










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkRevista Portuguesa de Enfermagem de Reabilitação
Print version ISSN 2184-965XOn-line version ISSN 2184-3023
RPER vol.6 no.1 Silvalde June 2023 Epub June 30, 2023
https://doi.org/10.33194/rper.2023.318
Original article reporting clinical or basic research
Quality of care structure in Physical Medicine and Rehabilitation Units: nurses' perception
1
, Conceptualization, Data curation, Formal analysis, Research, Methodology, Project management, Resources, Validation, View, Writing of the original draft, Writing - proofreading and editing, read, agreed with the published version of the manuscript http://orcid.org/0000-0002-5632-5408
http://orcid.org/0000-0002-5632-5408
1
, Methodology, Project management, Resources, Supervision, Validation, Writing of the original draft, Writing - proofreading and editing, read, agreed with the published version of the manuscripthttp://orcid.org/0000-0001-9982-9537
1
, Writing - proofreading and editing, read, agreed with the published version of the manuscripthttp://orcid.org/0000-0002-6631-776X
3
, Writing - proofreading and editing, read, agreed with the published version of the manuscripthttp://orcid.org/0000-0003-1527-9940
1
, Writing - proofreading and editing, read, agreed with the published version of the manuscripthttp://orcid.org/0000-0002-3346-5707
2
, Writing - proofreading and editing, read, agreed with the published version of the manuscripthttp://orcid.org/0000-0001-7251-5829
1Hospital de São João, Porto, Portugal
2Escola Superior de Enfermagem do Porto, Porto, Portugal
3Universidade do Porto, Instituto de Ciências Biomédicas Abel Salazar, Porto, Portugal
Introduction:
With the development of society, the concept of quality has become essential within health care organizations. However, little is known about the impact of the structural component of the Donabedian model on the quality of care provided by the Specialist Nurses in Rehabilitation Nursing. The purpose of this study is to identify and analysis the factors related to the quality of rehabilitation nursing care in Physical Medicine and Rehabilitation Units in the light of the Donabedian model in the structure dimension.
Methodology:
Case study of a qualitative nature. We used a non-probability convenience sample, with all participants being RNs from the same service. Data were collected through a semi-structured interview, composed of eight open-ended questions and a set of eight questions for socio-demographic and professional characterization. In data analysis, we used the guidelines for content analysis proposed by Bardin (2009) using the Atlas.ti software.
Results and Discussion:
From the analysis of the speeches of the 16 participants, in light of the Donabedian model in the thematic area Structure, the following categories emerged: people management and leadership in the service and physical environment and conditions for the functioning of nursing practices. The Donabedian model supported the discussion in conjunction with other references. We found discrepancies in the participants' discourses, specifically regarding the work methodologies and workload distribution related to rehabilitation nursing care. The work method emerges as a hampering contribution for some nurses, while, for others, it is an added value for the accountability of the autonomous practices developed.
Conclusion:
We can conclude that the nurses identify facilitating and complicating factors within the structure of the service, which interfere with the quality of care.
DESCRIPTORS: Physical Medicine and Rehabilitation; Nursing Care; Rehabilitation Nursing; Quality of Health Care; Structure
Introdução:
Com o desenvolvimento da sociedade, o conceito de qualidade tornou-se fundamental no âmbito das organizações de saúde. Contudo pouco ainda se sabe sobre o impacto da componente estrutura do modelo de Donabedian na qualidade dos cuidados prestados pelos Enfermeiros Especialistas em Enfermagem de Reabilitação (EEER). O objetivo deste estudo consiste em identificar e analisar os fatores relacionados com a qualidade dos cuidados de enfermagem de reabilitação nas Unidades de Medicina Física e Reabilitação (MFR) à luz do modelo de Donabedian na dimensão estrutura.
Metodologia:
Estudo de caso de natureza qualitativa. Utilizamos uma amostra não probabilística de conveniência, sendo todos os participantes, EEER do mesmo serviço. Os dados foram recolhidos através de uma entrevista semiestruturada, constituída por oito perguntas abertas e um conjunto de oito perguntas para a caraterização sociodemográfica e profissional. Na análise dos dados utilizamos as orientações para a análise de conteúdo propostas por Bardin (2009) com recurso ao software Atlas.ti.
Resultados
e Discussão: Da análise dos discursos dos 16 participantes, à luz do modelo de Donabedian na área temática Estrutura emergiram as seguintes categorias: gestão de pessoas e liderança no serviço e ambiente físico e condições para funcionamento das práticas de enfermagem. O modelo de Donabedian suportou a discussão em conjugação com outros referenciais. Encontramos discrepâncias nos discursos dos participantes, especificamente em relação às metodologias de trabalho e de distribuição da carga de trabalho relativa aos cuidados de enfermagem de reabilitação. O método de trabalho surge como contributo dificultador para alguns enfermeiros, enquanto, para outros é uma mais-valia para a responsabilização das práticas autónomas desenvolvidas.
Conclusão:
Podemos concluir que os enfermeiros identificam fatores facilitadores e dificultadores no âmbito da estrutura do serviço, que interferem com a qualidade dos cuidados.
Descritores: Medicina Física e Reabilitação; Cuidados de Enfermagem; Enfermagem em Reabilitação; Qualidade da Assistência à Saúde; Estrutura
Introducción:
Con el desarrollo de la sociedad, el concepto de calidad se ha convertido en esencial dentro de las organizaciones sanitarias. Sin embargo, poco se sabe sobre el impacto del componente estructural del modelo de Donabedian en la calidad de los cuidados prestados por las Enfermeras Especialistas en Enfermería de Rehabilitación. El objetivo de este estudio es identificar y analizar los factores relacionados con la calidad de los cuidados de enfermería de rehabilitación en las Unidades de Medicina Física y Rehabilitación a la luz del modelo de Donabedian en la dimensión estructura.
