










Serviços Personalizados
Journal
Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkRevista Portuguesa de Enfermagem de Reabilitação
versão impressa ISSN 2184-965Xversão On-line ISSN 2184-3023
RPER vol.2 no.1 Silvalde jun. 2019
https://doi.org/10.33194/rper.2019.v2.n1.05.4565
Articles
Physical exercise in the person with depressive disorder: A Systematic literature review
1
 http://orcid.org/0000-0001-6943-1499
http://orcid.org/0000-0001-6943-1499
2
http://orcid.org/0000-0002-6767-2421
1
http://orcid.org/0000-0002-7004-4792
2
http://orcid.org/0000-0002-9358-4011
1- Centro Hospitalar Universitário Lisboa Central Hospital Curry Cabral, Portugal
2- Centro Hospitalar Lisboa Norte, Hospital Santa Maria, Lisboa, Portugal
3- . Escola Superior de saúde Atlântica, Barcarena, Portugal
4- Universidade de Évora, Escola Superior de Enfermagem S. João de Deus, Évora, Portugal
Background:
Depressive disorder is currently one of the most common forms of mental disorder and one of the greatest causes of health problems. There has been a need to combine the pharmacological approach with adjuvant treatment such as psychoterapy and physical exercise in the treatment of this disorder.
Method:
Systematic Literature Review that was based on the recommendations of the Joanna Briggs Institute on PICO strategy and based on PRISMA. The research question raised was “What are the benefits of physical exercise in people with Depressive Disorder?”. The research was carried out using the electronic database platforms: EBSCOHost and B-on.
Results:
A sample of nine studies was included that fulfilled the eligibility and methodological quality criteria, where the type, volume, frequency and duration of the physical exercise practiced in each of the studies were described and analyzed.
Conclusions:
The results obtained allow us to conclude that regardless of the frequency, duration and intensity of physical exercise in depressive disorder, it decreases the depressive symptoms, improving also the physical fitness, the cognitive function and the well-being of the person with this disorder.
Key words: Exercise training; physical activity; depressive disorder; rehabilitation nursing
Introdução:
A depressão é das formas mais comuns de distúrbio mental e uma das maiores causas de problemas de saúde da atualidade. Tem surgido a necessidade de aliar ao tratamento farmacológico, tratamentos adjuvantes tais como a psicoterapia e a prática de exercício físico, no tratamento deste transtorno.
Método:
Revisão Sistemática da Literatura, que utiliza as recomendações do Joanna Briggs Institute na estratégia PICO e as recomendações PRISMA, foi formulada a questão de pesquisa “quais os benefícios do exercício físico na pessoa com transtorno depressivo?” A pesquisa foi realizada com recurso a plataformas de bases de dados eletrónicas EBSCOhost e B-on.
Resultados:
Foram incluídos nove estudos que cumpriam os critérios de inclusão, e onde se descreveram e analisaram o tipo, frequência, volume e duração de cada modalidade de exercício físico praticado em cada um dos estudos.
Conclusões:
Os resultados obtidos permitem concluir que independentemente da frequência, duração e intensidade da prática de exercício físico no transtorno depressivo, esta diminui os sintomas depressivos, melhorando também a forma física, função cognitiva e bem-estar da pessoa com transtorno depressivo.
Descritores: Transtorno depressivo; treino de exercício; atividade física; Enfermagem em Reabilitação
Introducción:
El trastorno depresivo es una de las formas más comunes de trastorno mental y una de las mayores causas de problemas de salud en la actualidad. Ha surgido la necesidad de aliar al tratamiento farmacológico, tratamientos adyuvantes tales como la psicoterapia y la práctica de ejercicio físico en este trastorno.
Objetivo:
Identificar cuales son los beneficios del ejercicio físico en una persona con un trastorno depresivo.
Método:
Revisión sistemática de la literatura, que utiliza las recomendaciones de Joanna Briggs Institute con la estrategia PICO y las recomendaciones PRISMA, se formuló la cuestión de investigación “ ¿cuáles son los beneficios del ejercicio físico en una persona con trastorno depresivo?” La búsqueda se realizó con recursos a plataformas de bases de datos electrónicas EBSCOhost y B-on.
Resultados:
Se incluyeron nueve estudios que cumplían los criterios de inclusión, y donde se describieron y analizaron el tipo, frecuencia y duración del ejercicio físico practicado en cada uno de los estudios.
