










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkRevista Portuguesa de Enfermagem de Reabilitação
Print version ISSN 2184-965XOn-line version ISSN 2184-3023
RPER vol.6 no.1 Silvalde June 2023 Epub June 30, 2023
https://doi.org/10.33194/rper.2023.316
Original article reporting clinical or basic research
Outline for the intervention of the Rehabilitation Nurse - organization of care for healthy and active aging
1
, Conceptualization, Data curation, Formal analysis, Research, Methodology, Project administration, Resources, Supervision, Validation, Visualization, Original draft wording, Writing - proofreading and editing, read, agreed with the published version of the manuscript http://orcid.org/0000-0002-3346-5707
http://orcid.org/0000-0002-3346-5707
2
, Project administration, Resources, Validation, Writing - proofreading and editing, read, agreed with the published version of the manuscripthttp://orcid.org/0000-0003-1527-9940
1
, Writing - proofreading and editing, read, agreed with the published version of the manuscripthttp://orcid.org/0000-0002-5632-5408
3
, Writing - proofreading and editing, read, agreed with the published version of the manuscripthttp://orcid.org/0000-0001-7251-5829
1Centro Hospitalar Universitário de São João, Porto, Portugal
2Universidade do Porto, Instituto de Ciências Biomédicas Abel Salazar, Porto, Portugal
3Escola Superior de Enfermagem do Porto; Porto, Portugal
Introduction:
Active aging is a European concern that requires health and social professionals to rethink their practices.
Methodology:
We seek to understand the care model for the elderly in a Group of Health Centers (ACES) in the North of Portugal to deduce the role of rehabilitation nurses in the community. We carried out a qualitative, phenomenological study. The intentional non-probabilistic sample consisted of eight Doctors, eight Nurses and eight Social Workers who develop their activity for people over 65 years old in an ACES. Data collection was carried out through a semi-structured interview, constituting the results of the body of analysis that sustains this research.
Results:
83% of participants had no training in gerontology. There were care evaluation focuses, in which all professionals estimated the same data, but there were data necessary for monitoring the elderly that were not evaluated by any professional. The sharing of information for assistance, when it occurred, fell into situations of illness or changes in the social context.
Discussion:
It was possible to verify that in all themes there is information that converges in the three groups of professionals, mainly in the data collected in the initial evaluation. As advocated by some authors, sharing information and dividing teamwork is important for a more specialized intervention aimed mainly at this age group.
Conclusion:
In this way, it was possible to perceive that the work of the three groups of professionals interviewed often intersects and that there is a need for data sharing between the multidisciplinary team, with the specialized work of the Rehabilitation Nurse being valued and important.
DESCRIPTORS: Elderly; Assistance; Models; Rehabilitation; Nursing; Health Promotion
Introdução:
O envelhecimento ativo é uma preocupação europeia que exige aos profissionais de saúde e sociais repensar as suas práticas.
Metodologia:
Procuramos compreender o modelo de assistência dos idosos num Agrupamento de Centros de Saúde (ACES) do Norte de Portugal para deduzir o papel dos enfermeiros de reabilitação na comunidade. Realizamos um estudo qualitativo, do tipo fenomenológico. A amostra não probabilística intencional foi constituída por oito Médicos, oito Enfermeiros e oito Assistentes Sociais que desenvolvem a sua atividade para pessoas com mais de 65 anos num ACES. A recolha de dados foi elaborada através de uma entrevista semi-estruturada, constituindo os resultados do corpo da análise que sustenta esta pesquisa.
Resultados:
83% dos participantes não possuíam formação em gerontologia. Havia focos de avaliação da assistência, em que todos os profissionais estimavam os mesmos dados, mas havia dados necessários ao acompanhamento dos idosos que não eram avaliados por nenhum profissional. A partilha da informação para a assistência, quando ocorria, recaía nas situações de doença ou de alterações do contexto social.
Discussão:
Foi possível verificar que em todas as temáticas há informação que converge nos três grupos de profissionais, principalmente nos dados colhidos na avaliação inicial. Tal como defendem alguns autores a partilha de informação e divisão do trabalho de equipa é importante para uma intervenção mais especializada e dirigida principalmente nesta faixa etária.
Conclusão:
Desta forma foi possível perceber que o trabalho dos três grupos de profissionais entrevistados muitas vezes se cruza e que há necessidade de partilha de dados entre a equipa multidisciplinar, sendo valorizado e importante o trabalho especializado do Enfermeiro de Reabilitação.
DESCRITORES: Idoso; Assistência; Modelos; Reabilitação; Enfermagem; Promoção da Saúde
Introducción:
El envejecimiento activo es una preocupación europea que requiere que los profesionales sociales y de la salud reconsideren sus prácticas.
Metodología:
Buscamos comprender el modelo de atención a los ancianos en un Grupo de Centros de Salud (ACES) en el Norte de Portugal para deducir el papel de las enfermeras de rehabilitación en la comunidad. Realizamos un estudio cualitativo, fenomenológico. La muestra no probabilística intencional estuvo constituida por ocho Médicos, ocho Enfermeros y ocho Trabajadores Sociales que desarrollan su actividad para personas mayores de 65 años en un ACES. La recolección de datos se realizó a través de una entrevista semiestructurada, constituyendo los resultados del cuerpo de análisis que sustenta esta investigación.
Resultados:
El 83% de los participantes no tenían formación en gerontología. Existían focos de evaluación del cuidado, en los que todos los profesionales estimaban los mismos datos, pero había datos necesarios para el seguimiento de los ancianos que no eran evaluados por ningún profesional. El intercambio de información para la asistencia, cuando ocurrió, cayó en situaciones de enfermedad o cambios en el contexto social.