Metodología:
Estudio de casos de carácter cualitativo. Se utilizó una muestra no probabilística de conveniencia, siendo todos los participantes EEER del mismo servicio. Los datos se recogieron a través de una entrevista semiestructurada, compuesta por ocho preguntas abiertas y un conjunto de ocho preguntas de caracterización sociodemográfica y profesional. En el análisis de los datos, se utilizaron las directrices para el análisis de contenido propuestas por Bardin (2009) utilizando el software Atlas.ti.
Resultados y Discusión:
Del análisis de los discursos de los 16 participantes, a la luz del modelo de Donabedian en el área temática Estructura, surgieron las siguientes categorías: gestión de personas y liderazgo en el servicio y entorno físico y condiciones para el funcionamiento de las prácticas de enfermería. El modelo de Donabedian apoyó la discusión junto con otras referencias. Encontramos discrepancias en los discursos de los participantes, específicamente en lo que se refiere a las metodologías de trabajo y a la distribución de la carga de trabajo relacionada con los cuidados de enfermería de rehabilitación. El método de trabajo surge como una contribución obstaculizadora para algunas enfermeras, mientras que, para otras, es un valor añadido para la responsabilización de las prácticas autónomas desarrolladas.
Conclusión:
Podemos concluir que los enfermeros identifican factores facilitadores y complicadores dentro de la estructura del servicio, que interfieren en la calidad de los cuidados.
Descriptores: Medicina Física y Rehabilitación; Cuidados de Enfermería; Enfermería de Rehabilitación; Calidad de la Atención Sanitaria; Estructura
INTRODUCTION
Looking at the quality of a service requires knowledge on the service, the care provided in that context, and the rules to be followed to guarantee quality.
The specialty of Physical Medicine and Rehabilitation (PMR) has a long history in Continental Europe and is recognized in almost all UEMS (Union Européene des Médicins Spécialistes) countries. Its structure varies in different countries, but its modernization and progress occurred after the Second World War with the return of soldiers, who suffered injuries resulting from their service, and with the need for employability of the population, leading to an increase in PMR units 1.
Currently, the National Health Service (NHS) faces multiple challenges due to demographic changes, changes in disease patterns, technological innovation and geographic mobility. Faced with these challenges, the Physical Medicine and Rehabilitation Hospital Referral Network (PMRHRN) was created under the responsibility of the Directorate-General for Health (DGH) within the scope of the PMR specialty 2.
The existence of PMR services in hospital services is essential, since in these health units differentiated care is provided essentially in the acute phase of the disease, which is potentially disabling in cases of stroke, spinal cord injury, traumatic brain injury (TBI), amputations, among others 2.
In recent years, the paradigm transition from a biomedical model to a biopsychosocial model imposes a different working method on the most common set of professionals in these PMR services. In these contexts, physiatrists, nurses, rehabilitation nurses, physiotherapists, speech therapists, occupational therapists, social workers, psychologists, nutritionists, among others, appear more frequently. In these services, teamwork must be effective and centered on the rehabilitation process of each person, which determines that decision-making must also be carried out by a team. The staff is defined as the group of professionals available in the service of different areas, but with the objective of interaction that enhances the achievement of results 3.
With the development of health and consumer demands, the concept of quality has become fundamental in health organizations. Within the scope of hospital institutions, the most used model is that of Avedis Donabedian (2003), and it is based on seven pillars: effectiveness, efficiency, effectiveness, accessibility, optimization, legitimacy and equity. This author developed a model consisting of three components: Structure (characterized by relatively stable aspects such as facilities, equipment, professionals and resources), Process (set of activities that professionals carry out to respond to the needs of patients, which includes diagnosis, therapy and preventive actions) and Outcome (which refers to levels of health, associated costs and patient satisfaction). With the aim of promoting and assessing quality, it is important to note that the components are not quality attributes, but types of information that can be obtained, and the combination of the three components allows for an improved understanding of quality in health 4.
Rehabilitation nurses are faced with four pillars: their short history, little scientific knowledge of the area, techniques similar to other professionals and little differentiation of their role in care, in some contexts. The RN’s field of action is also influenced by the different types of postgraduate training, continuous training, self-training and even by professional associations, of which the Portuguese Association of Rehabilitation Nurses (APER) is an example, as well as the regulatory body of the profession, the Order of Nurses (ON). That said, a problem emerges about the beliefs and values of nurses in their professional practice, which makes it necessary to study their perceptions and foundations for the context of services and organizations, in order to guarantee, more effectively, safety and quality in health.
From the RN’s perspective, we intend to analyze the structural aspects for the exercise of their activity, focusing on the aims of analyzing the perception of the RN in relation to the structure that supports care and analyzing the perception of specialist nurses in rehabilitation nursing on facilitating and hindering factors in providing care related to the structure in a PMR unit.
Given the importance of exploring practice guidelines based on quality standards, it is also important to understand how the RN value the structure for their clinical practice, since rehabilitation nursing is a specialized area of intervention that aims to maintain and promote well-being and quality of life, the recovery of functionality as much as possible, resorting to promoting self-care, preventing complications and maximizing capabilities. 5 Thus, we formulated the starting question “How do specialist nurses in rehabilitation nursing perceive the structure to support the nursing care provided in a Physical Medicine and Rehabilitation unit?”.