Conclusiones:
Los resultados obtenidos permiten concluir que independientemente de la frecuencia, duración, volumen e intensidad de la práctica de ejercicio físico en el tratamiento depresivo, ésta disminuye los síntomas depresivos, mejorando también la forma física, función cognitiva y el bienestar de la persona con trastorno depresivo.
Palabras clave: Trastorno depresivo; entrenamiento de ejercicio; actividad física; Enfermería en Rehabilitación
INTRODUCTION
Depression is considered a mental disorder that is characterized by the manifestation of depressive episodes once or twice a week. These episodes are expressed by the loss of interest and pleasure in activities of daily living (ADL). Persistent mood changes associated with emotional, cognitive and behavioral symptoms translating into loss of self-esteem, feelings of guilt and incapacity1.
Depression is a prevalent disease throughout life that affects 10 to 20% of the population in different countries, being the main responsible for the disability caused by mental disorders and substance use (about 40.5% of the total years of life adjusted for disability)2.
People with depression, in many cases, have associated comorbidities, increasing the negative impact on their quality of life, not only in social activities and ADL, but also in the increase in hospitalizations and mortality3.
In order to counteract depressive symptoms, there is a growing need to find strategies and therapies that make it possible to reduce these symptoms. In this sense, the use of non-drug therapies, such as physical exercise, can have a positive effect on decreasing depressive symptoms. This is well tolerated by people with depressive disorder, with good adherence, but it has to be administered, prescribed, managed supported and/or carried out by health professionals with specific training in exercise prescription4. Physical exercise is understood as the planned, organized and repeated body movements in order to maintain or improve one or more components of physical fitness5. There is evidence that physical exercise is an adjunct to the treatment of major depressive disorder, with beneficial effects in people 6. Thus, with the systematic literature review (SLR), we intend to find an answer to the following question: what are the benefits of physical exercise for people with depression?
Thus, it is intended to identify the benefits of physical exercise for people with depression.
MATERIAL AND METHODS
A literature review aims to systematize the studies of clinical practice in health care, which can be expressed in various ways. SLR is defined as an investigation method focused on a clearly formulated question, which, through systematic, explicit and reproducible methods, allows the identification, evaluation and synthesis of studies with relevant evidence. This is carried out by researchers, academics and health professionals, allowing the collection and analysis of data from the studies that are included in the review7.
For the present study, an SLR to publications worldwide was carried out between January 2014 and November 2018.
The recommendations of the Joanna Briggs Institute (JBI) were considered, which resulted in the research question from the PICO strategy8-10, the research question was formulated “What are the benefits (O) of physical exercise (I) in the person with depressive disorder (P) compared to the control group (C)?” where each PICO dimension contributed to define the inclusion criteria: Population (P) - People with depressive disorder; Intervention (I) - physical exercise, and Comparison (C) - people with depression who do not exercise compared to a group of people with depressive disorder who are subject to complementary therapy, exercise, and Results (O) - benefits of physical exercise in people with depressive disorder.
The descriptors related to each of the components of the PICO strategy were previously validated in the Descriptors in Health Sciences and Medical Subject Headings platform. The following Keywords were also used: exercise training, physical activity, and depressive disorder.
The following were defined as inclusion criteria for articles: (Table 1) quantitative studies, published in the last 4 years (2014-2018), in Portuguese, English and Spanish, with accessible full text.
Table 1 Criteria of inclusion and exclusion.
| Inclusion criteria | Exclusion criteria |
|---|---|
| Person with Depressive syndrome (or simply) with depression. | |
| Experimental studies | Other quantitative studies, qualitative studies and systematic literature review. |
| Studies published between 2014 and 2018. | Studied published before 2014 |
| Studies published in Portuguese, English and Spanish. |
The research was carried out by four investigators simultaneously, in the period between October and November 2018, and for it the following databases were used: EBSCOHost and online library B-on.
The articles selected for full reading were independently evaluated by two investigators, according to methodological quality criteria proposed by the JBI8, with only articles with more than 75% of the criteria being selected.
Information was extracted from the articles on authors, year, country, sample, data on the intervention (frequency, intensity, volume, duration and modality), conclusions and level of evidence. The classification of the levels of evidence of the included studies was based on the criteria of the Registered Nurses Association of Ontario9,11.