Discusión:
Fue posible verificar que en todos los temas hay informaciones que convergen en los tres grupos de profesionales, principalmente en los datos recogidos en la evaluación inicial. Como defienden algunos autores, compartir información y dividir el trabajo en equipo es importante para una intervención más especializada dirigida principalmente a este grupo de edad.
Conclusión:
De esa forma, fue posible percibir que el trabajo de los tres grupos de profesionales entrevistados muchas veces se entrecruza y que existe la necesidad de compartir datos entre el equipo multidisciplinario, siendo valorado e importante el trabajo especializado de la Enfermera de Rehabilitación.
DESCRIPTORES: Ancianos; Asistencia; Modelos; Rehabilitación; Enfermería; Promoción de la Salud
INTRODUCTION
The increasing aging of the population in our society has helped in the development of projects related to the assistance of the elderly. The promotion of healthy aging leads to the need for changes in health systems, in which disease-based curative models are outdated and are modified in an integrated service centered on the needs of the elderly over 65 years of age 1 , which motivated us for the present study.
Despite the numerous adverse effects of a sedentary lifestyle and the benefits, albeit modest, of increased physical activity, it is known today that physical inactivity continues to be a constant among various age groups of the population, especially among the elderly. 2, being considered the greatest community risk factor for health in Portugal. Therefore, the growing trend of population aging, which has worsened for some decades, requires a broad response from public health 1) .
Taking into account the existence of various care models, it can be emphasized that health and social care in this age group should be as preventive as possible and promote overall well-being, with multidisciplinary assessment and intervention being relevant in primary health care in the community with the aim of a multidisciplinary approach centered on the elderly as a whole.
In a multidisciplinary perspective of care in the community for the elderly, it is important to denote the importance of rehabilitation nursing based on specific knowledge and skills that allow an effective adoption of a holistic perspective of care, considering the person, the family and the environment as integral and inseparable parts of their decision-making processes, because their skills are based on prevention and rehabilitation, particularly mobility 14) .
Upon becoming aware of the guidelines on assistance policies for the elderly, the evidence of good practices in the care of this age group, the opinion of the elderly regarding their health and the assistance in the study in which we are included, in which 2461 people over 65 years old participated and presented, among other data, that 38.5% demonstrated a negative lifestyle, 87% recognized that they had a family doctor and 68% recognized the family nurse, 25% had already had one fall, 4% two falls and 3% three or more falls and even though 21% consider their health status to be bad, 36% report having increased their consumption of medication in the last 12 months, with diabetes and musculoskeletal diseases being the most reported pathologies (3 ) .
More than 1 in 5 people are over 60 years old, in a larger number of countries understanding Healthy Aging in all policies and at all levels of government is fundamental 1) . For this reason, it is believed that this study could encourage reflection on health promotion and improve quality of life, so that intervention falls within this scope using interdisciplinary teamwork.
In this context, the starting point of the study focused on the results of a research study carried out in a municipality in the North of Portugal and the respective Grouping of Health Centers (ACES) called “Models in use in assisting the elderly”. In order to clarify the path of investigation and understand the problem under study, the following research question was formulated: Do health and social professionals organize their assistance based on a model that promotes the health of people over 65 years of age, resorting to the availability of added value from the environment and from the elderly themselves?. The answer to the question presented may provide subsidies to expand knowledge about interdisciplinarity, contributing to improve the quality of health care for the elderly. Therefore, the present study aims to understand, based on the speeches of the health team, the development of care for people over 65 years of age, to remain healthy, active, independent and autonomous, and to analyze the areas where rehabilitation nurses have skills to contribute to the improvement of assistance in this area.
METHODOLOGY
Study design
The study was carried out in a Group of Health Centers in Vila Nova de Famalicão. As it is a public health service, whose mission is to guarantee the provision of close health care to the population of a given geographic area, it is composed of several units that integrate multidisciplinary teams. It is important to note that the authors are aware of the context, of the studies previously carried out with the population of over 65 years old, in which 2,461 elderly people participated, and of the results that emerged from it, with regard to the social and health perception. In this study, we intend to be guided by the following objectives: to understand the care model for the elderly in the municipality and to analyze the professionals' perception of the conditions of people over 65 years of age. Taking into account the objectives and characteristics of the study, we embarked on a qualitative field study based on phenomenology.
Participants
The choice of research subjects was carried out intentionally. In order to understand the care model in use to care for people over 65 years of age in this geographic area, the inclusion criteria used were the participation of doctors and nurses with a higher incidence of people over 65 years of age on their care lists and the participation of social workers who they assisted the elderly for more than a year, mostly in USF model A and a UCSP.
Data collection instrument
Taking into account the objectives and nature of this study, we chose the semi-structured interview. The interview of this study consists of three parts, the first being the consent, where the researcher is introduced, framing the study in the project, the explanation of the study, such as the name, purpose and objectives of this study, duration, conditions of participation, and questions of confidentiality and anonymity (signing of informed consent), the second referring to questions of context (gender, age, training in gerontology and profession) and the third consisting of thirteen guiding questions for the interview.
Data analysis
After transcribing the interviews, a first reading of all the interviews was carried out and then they were coded, organizing reference tables. The speeches produced by the interviewees were analyzed using content analysis according to the principles outlined by Bardin 4) . After transcribing the interviews, a first reading of all the interviews was carried out and then they were coded, organizing reference tables. The results obtained were presented in the form of categories, subcategories and recording units.