METHODOLOGY
Study Design
The qualitative nature of the study allows improving knowledge in nursing in the particularity of empirical, aesthetic, personal and moral knowledge 6, which appears in the participants' speeches as authors of the experience of being and caring in rehabilitation nursing and was designed through a case study. We consider the study to have case characteristics, since all participants are from the same service and the problem under analysis is the centrality of management and assistance in a PMR service.
Taking into account the starting question, we formulated the following research questions: What is the perception of specialist nurses in rehabilitation nursing about the structural component of the service for the development of their activity?; What is the perception of specialist nurses in rehabilitation nursing about the facilitating factors of the structure for providing care in a Physical Medicine and Rehabilitation unit?; What is the perception of specialist nurses in rehabilitation nursing about the factors that complicate the structure for providing care in a Physical Medicine and Rehabilitation unit?.
Given the nature of the study, we used a non-probabilistic convenience sample of RN with the inclusion criterion of being RN working in an PMR service. In this study, 16 RNs participated, which corresponds to all those who exercise functions in the service during the data collection period, whose characteristics we will describe.
Data collection and data analysis instruments
The data collection instrument used was a semi-structured face-to-face interview. The interview guide consisted of eight open questions and a set of eight questions for the sociodemographic and professional characterization of the participants. It was not entirely open, nor involved a rigid set of questions, the use of the semi-structured interview allowed, through the interaction between the interviewee/interviewer, the emergence of questions and data that, not having been previously considered, contributed to the enrichment of the collected information. The recording of the interviews was carried out through audio recording, after authorization from the participants. In order to guarantee anonymity, all interviews were coded with the initial letters of the words Nurses and Rehabilitation, followed by the number: ER1, ER2, ER3, etc.
The data analysis base was framed in the perspective of Bardin (2009). The content analysis proposed by the author is composed of a set of communication analysis techniques, a systematic and objective methodology that is developed in stages: pre-analysis, material exploration and, finally, the inference and interpretation of results obtained 7. After validating the content of the interviews by each participant, we created 16 documents constituting the analysis corpus that were later submitted to the Atlas.ti 22 software, designed for qualitative data analysis. The whole exploration of the expressions of the participants was coded by two separate researchers, followed by a moment of conciliation of the categories that did not coincide between the two, where the meaning of the expressions was defined from the definitions developed by the researchers.
Ethical considerations
After planning the study, it was submitted to the ethics committee of the hospital institution, with a favorable opinion expressed in Nº 51/22 (we did not identify the hospital institution to guarantee the confidentiality of the data). To guarantee the reliability of the data obtained, the recording of the interviews was carried out through audio recording, after informed consent. The meeting with the participants was confirmed in advance through telephone contact, according to the availability of each participant. The interviews took place between March 2022 and June 2022, in a reserved space at the hospital institution.
RESULTS AND DISCUSSION
Quality in health is designed with some peculiarities, in such a way that specific models emerge for its development, with particular emphasis on the Donabedian model, which, although already a few years old, is still maintained in the most current scientific references and in institutions national and international public 8, which is why it was selected as a support model for this study.
The structure component influences people's behavior and, consequently, the quality of care provided. In certain aspects, it can be the main determining factor of the quality of care, and the participants incorporate it into their speeches in two categories: people management and leadership in the service and physical environment and conditions for the functioning of nursing practices 4.
The nursing profession is mostly made up of women and the characteristics of the participants follow this trend, with the nursing team made up mostly of female nurses (81.3%). As for age, the study participants have an average age of 40.88 years old (standard deviation 6.5 years old), with the oldest being 57 years old and the youngest being 30. Regarding marital status, 68.8% are married, 18 .8% single and 12.5% divorced.
Although the majority are licensed (81.3%), three are masters: one in Rehabilitation Nursing, another in Management and Leadership of Nursing Services and another in Public Health. It should be noted that in the RN, the time working in the specialty area varies between 1 and 14 years, with an average of 7.31 years (standard deviation of 3.6 years). Their professional experience as nurses ranges from 10 to 36 years, with an average of 18.19 years (standard deviation of 7.03). When analyzing the exercise time in the service, we verified an interval of 1 to 10 years, with an average of 6.56% (standard deviation 3.6).
During the interviews, following the participants' speeches and the theoretical review carried out, it made sense for the researchers to create categories in advance, which guided and facilitated the organization of the findings. The theoretical references of Afaf Meleis and Dorothea Orem, the model of Donabedian (2003) and the regulatory instruments of professional practice theoretically supported the identification of categories and subcategories. Following the analysis carried out, in table nº1 the identified categories and subcategories are explained.
Table nº 1 Description of categories and sub-categories
| THEME AREA | CATEGORIES | SUB-CATEGORIES |
|---|---|---|
| STRUCTURE | PEOPLE MANAGEMENT AND SERVICE LEADERSHIP | Moments of reflection on practice |
| Recognition of nurses' training | ||
| PHYSICAL ENVIRONMENT AND CONDITIONS FOR THE OPERATION OF NURSING PRACTICES | Space available in the service | |
| Specialist nurse/patient staffing and ratio | ||
| Ongoing and in-service training | ||
| Work methodology |
The Structure encompasses relatively stable elements of an organization, namely the physical elements (material resources and characteristics of the physical environment), the characteristics of human resources in quantity and quality and also the organizational structure, representing key factors in the provision of care. However, the elements referring to the structure of an organization, by themselves, are not enough to guarantee the quality of health care 4.
