka et al., 2012; Vest et al., 2013). Poverty is associated with inadequate DSM (Hsu et al., 2012; Vest et al., 2013). Participants felt a comfortable socioeconomic status allowed them to increase their self-efficacy in diabetes management and their access to resources. However, for those participants living on a low income, it was a day-to-day struggle of deciding between basic needs (paying rent versus diabetes monitoring or accessing healthy food).
The final theme, rurality, also emerged as an important SDH affecting DSM. The possibility of being active was mentioned by our participants as a positive in regard to living rurally. Conversely, Arcury et al. (2006) demonstrated how the lack of appropriate places to walk made it more difficult for rural adults to engage in outdoor activities. Similar to other researchers, we found participants commented on the negative aspects of rurality, including a lack of access to healthy food, services, and health care (Homenko et al., 2010; Lutfiyya et al., 2011). Our findings add to the increasing evidence about the positive and negative impact of geographical location on DSM for seniors, and how rurality as a SDH must be considered in the development of DSME programs.
Overall, our results suggest participants’ DSM ability is profoundly affected by interrelated SDH. Participants expressed many struggles with SDH, which impeded their DSM. Through our findings, we have reaffirmed DSM is not a simple task that needs a prescribed set of clinical guidelines, but a complex interaction of individual needs, the SDH, and access to the right resources. The findings have provider practice and education implications, illuminating the importance of individualized care, and sensitivity to guidelines that may not be achievable for all given their circumstance. The findings also provide focus for future research regarding seniors and DSM/DSME, including intervention studies for facilitating reading of food labels, and healthy food accessibility; similar studies with more diverse populations are also needed.
6.Study Limitations
This study was conducted in a rural community, and most participants are Caucasian white males of English descent. As such, different perspectives about DSME may be obtained from suburban and urban populations, with a more diverse representation of sex, gender, and ethnicity. Additionally, while the use of the telephone for the interviews was extremely helpful in this context and it did allow us to attend to tone of voice when participants emphasized elements, it did prevent the use of visual aids that may have assisted, and it precluded the observation of participant non-verbal behavior (body language).
7.Conclusion
We demonstrated how the SDH affect DSME and self-management for older adults with diabetes living rurally. Participants were continuously rearranging their diabetes needs to accommodate other life priorities. Additionally, while rural living has its benefits, it is described as a barrier to DSM; accessing diabetes education, food, medications, and gas is at a distance-a particular inconvenience during wintertime. Critically, the barriers resulting from the intersection of rurality, access to food, and DSM were especially evident for participants living on a low income. These key local findings will guide future design, planning and implementation of DSME programs for seniors in this rural setting.