Ethical considerations
Access to the population was made from the ACES of the region under study, after a formal request to the ACES (since the project already had authorization for all inherent studies), to the ARS and to the Ethics Committee (of this study in particular -Opinion No. 19/2015). The request referred to all the information about the project and this study in particular. Before starting the interview, itself, the study and the conditions of participation were explained, and informed consent was signed by all participants. In the transcription of the interviews, they were coded with the letter’s A/E/M (“Social workers” / “Nurses” / “Doctors”), followed by Arabic numerals and randomly, depending on the subjects who caused them, ensuring so the coding. It was also mentioned to all interviewees that participation was voluntary, and that the information was confidential, and after transcription and codification, the recordings were eliminated.
RESULTS
Characterization of the participants
The research was developed with 24 participants, 23 women and 1 man, especially the female gender. The age of the three professional groups ranged from 30 years to a maximum of 60 years, with a predominance of the age group of 31 to 40 years in the groups of social workers and nurses and in the group of doctors, the age group of 51 to 60 years prevailed. 20 of the professionals did not have specific training in gerontology.
THE FLASH OF ELDERLY CARE IN AN ACES
The development process of this work begins with the proposal to carry out an investigation included in the Project Living well with the more-age - from the family context to institutional support. Thus, after analyzing the literature and recent scientific evidence, the need and the importance of reflecting on this theme and developing a preliminary study, which will serve as a basis for the development of an Assistance Model for the Elderly, arose.
From the result of the analysis of the interviews with the professionals, we found a flash, that is, a reductive view of the assistance to the elderly of the professionals in their practice, since we offer what was only perceived through the eyes of each professional from the different units of the parishes of a municipality of the North of the country with more population over 65 years old.
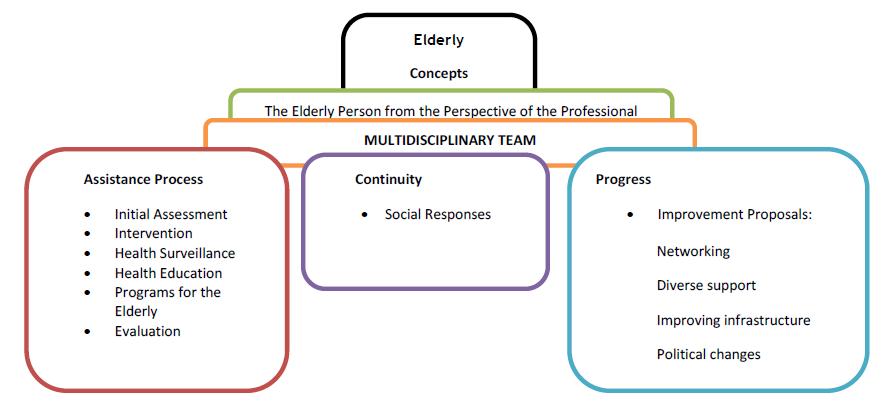
Through content analysis of the interviews, we sought to discover meanings and group the information obtained, which made it possible to identify the themes. Figure I reflect the mirror of a developed model that will be useful for interdisciplinary work and organization of care with a view to promoting active aging, being presented by themes that emerged from the emerging categories. From the thematic areas presented in the following Figure I, the categories and subcategories and respective registration units will be referred, and the information obtained will be discussed. Therefore, in the next figures, the categories identified in relation to the elderly person from the perspective of the professional who will guide the work of the multidisciplinary team and the categories related to the care process, such as initial assessment, intervention and health education, will be perceptible. also value the need for programmed surveillance and programs for the elderly defined according to the needs of the target population.
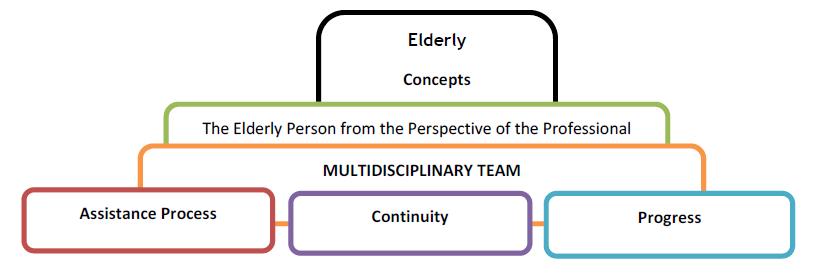
The flash made it possible to see an organized care process based on the concepts of professionals about the elderly client, which led us to find the idea of a work in which the multidisciplinary team is supported by three pillars: the care process, continuity and the progress. In this sense, we will focus on the results of the assistance process.
As a way of evaluating the thinking of professionals about those over 65 years of age, they were asked what their thinking was when they looked at the elderly. After interviewing health and social professionals, different categories emerged as positive and negative aspects and according to the vision of each group of professionals represented in Table I. These categories show how professionals perceive the elderly, most of them with aspects positive aspects related to life experience and the will to remain active, however and due to advancing age with fragility in terms of health, interaction and relationships and, consequently, to remain active.
Table I The elderly from the perspective of professionals
| The elderly from the perspective of professionals | ||
|---|---|---|
| Professionals | positive aspects | negative aspects |
| Social Workers | Life experience active person Relational Perception - Positive person with lifetime Remodeling |
health condition negative behaviors Relational Perception - Negative |
| nurses | Life experience active person |
health condition negative behaviors |
| Doctors | Life experience active person Relational Perception - Positive Supports |
health condition Associated problems Relational Perception - Negative |
In this context and according to the summary presented in Table I, we can see that aging is neither a positive nor a negative experience... in fact, a process with expression in the person's temporality, adhering to their life history, so that we age as we live, neither better nor worse. We perceive a balance between acquisition, a positive aspect, and losses, often considered negative, although the loss does not always represent an end; often engenders a takeover.