The specificity of the PMR service adds particularities to the structural aspects, particularly the physical structure of the service and the nature of the human resources available to assist the patient with dependence.
It is also evident that the structure includes the policies of the hospital institution expressed with particularities at the service of PMR. The analysis of the discourses on the factors of the structure dimension, lead us to consider an association between the moments of reflection on the practice, the recognition of the training and the space available in the service, as shown in the following diagram (Diagram nº1).
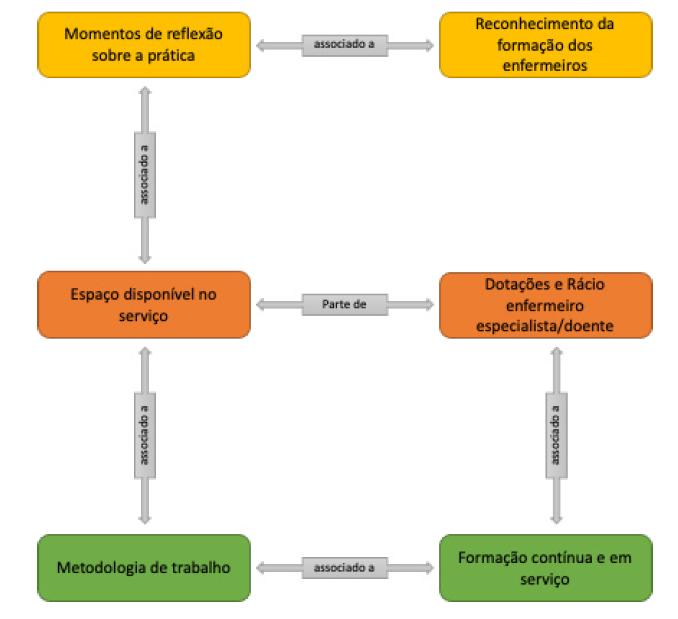
Participants consider that the fact that they are specialists in rehabilitation nursing makes them more sensitive to issues of available space, mentioning that “The fact that we are from rehabilitation we are better trained and more aware of this type of issue, recognizing the importance of having space for work with the patient” (ER9).
The available space is associated with the work methodology as well as with moments of reflection on the practice. The opportunity for the nurses to collaborate in the construction of the service project was fundamental from the perspective of the participants, “When we came to open this service, (...) we had the opportunity, together with the person responsible for the works, with the nurse director and with the supervising nurse, testing with wheelchairs, all entrances and exits of all compartments of this service, which contributed immensely to us being able to work in a place with all the conditions, which would not happen if it were a service not aimed at rehabilitation. (...) they even gave us the opportunity to eliminate walls that were in the initial project... test washbasins (...) some things were already in place, and we couldn't change, but we still managed to change others” (ER9).
Continuous and in-service training is associated with the need for staffing and work methodology. In fact, although the reflection generated in the context of training can contribute to the qualification of the work methodology used in the PMR service, these moments can only occur if the nursing staff guarantee, in the first instance, a safe response to the needs of patients. interned. As one nurse mentions, “The ratio also ends up helping with the quality of care provided, because if it were to replace patients, it would not be necessary, for example, 4 nurses in the morning shift (…) here it is different because for patients to evolve they need the quality of our specialized care” (ER7).
In this regard, the participants consider continuous and in-service training an excellent learning strategy, mentioning that “(...) continuous training is very important (...) in this service, the sharing between us, service meetings and training in service in relation to specific rehabilitation themes should still be more frequent (...) the problem is that there is not always time for everything” (ER8). As mentioned by another participant, “I think that the training sessions are great learning moments” (ER15).
People management and service leadership
The management of people and leadership has a preponderant role in the organizations, becoming fundamental in the competitiveness and in the changes of the services.
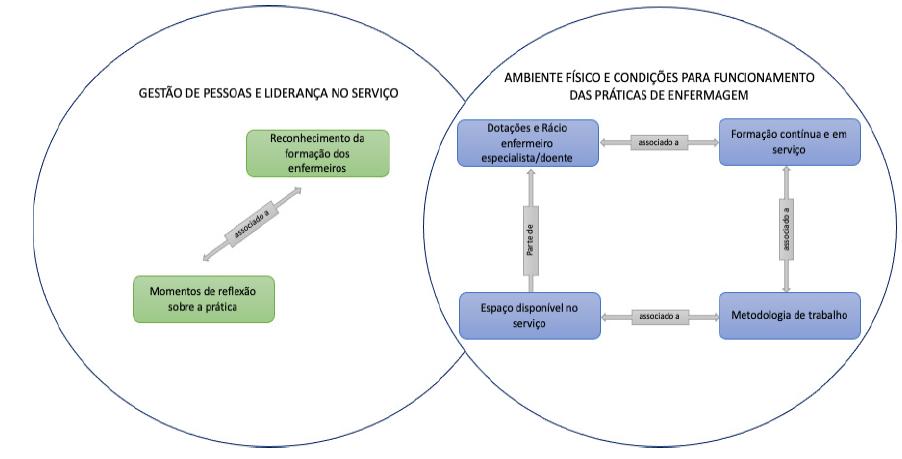
Once the identified associations were clarified, it is important to highlight that from the analysis of the participants' speeches, within the scope of the structure dimension, two categories emerged: people management and leadership in the service and the physical environment and conditions for the functioning of nursing practices. It should be noted that in the speeches these categories emerge in an intimate interaction between them, as shown in the following diagram (Diagram nº2).