RESULTS
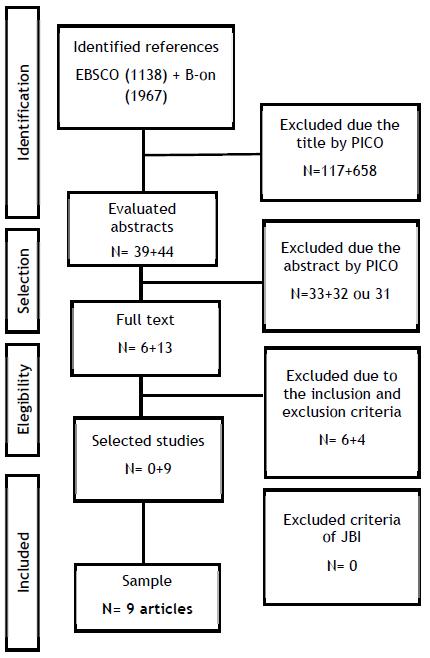
From the bibliographic research process carried out with this methodology, on the EBSCOhost platform we obtained 1,138 articles for initial selection. After insertion of the inclusion criteria, 156 articles were found. Out of these, 117 were rejected by title or subject and 33 by abstract. Out of the 6 resulting articles, all were excluded after analysis of the full text, as they did not meet the defined inclusion criteria.
By replicating the same methodology on the B-on platform, 1,967 articles were found, of which 702 articles were selected after insertion of the inclusion criteria. Of these, 658 were rejected by title or subject and 31 by abstract. Of the 13 resulting, 4 were excluded after reading the entire text, as they did not meet the defined inclusion criteria. As a final result, 9 articles that meet the inclusion criteria were obtained.
Table 2 describes the process of combining descriptors and keywords for searching the databases. Figure 1 illustrates the PRISMA12 flowchart corresponding to the identification, analysis, selection and inclusion of articles.
Table 2 Boolean Conjugation
| Boolean Conjugation | EBSCO | B-on |
|---|---|---|
| ((exercise training) OR (physical activity)) AND (depressive disorder) | ||
| Total of Articles | 1,138 | 1,967 |
In summary, 9 articles were included in this SLR that were published from 2015 to 2018.
The sample of people/participants in the different studies ranged between 1417 and 31021 and for the control group, the number of participants ranged between 617 and 31021. All studies included (table 2) are descriptive studies, with evidence level IB, that is, evidence obtained from a well-designed study, and from at least one randomized controlled study 10-11 (Table 3).
Table 3 Description of the included articles.
| Author, year, country | Participants | Objective | Intervention | Results | Evidence level |
|---|---|---|---|---|---|
| Minghetti et al., 2018, Switzerland 13 |
Total (n=59) Intervention group (n=29) (n=21 women n= 8 men) Control group (n=30) (n=25 women; n= 6 men) |
To evaluate the benefit of sprint interval training in people with depression compared to continuous aerobic exercise | Duration of study: 4 weeks Intervention Group: Modality - Interval sprint training on bicycle Frequency - 3 sessions/week Intensity - High Duration -25 sprint attacks of 30 seconds Volume - 2 sets and 4-6 reps Control group: Modality -Aerobic exercise Frequency - 3 sessions/week Intensity - Moderate Duration -20 min |
The practice of sprinting at short intervals has similar effects to the practice of aerobic exercise in people with depressive disorder. Both had beneficial effects in reducing depressive symptoms. | IB |
| Kerling et al., 2017, Germany14 | Total (n=30) Intervention group (n=20) (n=8 women; n=12 men) Control group (n=10) (n=4 women; n=6 men) |
To evaluate the benefit of sprint interval training in people with depression compared to continuous aerobic exercise | Duration of study: 6 weeks Intervention group: Modality - Aerobic and resistance exercises Frequency - 3 sessions/week Intensity - Moderate Duration - 45 minutes (25 minutes on bicycle and 20 minutes on resistance machine) Control group: Modality - Walking, ball games and stretching exercises Frequency - 3 sessions/week Intensity - Low Duration - 20 minutes |
There was a slight increase in muscle mass in the intervention group while in the control group there was a slight decrease in muscle mass. | IB |
| Kerling et al., 2015, Germany15
|
Total (n=42) Intervention group (n=22) (n=10 women; n=12 men) Control group (n=20) (n=6 women; n=14 men) |
To examine whether people receiving an exercise program as an adjunct to hospital treatment benefit in terms of physiological and psychological factors. | Duration of study: 6 weeks Intervention group: Modality - Static bicycle Frequency - 3 sessions/week Intensity - Moderate Duration - 45 minutes Control group: Modality - Walking, ball games and stretching Frequency - 3 sessions/week Intensity -moderate-intensity physical activity Duration - 20 minutes |
In people with depressive disorder, the practice of physical exercise as an adjuvant treatment improves physical/functional and psychological fitness. When depressive disorder and cardiometabolic disorders are present, physical exercise is recommended as adjuvant therapy. |
IB |
| Olson et al., 2015, USA16
|
Total (n=30) Intervention group(n=15) (n=11 women; n=4 men) Control group (n=15) (n=13 women; n=2 men) |