We verified that there was sharing of information between the various professionals, however it was necessary to deepen the meanings given by each of the participants to the concept of teamwork and how this work emerged in practice, which led us to identify the categories: multidisciplinary team, emerging professional classes, such as Nurse, Doctor, Social Worker, Social Educator, Psychologist, Sociologist, Administrator and Nutritionist. The identified data that would be pertinent to be shared with a multidisciplinary team were Self-Care, Health Conditions, Social, Family, Risk Conditions and information and aids for the development of teamwork. The periodicity of contact between teams obtained divergent findings and the need for articulation with other entities, such as local associations, Board, Council, schools, Private Institutions of Social Solidarity (IPSS), among others, was notorious. Nurses identified the importance of communication with the team.
Seeking to understand whether health and social professionals make a differentiated initial assessment for this population, we pose the following question: How do they carry out the initial assessment of clients over 65 years of age? Do they apply any scale, questionnaire, form and/or interview with specificities for these ages?
Based on the analysis, it can be concluded that all classes of professionals, including Social Workers, Nurses and Doctors, carry out the initial assessment of the elderly based on specific assessment data and validated instruments/scales, with these two categories emerging, with Nurses valuing as well as information systems.
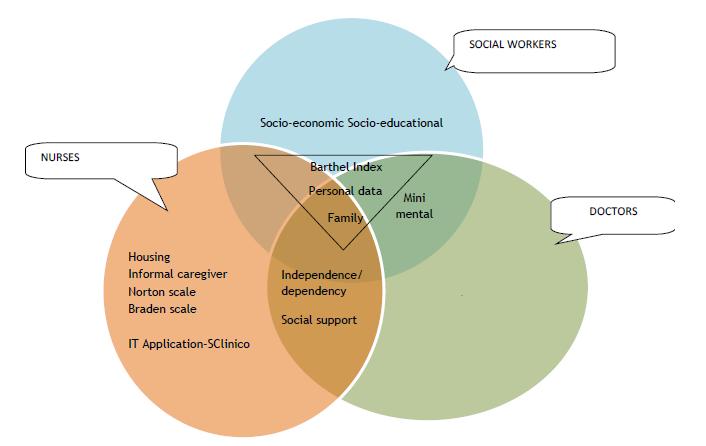
From the two categories described above, subcategories emerged as it is possible to verify in Figure II, there are data that are collected by the three groups of professionals, such as the Barthel Index, personal data and related to the family, making it possible to verify their importance , and the need to share collected data to avoid data duplication.
Barthel scale, which at the moment is through this scale that we monitor the user more or less closely. (E2). Barthel scale , to know if independent or not. (M2). [...] we have in an initial phase at the time of candidacy, the Barthel scale , which we adopt even for the level of dependence that is usually physical that this scale gives [...]. (A4).
Only Social Workers mentioned socioeconomic and socio-educational data. The Mini Mental was mentioned by Doctors and Social Workers.
[…] Yes, we normally spend the mini mental […]. (A5). […] Cognitive. It is the mini mental that we use the most [...]. (M3).
Both Doctors and Nurses reported data on independence/dependence and social support.
[…] If the patient is autonomous, if the patient does not have any deficit or any complaint at a motor or cognitive level [...] if he eventually has some kind of alteration, he is adapted […]. (M3). […] I see what the user's problems are, I raise the points and complete a normal initial assessment, regardless of whether they are over 65 years old […]. (E2).
Nurses cited data referring to housing, informal caregivers and the Norton and Braden scale , as well as the SClinico computer application.
[…] We here, at the service, work with SClínico in terms of IT. In terms of elderly health, the program itself already gives us. Opening the health program for the elderly from 65 onwards is mandatory for a patient over 65 years of age, he immediately enters into self-care, self-care, hygiene, clothing, transfer. We have to say if there is any kind of dependency when performing this type of self-care, but we work more in these areas [...]. (E6).
Since the elderly are the age group where there is a greater probability of physical and psychological decline, as well as problems with memory and other physical, mental, intellectual and social functions, the need for multidisciplinary intervention is imminent. Therefore, the professionals were asked about the approach and relevance of intervention in this age group (Figure III).
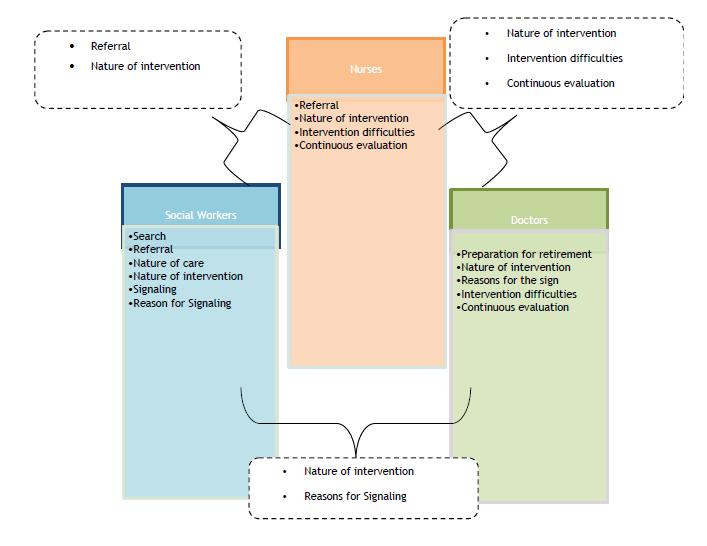
According to Figure III, where the categories related to the effectiveness of the intervention are highlighted, it is possible to verify that the three professionals focused on aspects related to their intervention, specifying some of their area of intervention.