In the people management and service leadership category, the participants argue that nurses with management functions should promote more moments of reflection on the practice “(...) the ideal would be to have time, and I am not talking about our own time, service time to be able to reflect on what we do. When we invest in any training it is with our personal time and I think that a different modality should be introduced in our daily lives, which would be for us to be able to evolve theoretically and in practice and these aspects are more balanced” (ER4).
Reflection on practice has been highlighted by several authors as an excellent strategy to improve the quality of care, namely Stonehouse, who mentions that finding time to stop and think is often impossible, however, reflective practice beyond of qualifying the decision-making process, it promotes the achievement of more positive results for the team and mainly for the clients 9. Any decision-making process can be improved, and the truth is that in the professional context, the positive points need to be recognized and valued, particularly by nurse managers.
As another participant reinforces, “there are things that I would like to see different here in this service, it is a service with a lot of potential, that we could do many things, that we could reflect more on the practice (...)” (ER13). In the same vein, other authors consider that reflection on practice is considered a key skill in the professional development of nurses, allowing them to become more self-aware and, consequently, improve the provision of care 10.
Most participants, due to the type of service, mention that their post-graduate training is recognized, especially regarding the opportunity to provide care within the scope of specialization in rehabilitation nursing “I was given the opportunity and, therefore, the focus of my work is the training of activities of daily living, I am a specialist nurse in rehabilitation nursing” (ER7), and in the same line of thought, they add “I perform everything related to general care and specialty nursing ( ...) (ER1). Regarding this finding, in Santos' perspective, it is effectively up to the manager nurse to coordinate, promote and increase measures and create conditions for the RN to assume themselves as reference nurses, especially in the case of patients with significant self-care needs 11.
The participants themselves value their postgraduate training in the context of professional practice, stating that “(...) our training is very complete, sometimes we may just have to look for some information to remember certain things” (ER2), but the truth is that “We have more training and are more aware of what we need to do.” (ER5). Postgraduate training in the area of rehabilitation nursing is of particular importance, as it makes it possible to deepen knowledge and develop essential skills to respond to health challenges. Currently, the intervention of the RN is clear and is explicit in health outcomes and people's satisfaction 12.
Participants representatively valued moments of reflection on the practice and recognition of nurses' training. Moments of reflection on practice contribute significantly to the quality of care but require time available for discussion. On the other hand, the recognition of training becomes an act of valuing formal and informal training, in the words of the participants.
Physical environment and conditions for the functioning of nursing practices
In the category physical environment and conditions for the functioning of nursing practices, four sub-categories emerged from the participants' speeches: available space in the service, staffing and specialist nurse/patient ratio, continuous and in-service training and work methodology.
Participants refer that the space available in the service is adequate to the needs of patients, remembering that “the service was created from scratch, albeit with some limitations (...) but from the outset it is a service that has a different type of attention. The fact that we have more bathrooms, the wards have only two beds (...) the service is adapted for patients and for our rehabilitation nursing practice, which is a process that facilitates our work” (ER1).
The sensitivity of the RN to environmental issues has already been addressed by other authors, namely Pereira and collaborators, who highlighted that the RN’s aim, in their specialized practice, to promote well-being and quality of life, developing at the same time maximize the health potential of people with disabilities by promoting mobility and accessibility, which effectively requires environmental conditions 13. In this context, other authors addressing the competences of the RN, praise their role in promoting more inclusive environments, and their involvement in improving accessibility conditions should exist 14. Although this involvement is fundamental, in the context in which the person lives, it must be a reality in each service where specialized rehabilitation care is provided, not least because without these structural conditions, it will be difficult to instruct and train strategies that promote the qualification of people to the self-care.
Environmental issues are decisive for the care provided by professionals, but essential for people who need their care. What is certain is that, as one participant stresses, “compared to other services, our physical structure is minimally adapted for this type of patient.” (ER15). Even so, other participants recognize opportunities for improvement “We have a physical structure that allows us to work with patients, but for example the bathrooms and shower spaces should be bigger, and the showers be equipped with mirrors. The wards have two beds, which is very good, but if they only had one, it would be better to simulate the patient's house.” (ER14).
Usually the common concept of structure focuses on the physical environment and material resources, but as Donabedian points out, human resources are also part of the structure 4. The participants, in the area of physical conditions, pointed to the space available in the service as a favorable condition for the development of care, however, they point out as suggestions for improvement: the need to equip the shower spaces with mirrors. It is necessary that environments meet accessibility conditions in order to respond to the needs of each individual, so that their total integration occurs, without any difficulty 13. In the PMR service, the participants report having good conditions, however, it will be necessary to think about them in terms of the interface with the patient's reality, in their home, for the training that begins in hospitalization.
As for staffing and the specialist nurse/client ratio, the participants considered it appropriate, stating that “In this service we have good ratios, in terms of nurses as assistants (…) mainly in the morning shift, (…) it helps us to have more time to provide care”. care for patients and care more calmly (...) give patients time to do things, in other services this no longer happens because they have fewer people working.” (ER2). This reality is not frequent in other contexts, with several authors actually mentioning ratios that are out of line with the needs of people in nursing care and, especially in specific rehabilitation. In an investigation carried out in Portugal on the environments of nursing practice, it was found that the perception of quality was unfavorable in most Portuguese hospitals, namely the dimension of human resources was one of the most critical quality components 15.
In the context of rehabilitation nursing care, there is no adequacy of human resources in health organizations 14, contrary to what one of the participants states, who considers “(...) from the point of view of staffing, we are not bad ( …) I even think we are doing very well in terms of ratios. (ER4).