To evaluate the effect of moderate-intensity aerobic exercise on cognitive control, depressive symptoms and ruminative thoughts. | Duration of study: 8 semanas Intervention group: Modalities - Aerobic exercises (treadmill or static bicycle) Volume - Absent, continuous exercise Frequency - 3 sessions/week Intensity - Moderate Duration: - 45 minutes of continuous exercise Control group: Modalities - Stretching exercises Volume - 3 sets (20 second stretches, with a 40 second rest period between stretches) Frequency - 3 sessions/week Intensity - Light Duration - 30-40 minutes/week |
A moderate-intensity aerobic exercise program improves cognitive control (conflict management), ruminative thinking and reduced depressive symptoms in people with depressive disorder. These results supported the demand that exercise could be a neurobehavioral treatment for cognitive control in people with depressive disorder. |
IB |
| Haller et al., 2018, Germany17
|
Total (n=20) Intervention group (n=14) (n=10 women n=4 men) Control group (n=6) (n=3 men n=3 women) |
To evaluate the feasibility, acceptability and effectiveness of an individualized approach to physical exercise on a web platform for people with moderate to severe depression. | Duration of study: 8 weeks Intervention group Modality - Resistance (through elastic bands) and strength (running on treadmill) Volume - 3 sets (12 reps) Frequency - 1 to 2 times a week Intensity - Moderate Borg < 4 (reduce if Borg > 7) Duration - 0-60 minutes Control group Modality - resistance (through bands) and strength (running on a treadmill) Volume - 3 sets (12 reps) Frequency - 1 to 2 sessions/week Intensity - Moderate Borg < 4 (reduce if Borg > 7) Duration - 10-20 minutes |
Improved quality of life (subjective well-being and social performance), self-efficacy and physical activity. Decrease in depressive symptoms. |
IB |
| Carneiro et al., 2015, Portugal18
|
Total (n=26) Control group (n=10) (n=10 women) Intervention group (n=16) (n=16 women) (group 1: n= 9 moderate-intensity exercises. Group 2: n=7 low intensity exercises) |
To measure the effect of a structured and individualized physical exercise program, supervised by a physical education teacher, as a complement to antidepressant therapy in the treatment of women with depressive disorder. | Duration of study: 16 weeks Intervention group: Modality - Aerobic exercise (traditional games, indoor/outdoor natural circuit exercises with resistance bands, jump ropes, fitness balls, dance and brisk walk test - 6 minutes). Frequency - 3 sessions/week Intensity - Group 1: moderate Group 2: low (Borg scale) Duration - 45-50 minutes/week (10 minutes of warm-up, 30 minutes of aerobic exercise and 5 minutes of stretching) Control group: Group to perform only antidepressant drug therapy. |
A structured, supervised exercise program is suitable not only as an adjunct therapy but as a primary option. It improves quality of life, reduce depressive and anxiety symptoms. Simultaneously it improves the physical/functional fitness of the participants. As for the intensity of the exercises, there were no differences in results when comparing the intervention subgroups. |
IB |
| Pentecost et al., 2015, England19 | Total (n=60) Intervention group (n=30) (n=12 women; n=18 men) Control group (n=30) (n=17 women; n=13 men) |
To compare a group of people undergoing a self-help program based on behavioral activation under the supervision of a Psychological Wellness Practitioner with a group of people undergoing the same self-help program combined with physical activity. | Duration of study:12 weeks Intervention group: Modality - Self-help program (manual, assessment sessions with Psychological Wellness professionals and self-determination training teachings) associated with activities monitored by a pedometer, Frequency - 1 session/week Intensity - Light Duration - Evaluation and follow-up sessions from 25 to 35 minutes Control group: Modality - self-help manual associated with a set of low-intensity cognitive behavioral therapy interventions. Frequency - 1 session/week Intensity - Low cognitive intensity. Duration - assessment and follow-up sessions from 25 to 35 minutes |
Study results indicate that there was acceptance of the use of self-help manuals by participants as well as Psychological Well-Being professionals. In this study, people increased their levels of physical activity, monitored by a pedometer. This monitoring encouraged the establishment of new goals and changed the personal behavioral activation program. They understood the joint importance of activities as a method to aid their recovery and improved cognitive ability. |
IB |
| Ólafsdóttir et al., 2017, Iceland 20
|
Total (n=15) (n=12 women; n=3 men) Intervention group; (n=15) Control group: (n=15) The study was carried out in two periods with the same group of participants |