[…] It is not a population that resorts to our care service [… ].( A1).
It was mentioned by a Social Worker that his intervention is not sought after by the elderly, since they do not resort to his services by their own will and need.
The social workers referred to the importance of the nature of care in this age group, such as referral to home, host family, home support, community center and day center, reporting and contact with the health center, filling out all documentation of identification and social report and the importance of socio-familial, socio-economic and health-illness assessment, the need to verify data and open a process.
The social workers mentioned that the signaling is carried out by neighbors, relatives or institutions, verifying that the Doctors and Social Workers valued the category reasons for the signaling, such as abandonment, violence, change in family health and lack of rear.
[…] abandonment, not only in the hospital but in the institutions themselves […]. (A7). […] abandoned at home, so we activated social services [ …] . (M8).
[…] an elderly woman was a nuisance […]. (A7). […] suspicion of mistreatment, therefore domestic violence […]. (A5).
[…] there are disagreements between neighbors […. ]. (A5) […] negligence on the part of these family members […]. (A5).
[…. ] for various problems or health[…]. (A7). […] I can't I'm pregnant […. ]. (A7).
[…] it is an elderly couple who have no children […]. (M8).
In relation to the nature of the intervention, data were mentioned regarding treatment, home visits, articulation between professionals, identification of phenomena, interventions at the family level, individual teaching, group teaching, economic support, change strategies behavior/ motivation; rehabilitation and preparation for reform.
Strategies for changing behavior/motivation were cited by Nurses and Social Workers.
[…. ] meet the expectations they create and when there is a need to make some behavioral adjustment it is done without them being aware that it is being done and they end up changing behaviors without realizing that they are being motivated to do so[…] . (A4). […] until we managed to adjust our diet and physical exercise at the same time, so go have some water, go have some coffee, it’s ok one a day, it’s ok, it doesn’t matter, but you shouldn’t take the car, go on foot instead of going to the cafe… by car […]. (E3).
These professionals also mentioned the importance of Rehabilitation in this age group.
[…] they come with the specific diagnosis and to carry out rehabilitation specifically for that pathology […]. (E1). […] some rehabilitation scales […]. (E1). […] he has the ability to dress himself […]. he has the ability to put food in his mouth [...]. (E1). […] maybe the caregiver even dresses him and he has the ability to get dressed, puts food on him and he has the ability to put food in his mouth […]. (E1). […] technical aids, at the moment it is the support product attribution service (SAPA) […]. (A3).
One category identified is preparation for retirement being referred by a physician.
[…] Retirement age is a complex age, because our users, I don't know if they have this training, but the educational and training level is very low and they are not used to any of that... from the moment that the user starts to have all the time for himself and stops deciding what to do with the time [ ...]. (M6).
The Nurses and Social Workers specified that referral is most often carried out for social responses and continued care in the community, and in situations of violence it is referred to a regional center and public prosecutor with the person's consent.
Only Nurses and Doctors mentioned intervention difficulties, due to the high number of patients, the need to comply with indicators, difficulties in collecting clinical information and due to economic factors. They also valued the continuous evaluation of their intervention to improve it, referring to the evolution of dependence and dementia.
Although there is no consensus, it is noticeable that surveillance (in a health center or at home) is more restricted and less spaced out in chronic patients, diagnosed with hypertension, diabetes or another chronic disease.
Another category referred to was health education, and work with the elderly should be centered on health education, on care based on knowledge of the process of senescence and senility and on the return of functional capacity to carry out their tasks. activities, with the aim of meeting their basic needs and achieving their independence and happiness. Thus, we obtain targeted themes presented in subcategories (Figure IV).
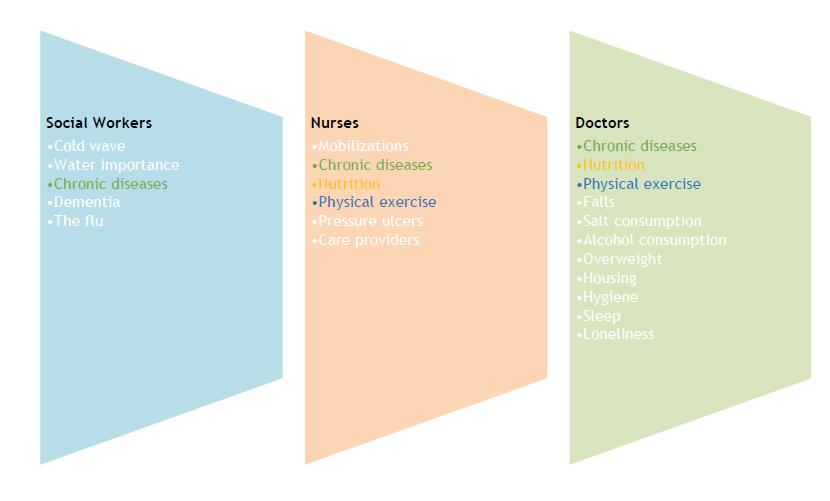
According to this Figure IV, it is possible to verify that the need for health education about chronic illness was mentioned by the three groups of professionals, while the issues of food and physical exercise were listed only by Nurses and Doctors.
[…] By encouraging the practice of physical activities, […] active exercise session […] active exercise in the elderly and the fact that they are elderly, they remain the most active [… . ]. (E1). […] exercise. (E2).
As well as health education actions, where the interaction of the elderly with other people is promoted and mental activities are stimulated through their active participation.
