










Servicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkRevista Portuguesa de Enfermagem de Reabilitação
versión impresa ISSN 2184-965Xversión On-line ISSN 2184-3023
RPER vol.2 no.1 Silvalde jun. 2019
https://doi.org/10.33194/rper.2019.v2.n1.03.4564
Articles
Physical Exercise in people with Diabetes: Systematic Review of Literature
1
 http://orcid.org/0000-0001-7427-0335
http://orcid.org/0000-0001-7427-0335
2
http://orcid.org/0000-0001-9764-5259
3
http://orcid.org/0000-0002-9702-3174
4
http://orcid.org/0000-0002-0004-8691
1- Unidade de Cuidados Continuados na ASFE Saúde, Portugal
2- Centro hospitalar Lisboa Ocidental, Hospital Egas Moniz, Portugal
3- Centro Hospitalar Lisboa Norte, Hospital Santa Maria, Lisboa, Portugal
4- . Escola Superior de saúde Atlântica, Barcarena, Portugal
5- Universidade de Évora, Escola Superior de Enfermagem S. João de Deus, Évora, Portugal
Background:
Diabetes mellitus is characterized as group of metabolic alterations manifested by chronic hyperglycemia. Physical exercise has been shown as a positive strategy in the diabetes therapeutic process.
Methods:
Systematic Review of Literature through the PICO method with the following research question: What are the benefits of physical exercise in a diabetic person? The research was carried out by using the electronic database platforms: EBSCOhost, Medline and BVS. The methodological quality was identified, selected, evaluated and we included the scientific papers that were according to PRISMA recommendations.
Results:
9 studies were included; they fulfilled the eligibility and methodological quality criteria.
Conclusion:
The physical exercise prescription in people with diabetes can be an adjuvant in the treatment of this condition with metabolic control benefits, and improve quality of life.
Keywords: Diabetes; Physical Exercise; Glycemia; Rehabilitation Nursing
Introdução:
A Diabetes mellitus é caraterizada como um conjunto de alterações metabólicas, manifestada por hiperglicemia crónica. A atividade física surge neste contexto como uma estratégia positiva no processo terapêutico da diabetes.
Método:
Revisão Sistemática da Literatura através do método PICO com a seguinte questão de pesquisa: Quais os benefícios do exercício físico na pessoa com diabetes? A pesquisa foi realizada com recurso a plataformas de bases de dados eletrónicas EBSCOhost, Medline e BVS tendo identificado, selecionado e avaliado a qualidade metodológica, incluindo artigos em acordo com as recomendações do PRISMA.
Resultados:
Foram incluídos 9 estudos que cumpriam os critérios de elegibilidade e qualidade metodológica definidos para esta revisão. O exercício físico traz benefícios para a pessoa com diabetes nomeadamente a nível da redução da glicose plasmática em jejum e dos valores da hemoglobina glicada, assim como, melhoria da qualidade de vida.
Conclusões:
A prescrição de exercícios físico em pessoas com diabetes pode ser um adjuvante no tratamento desta condição com benefícios no controlo metabólico e qualidade de vida.
Descritores: Diabetes; Exercício Físico; Glicémia; Enfermagem em Reabilitação
Introducción:
La diabetes mellitus es caracterizada como un conjunto de alteraciones metabólicas, manifestada por hiperglucemia crónica. La actividad física surge en este contexto como una estrategia positiva en el proceso terapéutico de la diabetes.
Método:
Revisión Sistemática de la Literatura. Se utilizó el método PICO con la siguiente pregunta de investigación: ¿Cuáles son los beneficios del ejercicio físico en la persona con diabetes? La pesquisa se realizó utilizando plataformas de bases de datos electrónicas EBSCOhost, Medline y BVS, identificando, seleccionando y evaluando la calidad metodológica, incluyendo artículos de acuerdo con las recomendaciones del PRISMA.
Resultados:
Se incluyeron 9 estudios que cumplían los criterios de elegibilidad y calidad metodológica definidos para esta revisión. El ejercicio físico trae beneficios para la persona con diabetes, especialmente en la reducción de la glucosa plasmática en ayuno y de los valores de la hemoglobina glucosa, así como la mejora de la calidad de vida.
Conclusiones:
La prescripción de ejercicios físicos en personas con diabetes puede ser un adyuvante en el tratamiento de esta condición con beneficios en el control metabólico y calidad de vida.
Descriptores: Diabetes; Ejercicio físico; Glucemia; Enfermería en Rehabilitación
INTRODUCTION
Diabetes mellitus is defined as a set of metabolic changes characterized by chronic hyperglycemia, which occur due to the destruction of beta cells in the pancreas, resistance to the action and/or insulin secretion disorders1.