To know the effects of physical exercise in a group of people with depressive and anxiety disorder, comparing to the same group of people undergoing only Cognitive Behavioral Group Therapy Transdiagnosis. | Duration of study: De 5 a 8 semanas Intervention group: Modality - Aerobic Exercises Frequency - 3 sessions/week Intensity - Moderate Duration - 60 minutes Control group: Modality - Transdiagnostic Cognitive Behavioral Group Therapy Frequency - 1 session/week Duration - 120 minutes (behavioral therapy group) |
Physical exercise has beneficial effects in reducing depressive symptoms in people with depressive disorder and anxiety. The group, when submitted to physical exercise presented results a little better than when submitted to Transdiagnostic Cognitive Behavioral Group Therapy. |
IB |
| Helgadóttir et al.,21 2016, Sweden. |
Total (n 620) Control group (n=310) (n=310 women) Intervention group (n=310) (n=310 women) (group 1: n=106 low intensity, group 2: n=105 moderate intensity, group 3: n=99 High intensity) |
To verify the response between physical exercise performed at three levels of intensity, with similar frequency and duration, and the severity of post-treatment depression. Compare the various levels of intensity and severity of post-treatment depression. | Duration of study:12 Semanas Intervention group: Modality - Yoga, Mindfulness (group 1), aerobics classes (group 2), vigorous exercise (group 3) Frequency - 3 sessions/week Intensity - Group 1 - Low, Group 2 - Moderate, Group 3 - High Duration - 55 minutes Control group: Modality - Group to perform only Usual treatment of depressive disorders (TAU) |
The four groups showed a significant reduction in the Montgomery-Åsberg Depression Rating Scale (MADRS) scores at post-treatment. The reductions in the three exercise groups were similar (7.4 to 9.4 points), and in all of them greater than the reduction observed in the TAU group (5.4 points). Regarding the training intensities used, although the differences were not significant, there was a reduction of almost 2 points in the MADRS score in group 1 compared to group 2. |
IB |
DISCUSSION
In order to understand the benefits of physical exercise in people with depressive disorder, we analyzed different studies in which a variety of strategies were found, such as the use of physical exercise and/or cognitive-behavioral therapies to reduce depressive symptoms13-21.
Through research from different studies, it was possible to verify some similarities in the interventions used by the various authors, who used parameters such as modality, intensity, frequency, volume and duration of the different types of exercises.
Given the diversity of exercises presented by the authors, they were grouped according to the associated intensity. We were able to verify that the study by Minghetti et al.13, comparing two groups of people, in which one of them practiced interval sprint training (high intensity exercise) and the other continuous aerobic physical exercise (moderate intensity exercise), found benefits of both physical exercise practices in the treatment of depressive disorders. Thus, it was not clear whether high-intensity physical exercise had a better conditioning when it is compared to moderate-intensity exercise.
This same line of thought was found by Helgadóttir et al.21 who, when comparing the different types of intensities of physical exercise practice, did not find significant differences between them. However, it was found that in the low intensity exercise group (yoga) there was a reduction of almost 2 points in the MADRS score compared to the moderate/aerobic exercise group.
Olson et al. 16, go against what has already been described, since these authors also concluded that the practice of light intensity exercise allows for improvements in the cognitive level and in the reduction of depressive symptoms.
Shuch et al.2 report in their study that exercises of moderate to high intensity showed better results; however they highlight the fact that the study sample is small, being difficult to extrapolate.
But given the above, none of the articles managed to present advantages regarding the duration of the exercises. The exercise intensities ranged between light and moderate, with a variation in duration between 20-60 minutes(16-18.20), with the exception of the high-intensity exercises13 which was performed in sessions of 25 repetitions of lasting 30 seconds (followed by 30 seconds of total rest).
Regarding the frequency of exercises, it ranged from one to three times a week for a period ranging from four to sixteen weeks13-21.
It was found that the physical exercise performed more frequently16,18,21 allowed to obtain more evident improvements than for those ones who only performed it once or twice17,19.