The promotion of health-related practices, such as primary disease prevention, the proper management of health problems as well as the promotion of safety behaviors, such as the prevention of falls […] walk when you can, walking care, what should avoid, avoid falls, remove those elements that are left over at home or that can precipitate a fall [...]. (M2), are important for promoting healthy and consequently active aging; it is also important to adopt a healthy lifestyle.
Adopting healthy lifestyles and actively participating in self-care are important at all stages of life. One of the myths of aging is that it's too late to adopt these styles later in life. On the contrary, involvement in appropriate physical activities, […] healthy eating, care for […] food […]. (E2), […] food advice […]. (M6), […] salt restrictions[ …]. (M3), [...] abstinence from smoking and alcohol, modifying alcoholic habits [...] (M3), and wisely using medication can prevent diseases and functional decline, increase the individual's longevity and quality of life
Having said that, questions were asked about programs for the elderly within the target population, emerging categories related to the promotion of well-being, safety and well-being. The Social Workers mentioned the senior pass, free senior sport, […] senior sport, swimming and free sport[…], (A4) and close monitoring of the elderly, […] a police officer [… ] develops that program of proximity to the elderly and that we go[…] when there are suspicions that the elderly person is at risk or on the verge of[…] and we go to see how the elderly are doing and if they need support, if there are collaterals available or if the collaterals are far away and that they don't care about the elderly [...]. (A7).
Nurses mentioned a project regarding vaccination counseling, […] PAI, which was a project we had […], all the elderly, all people over 65 years of age, we were advising and vaccinating with the vaccine from pneumonia ( pneumo 23) […]. (E2), close monitoring of the elderly, [...] we should have more support in this sense and not in the sense of … institutionalizing [...] If they had support, and also the proximity police [...]. (E3) and health screenings where they invite the entire population and even denoted partnerships with the council.
To summarize what was mentioned in the speeches, it is noticeable that this theme is quite reductive, and it is pertinent to understand that in this age group the programs are very relevant, since there is often a transition at various levels and the whole process is due to specific and specialized monitoring , with the autonomy and independence of elderly people often at stake, the promotion of enabling environments, taking into account the impact of these strategies on the main determinants of the active aging of each citizen.
With regard to the objectives of this study, more precisely to the care model available for the elderly in the municipality studied in the North of the country, the following Figure V.
The results studied in relation to the evaluation of the care process, continuity of care and progress will be presented in the future, as a way of improving and developing the presented model.
Finally, reflecting on the activities whose Rehabilitation Nurses (RE) could be an added value, it is important to point out that in the speeches of the participants, areas contextualized in the competences appear specifically: Maximizes functionality by developing the person's capabilities5) , where participants refer: […] By encouraging the practice of physical activities, […]active exercise session[…] active exercise in the elderly and the fact that they are elderly they remain the most active[… .]. (E1); […] exercise. (E2), areas that require knowledge that are held particularly by these specialized nurses. As well as enabling the person with a disability, activity limitation and/or participation restriction for the reinsertion and exercise of citizenship5) , being mentioned by the participants that in this age group they are […] sad individuals […]. (M5), who […] feel “I am not useful and where am I going to fit in”[ …]. (E3), with […] mobility difficulties […]. (M2) and […] dependents […]. (E2), so the Specialist Nurse in Rehabilitation Nursing will contribute so that those at […] home are autonomous […]. (A3). It takes care of people with special needs, throughout the life cycle, in all contexts of care practice5) , which is another ER competence, so that in this age group there are changes at various levels […] guidance [… ]. (M2) […] memory state […]. (M2) and […] issues of mistreatment […]. (A8) [...] abandonment, a patient who is under poor care [...]. (E4 ), with specialized care being an added value.
DISCUSSION
Regarding the health status category (table I) and according to the author, the first idea that comes to mind when we ask someone about what it means to be elderly is a tenuous reference to aspects such as illness, frailty, disability and, mainly, memory loss, prejudice against old age being noticeable even when someone says that the other is getting old due to the fact that they cannot remember, for example, where they left their car keys. From another angle, when the first strands of white hair start to appear on our heads, we will certainly always think that we are getting older 6) .
Other categories mentioned are people with life experience (table I), active people and people with a lifetime, and due to all the difficulties in facing social reality, many elderly people deny their own existence and age, so that they can be accepted again in younger groups. Such behavior boils down to not being able to face old age. Staying young and active is the desire of all those who are aging, but it is necessary to be aware of age, accepting it, transmitting your life experience and living fully. Based on what was mentioned in the previous chapters, it is clear that the negative behaviors of this age group are frequent, for many elderly people, the reality of exclusion has become more accentuated in old age. These conditions bring even worse repercussions, when one thinks that at the stage when they believed they had achieved dignity and respect, they became victims of an oppressive and excluding system 7) .
Regarding the multidisciplinary team composition category, it was possible to verify that the professionals mentioned the Doctor, Social Worker, Social Educator, Psychologist, Sociologist, Nutritionist and Administrator. Data that, from the professionals' perspective, should be shared within the multidisciplinary team were also valued, such as self-care, health conditions, social conditions, family conditions, development of teamwork and risk conditions. The complexity of current health care requires that “[...] teamwork is systematically referred to as a fundamental human factor for the quality of care provided in health institutions” (8:53 ) . Its purpose is to avoid fragmented thinking and promote integrated care. It can be described as a well-organized set of services and assistance processes aimed at the multidimensional needs of the elderly, which grants better results to the articulated performance of the multidisciplinary team than individual performances (9 ) . Therefore, it appears that the change to comprehensive care requires restructuring at the level of services, as well as reformulating the work carried out by health teams with a focus on interdisciplinary collaboration. It is also important to consider that teamwork and communication are closely linked to patient care safety 10) .