The participants consider that the ratios have an impact both on the quality of care and on promoting the patient's autonomy. As a result of the concern to provide care in a partially compensatory pattern and with a view to evolving towards a support/education pattern, the RN recognize the value of the time they can spend with each patient “we have a very good ratio that allows us to spend the time with the patient time he needs, namely in promoting autonomy in self-care” (ER14). In the provision of care, the Order of Nurses in Regulation No. 743/2019, defined the appropriate number of nurses in each work context, thus promoting favorable rates of quality and safety of care. In specialized centers and internment services for MFR, they must have 75% of RN, having to guarantee that at least one RN remains 24 hours a day 16.
The complexities associated with health care, specifically nursing and rehabilitation nursing care, require adequate staffing to ensure safety and quality in different contexts, as is the case of the PMR. The concept of safe staffing in nursing is dynamic and comprehensive, where the number of nurses is considered and their skills are valued, in order to guarantee the provision of safe care. This means that it is not only the number that is at stake, but also the skills, experience, training and motivation 17. Most study participants refer to staffing only in the sense of the specialist nurse/patient ratio, with good ratios for the assistance required in the service being predominant, but they warn of the need for more time to provide care, in order to guarantee time for the patient to develop independence and autonomy.
With regard to in-service training, the participants state that it can make an important contribution to the organization and guidance of nursing practice “I think there should be more in-service training, because then we end up investing more in training or congresses. We should plan in-service training throughout the year” (ER5), not least because, as one participant mentions, “in-service training in recent years has been completely reduced (...)” (ER9). The contribution of in-service training to nursing practice allows theoretical knowledge to be contextualized in solving real problems in the practice of nursing care. In this sense, and through in-service training, organizations can create reflective environments, for team learning, which promote professional autonomy, as well as intercommunication between all stakeholders 18.
Continuous and in-service training takes paths that range from informal training to formal training, including self-training with emphasis on the job, which effectively becomes a unit within the pillar of the structure. All participants embodied the subcategory continuous and in-service training, bringing to the discussion its importance in guaranteeing a structure adequate to quality, from the person's own investment, outdoor training (conferences, workshops) and indoor training (in-service), in addition to the current ease of the e-learning methodology. The weakness identified by the participants is the lack of an in-service training plan, considering the specificity of the care and techniques developed in the PMR services. Given the contributions of in-service training to guarantee the quality of care, it is necessary to adopt strategies that allow reflections on practice, with an impact on the design and delivery of nursing care 20.
As for the work methodology, the opinions among the participants differ, with some considering that the methodology adopted in the service - reference nurse - is a facilitating aspect of promoting the quality of care, however, they point out that this method has already been more efficient and complete , “We should follow the reference nurse method as it used to be, that (…) we had home visits and meetings with the family, we should take this further (…)” (ER1). As one participant clarifies, “We have the reference nurse method, which at the moment is only based on updating the patient's care plan assigned to us” (ER3). The reference nursing method is internationally recognized, it consists of a strategy of individualized responsibility in decision-making, in relation to nursing care 21.
For some participants, the reference nurse method remains the most appropriate “We have the reference nurse method (...) which allows us to have a view of the patient, because each nurse is associated with a patient, and, although not we always stay with that patient, we assess the patient and manage the care plan” (ER8).
On the other hand, some participants consider the reference nurse method a difficult aspect, “In this service I do not consider the reference nurse method the most appropriate, sometimes with the distribution I can spend more than two weeks without being with my patient reference and then I practically don't know him, (...) now if they ask me what would be the most appropriate method, I think we would have to reflect on that” (ER13). In this follow-up, two participants chose the individual method as a guide for their professional practice, “I think we should have an individual method of work” (ER6), “In my perspective, the method of work should be mostly individual so that each nurse is responsible for everything that concerns its users” (ER10).
In the scientific community, the work methodology has been the subject of discussion, however, it is certain that this is an integral part of the nurses' work process. The selection of a nursing work method reflects the type of conceptualization, organization and provision of care in a given context. And for that reason, they translate a perspective, a way of thinking and organizing nursing practice 22.
It should be noted that the RN, in the organization of work, may adopt various methods, in order to respond to the complexity and differentiation of care. However, given the specific skills of these professionals, the choice of reference nurse and/or case manager methods will be effectively the most relevant, in terms of satisfying people's real needs 23.
The Nursing Order recognizes the need to organize nursing care with an emphasis on the use of methodologies that promote quality and safety, allowing an integrated response to patients' problems. Participants are divided in their opinion between the reference nurse method and the individual method, emphasizing the need to particularly improve the daily distribution strategy 24.
Let us remember that in the work methodology, the most mentioned method is the reference nurse method, also referred to as responsible nurse or Primary Nursing. Nurses are assigned one or more patients and are responsible for planning, executing and evaluating care, from admission to discharge, whenever they are on duty. The fragility identified by the participants is related to the lack of respect for the maintenance of the dyad, responsible nurse/patient, when the work is distributed, which conflicts with the design of the method. The method foresees that the services will have two types of nurses, the reference and the adjuncts/associates, which will facilitate the distribution of patients in the absence of the reference nurse. This method values the nurse's responsibility considering that the reference nurse, in addition to being responsible for the patient, coordinates and supervises care throughout the hospitalization 21,22.
In opposition to the methodological practices of the organization of care, where the use of the reference nurse method is mentioned, participants appear to defend the individual method, which consists of a care approach to the patient as a whole, where the nurse assumes daily responsibility for care for all distributed patient care 21. Recently, some studies have emerged that demonstrate associated weaknesses, considering that the nurse's responsibility is limited to the work shift in which the patient is distributed 22.