When talking about the impact of physical exercise on people with depressive disorder undergoing pharmacological therapy compared to people with depressive disorder who underwent therapy at the behavioral level21, it was found that according to the MADRS score reductions in the three exercise groups were similar, and in all three were greater than the reduction observed in drug therapy. In the same perspective, Carneiro et al.18 found that the group of people undergoing pharmacological therapy combined with physical exercise had an improvement in quality of life and a reduction in depressive and anxiety symptoms, also improving physical fitness.
Pentecost et al.19 report that the use of self-help manuals in behavioral activation therapy with encouragement to exercise facilitated adherence to its treatment and proved to be an option to consider in the treatment of depressive symptoms.
In turn, Ólafsdóttir et al.20 concluded that physical exercise can be a highly recommended alternative to the detriment of the transdiagnostic cognitive behavioral group. Minghetti et al.13, on the other hand, found that the association of these brought significant improvements in the reduction of symptoms of depression. Therefore, combining a physical exercise program with antidepressant therapy and cognitive behavioral therapy15 resulted in an improvement in cardiovascular capacity and a reduction in metabolic risk factors.
In the same line of thought, Helgadóttir et al.21 also found that physical exercise helped to prevent somatic disorders, such as cardio and cerebrovascular diseases and metabolic diseases. Knapen et al.1 suggest that there is an improvement in the metabolic level. In addition to improving physical health, there was an improvement in terms of body image, coping strategies to deal with stress, consequently improving quality of life and independence in activities of daily living in elderly people with depression.
As the loss of muscle mass is a consequence of the depressive disorder, Kerling et al.14 concluded that the practice of regular aerobic exercise (resistance training) is effective in preserving mass in people with depression. However, the authors mentioned that more studies are needed to prove a concrete improvement in this field.
Knapen et al.1 also reveal that the implementation of motivational strategies in exercise plans seems to improve the motivation of people with depression, as well as their long-term adherence to exercise.
Shuch et al.2 also state that the results in the improvement of symptoms of depression using physical exercise are more evident when there are no other associated comorbidities and when the exercises were supervised by qualified professionals.
In other studies, it was possible to see evidence of physical exercise in reducing depressive symptoms. Tu et al.3 concluded that in people with stable heart failure and depression, physical exercise (aerobic and strength exercises) was beneficial in improving depressive symptoms and still has positive effects on self-esteem and social interaction.
Kerling et al.6 reveal that physical exercise has a positive impact on the serum concentrations of the neurotransmitter in the brain. An assessment of neurotransmitter levels before and after structured and supervised training in people with major depression has shown beneficial results and therefore exercise should be considered as an adjuvant treatment.
All these studies highlight the importance of physical exercise programs to be supervised by professionals with relevant training as it seems that the dropout rates of interventions decrease when given by these professionals (physical education teacher, health professionals, and instructors).
Practical implications
In general, all the studies included report that physical exercise is beneficial and that it promotes an improvement in the quality of life of people with depression and under pharmacological therapy13-21.
More than subjecting the person with depression to a rigid physical exercise plan, it must be kept active. Studies have shown that regardless of the modality, frequency and/or intensity used, the person needs to be motivated. For this, it is essential that the choice of physical exercise and/or physical activity is carried out according to personal tastes, as it increases the interest and motivation to practice it.
In view of these results, and knowing that people with depression show varying degrees of anxiety and lack of motivation, it is important that these physical exercise plans are carried out by qualified health professionals, as they allow for monitoring and maintenance of the exercise plan. In this way, there is a more personalized follow-up of the person and, whenever necessary, an adjustment in the exercise plan to obtain better results.
Study Limitations
The limitations found are related to the heterogeneity of the articles, namely the existence of articles that compare groups of people with major depression and a group of people with depression and anxiety. Others, in turn, make comparisons between groups that only perform pharmacological therapy versus groups that perform pharmacological therapy and perform physical exercise15. And still other studies compare groups undergoing behavioral therapies (cognitive behavioral group therapy16,20 and behavioral activation therapy19) versus groups performing physical exercise.
We were also faced with the heterogeneity of groups regarding gender. There is a predominance of the female gender13,16-18,20-21 in the studies presented, which causes a bias in replicating the studies for the population with depression.
The small number of people in the sample14,16-18,20 was also a limitation presented by some of the authors. As well as the difficulty of monitoring people in the execution and fulfillment of the interventions proposed by the study.