The initial assessment was a theme identified by the professionals, with specific data to be assessed valued, such as personal data, family, socioeconomic, socio-educational, social support, independence/dependence, housing and caregiver information, as well as the activity assessment scales and mental capacity.
National and international studies 11-12) show the importance of the effectiveness of a holistic and multidimensional assessment of the elderly, highlighting the clinical, physical, mental, functional, social, nutritional assessment, among others, with the use of several instruments. “All evidence suggests that it benefits both healthy individuals and those with significant impairments and multiple comorbidities” (12:7) . This assessment also reveals a paradigm shift, since it is currently not considered for healthy people and is still very much aimed at identifying medical, mental and functional problems of frail elderly people 11) . Other studies emphasize focusing on the assessment of the elderly with significant cognitive alterations, in addition to morbidity and functionality 11) . This multidimensional assessment carried out by a team consisting of a doctor, a nurse and a social worker, among others, Primary Health Care constitute privileged places for interdisciplinary assistance to the elderly and health promotion.
The assessment corresponds to the first stage of the Nursing Process, which is extremely important for identifying nursing care needs. The Barthel index is the most commonly used instrument to assess whether the elderly are able to perform certain activities independently, comprising ten basic activities of daily living: eating, using the toilet, personal hygiene, bathing, dressing and undressing, sphincter control, walking, transferring from chair to bed, going up and down stairs. Still focusing on the physical aspects, the nurses apply the Norton or Braden scale to assess the health of the elderly. These instruments are frequently used in the professional practice of these nurses, since pressure ulcers are a highly sensitive focus of attention in nursing care. However, it is admitted that this practice is not systematized in all health institutions 13) .
Another theme that was reported by the professionals was the intervention of the three professionals involved, having identified the categories demand, nature of the service, nature of the intervention, referral, reasons for signaling, intervention difficulties and continuous evaluation. In the nature of the intervention, the importance of rehabilitation was highlighted.
Rehabilitation, as an educational process, must be dynamic, continuous and progressive, and must have as its objectives the functional recovery of the person, his/her reintegration in the family and in the community. The same author states that rehabilitation aims to improve or replace function and limit the impact of disability. Rehabilitation Nursing is a creative process that begins in primary prevention care, in the first stage of the disease or accident (secondary prevention) and continues in the recovery phase, implying an adaptation of the whole being to a new life (tertiary prevention). ) 14) . According to the same author, rehabilitation nursing follows the following assumptions, aimed at the person being cared for: “defining objectives for maximum levels of functional interdependence and activities of daily living; promote self-care, prevent complications and subsequent disability; reinforce positive adaptive behaviors; ensure accessibility and continuity of services and care; advocate an optimal quality of life; improve the expected results; contribute to reforms in the character, structure and provision of care in health services” (14:3) .
Of the new social demands in the provision of health services, comprehensive health care for the elderly stands out, which should include biopsychosocial changes typical of aging, as a way to enhance functional capacity and quality of life. In this context, another category mentioned was health education, with health promotion being essential for active aging, with the aim of minimizing the risk of frailty and vulnerability, through participation, social control and integrated and expanded actions in the face of multidimensionality. of the elderly 15) .
Among the actions used for health promotion, educational interventions stand out, which may facilitate the process of adherence to treatment and rehabilitation, as well as promote positive attitudes. In this way, understanding is facilitated, improving formal education and enabling the construction of new spaces of knowledge, whether internal or external to the care scope through educational and dialogic relationships. These, in turn, transform the practice of professionals who start to see the person and their relationship with the world and not just with aging 16) .
Programs to promote well-being, safety and health were also identified that could make a great contribution if a rehabilitation nurse were included in the team. With the growing growth of an aging population, there has been a greater concern with the implementation of physical activity programs, with the aim of alerting society to the importance of social involvement and the need to create healthy lifestyle habits, as a regular practice of physical activity 17) . However, it is known that most elderly people do not have or have very little knowledge about the benefits of physical activity in the aging process, and how they can be regularly active 18) .
After analyzing the care model for the elderly, it is possible to refer to the relevance and need for rehabilitation nursing in primary health care, specifically in the family health units (USF), where this study was carried out, due to all the requirements reported by the professionals. and with a view to active ageing, based on health promotion and disease prevention.
CONCLUSION
The care model for people over 65 years of age existing in the ACES of a municipality in the north of the country covers factors related to the attempt at strategies predisposing to a care practice that has active aging as its main focus.
The care model we arrived at is based on the elderly and the professionals' perspective of the entire care process, valuing the need for multidisciplinary assessment and intervention, with information sharing, in addition to health education and programs for the elderly. .
Professionals take into account the conditions and environment of the elderly, with emphasis on promoting behavior aimed at active aging, however, they did not demonstrate articulation between professional groups.
Finally, the need for rehabilitation nursing in the multidisciplinary team was also evident, due to all the needs and demands of the elderly and taking into account the reflection on the competences of the rehabilitation nurse in the gerontological area.
Some flaws in the sharing of information emerged from the speeches, since it appears that both in the initial assessment and in the intervention process there is repetition of data that could be more specifically collected and worked on by professionals if there was greater and better sharing between the multidisciplinary team .
The multidisciplinary assessment in this age group focuses mainly on factors related to motor, cognitive and social support capacities, but it is clear that the assessment of dependence should be focused in more detail on that person and that an assessment specialized mainly in improving well-being in a phase with the aim of sharing a specific plan for each user with the team, it was an added value in a care model for people over 65 years of age.