Rehabilitation nursing can mean a philosophy of care based on rehabilitative and recovery principles, which implies skills on the part of nurses to intervene in functional, psychological, educational and social terms. With the aim of seeking health, independence in self-care and adapting to healthy lifestyles, well-being and quality of life, it requires knowledge that goes beyond promoting self-care, as it involves the person as a whole, reasons that make this area of intervention a differentiating specialty from others 25. The particularity of this study constitutes the analysis of the structure in order to guarantee conditions for the achievement of the process and thus demonstrate the results of assistance in the PMR service.
CONCLUSION
From this study, it was possible to observe and analyze the perception of the RN in relation to the quality of care in the PMR Units regarding the Structure from which the following categories emerged: people management and leadership in the service and physical environment and conditions for the functioning of nursing practices.
Although in most contexts, the contribution of RN is recognized and valued, studies that seek to qualify professional practice through in-depth analysis of the practices of these professionals are rare. In this context, this qualitative study allowed a reflection on the problem and identified strategies for improving professional practice.
The factors that facilitate the provision of care in a Physical Medicine and Rehabilitation unit concern the structure of the service, the type of work they develop and what motivates them, thus contributing to professional satisfaction and to the service, showing up in their well-being and motivation.
The factors that hinder the provision of care in a Physical Medicine and Rehabilitation unit are related to continuous and in-service training, as well as the lack of moments of reflection on practice. The work method emerges as a difficult contribution for some nurses, while for others it is an added value for the accountability of the autonomous practices developed.
Donabedian's model (2003) supports the perception of the RN in terms of what is considered adjusted to the practice of nursing and a contribution to the organization and control of the quality of care in PMR services. Rehabilitation nurses perceive the organization of care based on particular aspects of the structure, relating them to their skills.
The course of this study added value to the researchers' learning; however, we identified limitations in deepening the problem under study, which allows us to leave the suggestion of developing a new investigation with research/action methodologies on the practice of RN in a PMR service.
REFERENCES
1 Ward, A. & Gutenbrunner, C. Physical and Rehabilitation Medicine in Europe. J Rehabil Med [Internet]. 2006 [citado 13 de Fevereiro de 2023]. 38: 81-86. DOI: 10.1080/16501970500477777; [ Links ]
2 Sampaio, F., Pinto, C., Parada, F., Antunes, F., Silva, H., Caldas, J., André, L. & Mirco, T. Rede Nacional de Especialidade Hospitalar e de Referenciação - Medicina Física e de Reabilitação [Internet]. Ministério da Saúde. 2017 [citado 13 de Fevereiro de 2023]. Disponível em: https://www.acss.min-saude.pt/wp-content/uploads/2017/03/RNEHRMedFisicaReab_vf.pdf; [ Links ]
3 Queiroz, E. & Araújo, T. Trabalho de equipe em reabilitação: um estudo sobre a perceção individual e grupal dos profissionais de saúde. Paidéia [Internet]. 2009; 19 (43): 177-187; [ Links ]
4 Donabedian, A. An Introduction to Quality Assurance in Health Care. Oxford: University Press. 2003; [ Links ]
5 Ordem dos Enfermeiros. Regulamento n.º 392/2019 - Regulamento das Competências Específicas do Enfermeiro Especialista em Enfermagem de Reabilitação [Internet]. 2019. Diário da República II Série, n.º 85: 13565-68. Disponível em: https://www.ordemenfermeiros.pt/media/11871/1356513568.pdf; [ Links ]
6 Streubert, H. & Carpenter, D. Investigação qualitativa em Enfermagem - Avançando o Imperativo Humanista. (5ª ed.). Loures: Lusociência. 2013. [ Links ]
7 Bardin, L. Análise de conteúdo. Lisboa: Edições 70. 2009; [ Links ]
8 Organização Mundial da Saúde. Orientações da OMS para a cirurgia segura 2009: cirurgia segura salva vidas. Direção-Geral da Saúde. 2010. Disponível em: https://apps.who.int/iris/bitstream/handle/10665/44185/9789241598552_por.pdf;jsessio; [ Links ]
9 Stonehouse, D. Reflective practice: Ensuring quality care. British Journal of Healthcare Management [Internet]. 2015 [citado 20 de Fevereiro de 2023]. 21(5): 237-241. Disponível em: https://www.researchgate.net/publication/276238398_Reflective_Practice_Ensuring_Quality_Care; [ Links ]
10 Peixoto, N. & Peixoto T. (2016). Prática reflexiva em estudantes de enfermagem em ensino clínico. Revista de Enfermagem Referência [Internet]. 2016 [citado 20 de Fevereiro de 2023]. 4(11): 121-132. Disponível em: http://dx.doi.org/10.12707/RIV16030; [ Links ]