There is a consensus among the studies that physical exercise is beneficial, however, based on the points mentioned above, the variety of exercises was so extensive that it did not allow us to draw specific conclusions about the benefit that each exercise alone had in improving the depressive symptoms. It was not possible to establish a direct comparison between studies, with regard to the specific physical exercises used, since the selection of activities according to the degree of intensity was divergent between the studies, which made it impossible to make a specific conclusion for the selection of a certain type of exercise over another.
CONCLUSION
After the SLR, we can conclude that there is an improvement in quality of life, cognitive improvement, and decrease in depressive symptoms when practicing a training plan of exercises of light to moderate intensity under the supervision of health professionals in the treatment of depressive disorder.
The included studies recommend that the person with depression and under pharmacological therapy should remain physically active regardless of the type, frequency or intensity of physical exercise performed. In addition, the motivation, as well as the preference of physical activity to be practiced by the person with depression should be taken into account in detriment of a structured and rigid plan, thus obtaining better results.
Finally, the goal of depression treatment should not be limited to the remission of depressive symptoms, but focus on functional recovery, social participation and improvement of the person's physical health.
Considering the results obtained from this SLR, as well as its limitations, it seems essential to continue with the investigation in this field of knowledge, since physical exercise is a promising strategy and should be included as a treatment option for people with depression. And finally, objectively define the interventions and select the assessment instruments that allow measuring the level of effectiveness and also verifying the transferability of these interventions in other contexts.
REFERÊNCIAS BIBLIOGRÁFICAS
1 Knapen J, Vancampfort D, Moriën Y, Marchal Y. Exercise therapy improves both mental and physical health in patients with major depression. Disabil Rehabil.. 2015 Jul 31;37(16):1490-5. Acessível em: https://doi.org/10.3109/09638288.2014.972579 [ Links ]
2 Schuch FB, Vancampfort D, Richards J, Rosenbaum S, Ward PB, Stubbs B. Exercise as a treatment for depression: a meta-analysis adjusting for publication bias. J Psychiatr. Res. 2016 Jun 1;77:42-51. Acessível em: https://doi.org/10.1016/j.jpsychires.2016.02.023 [ Links ]
3 Tu RH, Zeng ZY, Zhong GQ, Wu WF, Lu YJ, Bo ZD, He Y, Huang WQ, Yao LM. Effects of exercise training on depression in patients with heart failure: a systematic review and meta-analysis of randomized controlled trials. Eur J Heart Fail.. 2014 Jul;16(7):749-57. Acessível em: https://doi.org/10.1002/ejhf.101 [ Links ]
4 Stubbs B, Vancampfort D, Rosenbaum S, Ward PB, Richards J, Soundy A, Veronese N, Solmi M, Schuch FB. Dropout from exercise randomized controlled trials among people with depression: a meta-analysis and meta regression. J Affect Disord.. 2016 Jan 15;190:457-66. Acessível em: https://doi.org/10.1016/j.jad.2015.10.019 [ Links ]
5 Santa-Clara H, Pinto I, Santos V, Pinto R, Melo X, Almeida JP, Pimenta N, Abreu A, Mendes M. Atividade física e exercício físico: especificidades no doente cardíaco. Rev Factores de Risco. 2015, 35:28-35. [ Links ]
6 Kerling A, Kück M, Tegtbur U, Grams L, Weber-Spickschen S, Hanke A, Stubbs B, Kahl KG. Exercise increases serum brain-derived neurotrophic factor in patients with major depressive disorder. J Affect Disord.. 2017 Jun 1;215:152-5. Acessível em: https://doi.org/10.1016/j.jad.2017.03.034 [ Links ]
7 Sousa LMM, Firmino CF, Marques-Vieira CMA, Severino S, Pestana HCFC. Revisões da literatura científica: tipos, métodos e aplicações em enfermagem. Rev Port Enferm Reabil. 2018; 1(1): 46-55. Acessível em: http://www.aper.pt/ficheiros/revista/rpern0.pdf. [ Links ]