In our perspective, this study presents a limitation with regard to the sample, since for a qualitative study the sample is large and covers different classes of professionals, making it sometimes difficult to analyze some of the results obtained. The confrontation with the complexity of information, its organization and layout, was undoubtedly the most delicate phase, in a way generating anxiety, including due to the continuous state of alert that the phase required, given the need to promote the recommended rigor, however gradually overcome. We would like to suggest a quantitative study to validate the model in use.
REFERENCES
1 Organização Mundial da Saúde. Relatório Mundial de Envelhecimento e Saúde [Internet]. Genebra; 2015 [cited 2023 Fev 10]. Available from: http:// apps.who.int/iris/bitstream/10665/186468/6/ WHO_FWC_ALC_15.01_por.pdf?ua=1 [ Links ]
2 Escalante Y. Actividad física, ejercicio físico y condición física en el ámbito de la Salud Pública. Rev Esp Salud Pública [Internet]. 2011 [cited 2023 Fev 10];85(4):325-8. Available from: https://scielo.isciii.es/scielo.php?script=sci_arttext&pid=S1135-57272011000400001 [ Links ]
3 Martins MM, Martinho J, Nogueira N, Araújo F, Marques P, Santos R. Viver bem com mais idade do contexto familiar ao apoio institucional. Relatório. Escola Superior de Enfermagem do Porto. Porto; 2018. [ Links ]
4 Bardin L. Análise de conteúdo. 5a ed. Lisboa: Edições 70; 2009. [ Links ]
5 Ordem dos Enfermeiros. Regulamento 125/2011. Regulamento das competências específicas do enfermeiro de reabilitação. 2011. [ Links ]
6 Castro SFF de, Barros Júnior FO. Atenção à Saúde do Idoso: o pensar e o fazer Políticas Públicas. Revista Kairós Gerontologia, 19 (Número Especial 22, “Envelhecimento e Velhice”), 2016. ISSNe 2176-901X. São Paulo (SP), Brasil: FACHS/NEPE/PEPGG/PUC-SP, p. 270-294. [ Links ]
7 Scortegana PA, Oliveira RCS. Idoso: um novo ator social. Seminário de pesquisa em educação da região do Sul; 2012. [ Links ]
8 Santos MC, Grilo AM, Andrade G, Guimarães T, Gomes A. Comunicação em saúde e a segurança do doente: problemas e desafios. Rev Portuguesa Saude Pub [Internet]. 2010 [cited 2023 Fev 10];(10):47-57. Avaliable from: http://hdl.handle.net/10400.21/3120 . [ Links ]
9 Boeckxstaens P, De Graaf P. Primary care and care for older persons: position paper of the European Forum for Primary Care. Qual Prim Care [Internet]. 2011 [cited 2023 Fev 10];19(6):369-89. Available form: https://pubmed.ncbi.nlm.nih. gov/22340900/ . [ Links ]
10 Portugal. Ministério da Saúde. Direção Geral da Saúde. Plano Nacional de Saúde: Revisão e Extensão a 2020 [Internet]. Lisboa (PT); 2015 maio [cited 2023 Fev 19]. Available from: https://drive.google.com/drive/folders/ 1eozNFyshkj7xOnuBZfL0aKMtVTvwNKGT?usp =sharing . [ Links ]
11 Ellis G, Gardner M, Tsiachristas A, Langhorne P, Burke O, Harwood RH, et al. Comprehensive geriatric assessment for older adults admitted to hospital. Cochrane Database Syst Rev. 2017;9(9):CD006211. DOI: 10.1002/14651858. CD006211.pub3 . [ Links ]
12 López MVG, Bastante MM, Torres LM, Cantero ADP. Cuidados básicos para la edad avanzada. Spain: Grupoparadigma. Serie Cuidados Básicos, Geriatria, Gerontologia y enfermería geriátrica. Editorial DAE; 2015. [ Links ]
13 Portugal. Serviço Nacional de Saúde. Direção Geral da Saúde. Plano Nacional para a Segurança dos Doentes 2015-2020 [Interrnet]. Lisboa (PT); 2015 [cited 2023 Fev 19]. Avaiable from: https:// www.dgs.pt/qualidade-e-seguranca/segurancados-doentes/plano-nacional-para-a-segurancados-doentes-2015-2020.aspx . [ Links ]
14 Hoeman SP. Enfermagem de Reabilitação Prevenção, intervenção e resultados esperados. Lusodidacta, 2011. ISBN: 9789898075314. [ Links ]
15 Brasil. Ministério da Saúde. Caderno de Educação Popular em Saúde [Internet]. Brasília (DF); Ministério da Saúde; 2014 [cited 2023 Fev 19]. Avaiable from: bvsms.saude.gov.br/bvs/publicacoes/2_caderno_educacao_popular_saude.pdf. [ Links ]
16 Patrocinio WP, Pereira BP. Efeitos da educação em saúde sobre atitudes de idosos e sua contribuição para a educação gerontológica. Trab Educ Saúde. 2013;11(2):375-94. [ Links ]
17 Costa M, Rocha L, Oliveira S. Educação em saúde: estratégia de promoção da qualidade de vida na terceira idade. Revista Lusófona de Educação. 2012; 22: 123-140. [ Links ]
18 Silva SR, Marques FD, Seiro DI, Parreiral S, Tavares J, Atalaia L, Raposo D. Sentimento de comunidade e bem-estar em contexto institucional: perceção das pessoas idosas. Exedra Revista científica ESEC; 2016. [ Links ]
Declaration of informed consent: Written informed consent to publish this work was obtained from the participants.
Received: March 09, 2023; Accepted: May 28, 2023; Published: June 19, 2023
 Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