11 Santos, M. A gestão e a liderança em serviços de enfermagem de reabilitação. In O. Ribeiro, Enfermagem de Reabilitação conceções e práticas. Lidel. 2021. p.19-27; [ Links ]
12 Padilha, J., Martins, M., Gonçalves, N., Ribeiro, O., Fernandes, C. & Gomes, B. Olhares sobre os processos formativos em enfermagem de reabilitação. Revista Portuguesa de Enfermagem de Reabilitação [Internet]. 2021 [citado 20 de Fevereiro de 2023]. 4(1): 83-89. Disponível em: https://doi.org/10.33194/rper.2021.v4.n1.178; [ Links ]
13 Pereira, P., Martins, M. & Machado, W. Enfermagem de Reabilitação e a pessoa com deficiência: o caminho para a inclusão social. In O. Ribeiro, Enfermagem de Reabilitação conceções e práticas. Lidel. 2021. p.430-449; [ Links ]
14 Silva, C., Oliveira, F., Ribeiro, M., Prazeres, V. & Ribeiro, O. Novos desafios para velhos problemas: o enfermeiro especialista em enfermagem de Reabilitação na promoção da acessibilidade. Revista Portuguesa de Enfermagem de Reabilitação [Internet]. 2019 [citado 2 de Fevereiro de 2023]. 2(2): 20-26. Disponível em: https://doi.org/10.33194/rper.2019.v1.n2.02.4561; [ Links ]
15 Jesus, E., Roque, S. & Amaral, A. Estudo RN4CAST em Portugal: Ambientes de Prática de Enfermagem. Revista Investigação em Enfermagem [Internet]. 2015 [citado 2 de Fevereiro de 2023]. 26-44. Disponível em: https://repositorio.ucp.pt/bitstream/10400.14/19776/1/2015066.pdf; [ Links ]
16 Ordem dos Enfermeiros. Regulamento n.º 743/2019 - Regulamento da Norma para Cálculo de Dotações Seguras dos Cuidados de Enfermagem [Internet]. 2019 [citado 2 de Fevereiro de 2023]. Diário da República, II Série, n.º 184: 128-155. Disponível em: https://dre.pt/dre/detalhe/regulamento/743-2019-124981040; [ Links ]
17 Freitas, M., Parreira, P. & Neves, T. Dotação Segura em Enfermagem. In Parreira, P., Castilho, A., Martins, M., Santos, M., Rocha, M., Souza, M. - Gestão nas organizações de saúde - Pessoa, formação e desenvolvimento profissional (1ªed.). Portugal: Ordem dos Enfermeiros, Associação de Apoio aos Cuidados de Saúde dos Pequenitos. 2022; [ Links ]
18 Ferreira, R. & Amendoeira, J. Resultados sensíveis em enfermagem. Ensaio: modelo de avaliação da qualidade dos cuidados. Revista da UIIPS. 2015; 5 (3):396-407; [ Links ]
19 Martins, M. & Fernandes, H. O Trabalho do Enfermeiro Gestor em Unidades de Saúde. In Parreira, P., Castilho, A., Martins, M., Santos, M., Rocha, M., Souza, M. - Gestão nas organizações de saúde - Pessoa, formação e desenvolvimento profissional (1ªed.). Portugal: Ordem dos Enfermeiros, Associação de Apoio aos Cuidados de Saúde dos Pequenitos. 2022; [ Links ]
20 Martins, M., Ribeiro, O. & Bastos, A. Formação em Serviço. In Parreira, P., Castilho, A., Martins, M., Santos, M., Rocha, M., Souza, M. - Gestão nas organizações de saúde - Pessoa, formação e desenvolvimento profissional (1ªed.). Portugal: Ordem dos Enfermeiros, Associação de Apoio aos Cuidados de Saúde dos Pequenitos. 2022; [ Links ]
21 Ventura-Silva, J., Martins, M., Trindade, L., Ribeiro, O. & Cardoso, M. Métodos de trabalho dos enfermeiros em hospitais: scoping review. Journal Health NPEPS [Internet]. 2021; 6(2): 278-295. Disponível em: https://docs.bvsalud.org/biblioref/2021/12/1349325/document-7.pdf; [ Links ]
22 Parreira, P., Costa, P., Neri, M., Marques, A., Queirós, P. & Oliveira, A. Métodos de trabalho para prestação de cuidados de enfermagem. In Parreira, P., Castilho, A., Martins, M., Santos, M., Rocha, M., Souza, M. - Gestão nas organizações de saúde - Pessoa, formação e desenvolvimento profissional (1ªed.). Portugal: Ordem dos Enfermeiros, Associação de Apoio aos Cuidados de Saúde dos Pequenitos. 2022. [ Links ]
23 Silva, J., Martins, M., Trindade, L., Ribeiro, O., Ribeiro, M. & Cardoso, M. O processo de trabalho dos enfermeiros especialistas em enfermagem de reabilitação numa ótica marxista. Revista Portuguesa de Enfermagem de Reabilitação [Internet]. 2021; 4(2): 72-80. Disponível em: https://doi.org/10.33194/rper.2021.73; [ Links ]
24 Ordem dos Enfermeiros. Regulamento do Perfil de Competências do Enfermeiro de Cuidados Gerais [Internet]. Lisboa: Ordem dos Enfermeiros. 2012 [cited 2023 Fev 21]. Disponível em: http://www.ordemenfermeiros.pt/publicacoes/Documents/divulgar%20-%20regulamento%20do%20perfil_VF.pdf; [ Links ]
25 Schoeller, S., Martins, M., Ribeiro, I., Lima, D., Padilha, M. & Gomes, B. Breve panorama mundial da enfermagem de reabilitação. Revista Portuguesa de Enfermagem de Reabilitação [Internet]. 2018 [citado 21 de Fevereiro de 2023]; 1(1): 6-12. Disponível em: https://doi.org/10.33194/rper.2018.v1.n1.01.4388. [ Links ]
Ethics Committee: Study authorized by the Ethics Committee of the Centro Hospitalar Universitario de São João (Opinion No. 51/22).
Declaration of informed consent: Written informed consent to publish this study was obtained from the participants.
Received: March 10, 2023; Accepted: May 04, 2023; Published: May 26, 2023
 Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