8 The Joanna Briggs Institute (AT). Joanna Briggs Institute's user manual: version 5.0 system for the unified management. Assessment and Review of Information. Adelaide: Joanna Briggs Institute; 2011 Acessível em: http://joannabriggs.org/assets/docs/sumari/SUMARI-V5-User-guide.pdf [ Links ]
9 Sousa LM, Marques JM, Firmino CF, Frade F, Valentim OS, Antunes AV. Modelos de formulação da questão de investigação na Prática Baseada na Evidência. Rev Inv. Enferm. 2018; S2(23): 31-39. Acessível em: http://hdl.handle.net/20.500.12253/1287 [ Links ]
10 Sousa, LMM, Vieira, CMA, Severino, SS, Antunes, AV. A metodologia de Revisão Integrativa da Literatura em Enfermagem. Rev Inv. Enferm. 2017; S2(21): 17-26. Acessível em: http://hdl.handle.net/20.500.12253/1311 [ Links ]
11 Registered Nurses' Association of Ontario (CA). Falls Prevention: Building the Foundations for Patient Safety. A Self Learning Package. Toronto, Canada: Registered Nurses' Association of Ontario; 2007. Acessível em: https://rnao.ca/bpg/guidelines/resources/falls-prevention-building-foundations-patient-safety-selflearning-package [ Links ]
12 Moher D, Liberati A, Tetzlaff J, Altman DG, The PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement.PLoS Med. 2009; 6(7): e1000097. Acessível em: https://doi.org/10.1371/journal.pmed1000097. [ Links ]
13 Minghetti A, Faude O, Hanssen H, Zahner L, Gerber M, Donath L. Sprint interval training (SIT) substantially reduces depressive symptoms in major depressive disorder (MDD): A randomized controlled trial. Psychiatry Res. 2018 Jul 1; 265:292-7. Acessível em: https://doi.org/10.1016/j.psychres.2018.04.053 [ Links ]
14 Kerling A, Hartung D, Stubbs B, Kück M, Tegtbur U, Grams L, Weber-Spickschen TS, Kahl KG. Impact of aerobic exercise on muscle mass in patients with major depressive disorder: a randomized controlled trial. Neuropsychiatr Dis Treat.. 2018; 14:1969. Acessível em: https://doi.org/ 10.2147/NDT.S167786 [ Links ]
15 Kerling A, Tegtbur U, Gützlaff E, Kück M, Borchert L, Ates Z, Frieling H, Hüper K, Hartung D, Schweiger U, Kahl KG. Effects of adjunctive exercise on physiological and psychological parameters in depression: a randomized pilot trial. J Affect Disord. 2015 May; 177:1-6. Acessível em: https://doi.org/10.1016/j.jad.2015.01.006 [ Links ]
16 Olson RL, Brush CJ, Ehmann PJ, Alderman BL. A randomized trial of aerobic exercise on cognitive control in major depression. Clin Neurophysiol. 2017 Jun;128(6):903. Acessível em: https://doi.org/ 10.1016/j.clinph.2017.01.023 [ Links ]
17 Haller N, Lorenz S, Pfirrmann D, Koch C, Lieb K, Dettweiler U, Simon P, Jung P. Individualized Web-Based Exercise for the Treatment of Depression: Randomized Controlled Trial. JMIR mental health. 2018;5(4):e10698. Acessível em: https://doi.org/ 10.2196/10698 [ Links ]
18 Carneiro LS, Fonseca AM, Vieira-Coelho MA, Mota MP, Vasconcelos-Raposo J. Effects of structured exercise and pharmacotherapy vs. pharmacotherapy for adults with depressive symptoms: a randomized clinical trial. J Psychiatr Res. 2015 Dec 1;71:48-55. Acessível em: https://doi.org/ 10.1016/j.jpsychires.2015.09.007 [ Links ]
19 Pentecost C, Farrand P, Greaves CJ, Taylor RS, Warren FC, Hillsdon M, Green C, Welsman JR, Rayson K, Evans PH, Taylor AH. Combining behavioural activation with physical activity promotion for adults with depression: findings of a parallel-group pilot randomised controlled trial (BAcPAc). Trials. 2015 Dec 1;16(1):367. Acessível em: https://doi.org/ 10.1186/s13063-015-0881-0 [ Links ]
20 Ólafsdóttir KB, Kristjánsdóttir H, Saavedra JM. Effects of exercise on depression and anxiety. A comparison to transdiagnostic cognitive behavioral therapy. Community Ment Health J. 2018 Aug 1;54(6):855-9. Acessível em: https://doi.org/ 10.1007/s10597-017-0213-9 [ Links ]
21 Helgadóttir B, Hallgren M, Ekblom Ö, Forsell Y. Training fast or slow? Exercise for depression: a randomized controlled trial. Prev Med. 2016 Oct 1; 91:123-31. Acessível em: https://doi.org/10.1016/j.ypmed.2016.08.011 [ Links ]
Received: March 07, 2019; Accepted: June 24, 2019
 Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