Diabetes mellitus can be classified into the following categories: type 1 diabetes, type 2 diabetes, gestational diabetes mellitus and diabetes originating from other specific causes2-3. However, the study will focus on type 1 and type 2 diabetes mellitus.
Type 1 diabetes mellitus arises when beta cells are destroyed, leading to deficient production of insulin in the body. The cause for this type of diabetes is not known yet. The symptoms include: excessive thirst, frequent urination, hunger, weight loss, changes in vision and fatigue2-3.
Type 2 diabetes mellitus occurs due to an alteration in insulin secretion leading to body insulin resistance. This type of diabetes is one of the most frequent and the symptoms are very similar to type I diabetes mellitus, but generally less evident or even absent2-3.
Diabetes mellitus has become one of the most important public health challenges of the 21st century. Until the last decade, it was underestimated, and currently it is seen as a threat to global public health 4.
In 2014, worldwide, it was estimated that 422 million adults had diabetes, an increase compared to 1980, which had a prevalence of 108 million people. The overall (age-standardized) prevalence of diabetes has nearly doubled since 1980, rising from 4.7% to 8.5% in adults. This increase is associated with risk factors such as overweight or obesity3.
In Portugal, there is a statistically significant difference in the prevalence of Diabetes between men (15.9%) and women (10.9%), as well as the existence of a strong increase in the prevalence of diabetes with age (more than one quarter of people aged 60-79 years have diabetes) 5.
Among the various types of diabetes, type 2 diabetes mellitus is the most common, representing about 90-95% of cases6. Some risk factors for this type of diabetes are: genetics, ethnicity, age (non-modifiable factors), overweight or obesity, unhealthy diet, insufficient physical activity and smoking (factors modifiable through behavioral and environmental changes) 3.
Regular physical activity is important for everyone, but it is especially relevant for people with diabetes, being considered as an adjuvant in prevention and treatment7.
Physical activity includes all movements that result in energy expenditure above the resting level. Physical exercise, on the other hand, is a type of activity that consists of programmed, structured and systematically repetitive body movements that aim to improve physical preparation6.
Physical exercise, in addition to healthy eating habits, is one of the first strategies recommended for people newly diagnosed with type 2 diabetes mellitus, bringing benefits in terms of reducing the risk of diabetes and increasing blood glucose3 being essential for cardiovascular risk reduction, weight loss or control and general well-being. Physical exercise, whether aerobic, resistance or a combination, facilitates glucose regulation. High-intensity interval exercise is effective and has the advantage of being very efficient in terms of time7.
Regular physical exercise also brings considerable benefits to the health of people with type 1 diabetes mellitus, specifically, at the cardiovascular level, muscle strength and insulin sensitivity6.
Aerobic exercise is a type of exercise that involves continuous and rhythmic movements of large muscle groups, such as walking, running and cycling.8 This impacts on the increase in mitochondrial density, insulin sensitivity, oxidative enzymes, blood vessel reactivity, pulmonary function, immune function and cardiac output. In type 1 diabetes mellitus, aerobic exercise increases cardiorespiratory fitness, decreases insulin resistance and improves lipid levels and endothelial function6, while in people with type 2 diabetes mellitus, it improves blood glucose control, insulin sensitivity , oxidative capacity and important related metabolic parameters8.
Resistance exercise is synonymous of strength training and includes movements using free weights, weight machines, body weight exercises or elastic resistance bands8. At the level of type 1 diebetes mellitus, resistance exercise in the control of capillary blood glucose is not well defined, however it can help to minimize the risk of hypoglycemia induced by physical exercise6. In people with type 2 diabetes mellitus, resistance exercise brings gains, namely in terms of strength, bone mineral density, blood pressure, lipid profile, cardiovascular health, insulin sensitivity and muscle mass8.
In relation to mobility and balance exercises, these are more relevant in elderly people with diabetes. The limited joint mobility often observed in this population results in part from the formation of advanced glycosylation end-products, which accumulate during normal aging and are accelerated by hyperglycemia6.
Stretching exercises contribute to increased mobility, but do not affect glycemic control, while balance exercises can reduce the risk of falls6.
The specialist nurse in rehabilitation nursing has specialized knowledge and skills, intervening in an individual and unique way, taking into account the needs, characteristics, abilities and tolerance of each person9.
It is also responsible for monitoring and implementing rehabilitation programs, evaluating and making the necessary adjustments in the care delivery process. In this way, it makes it possible to improve the quality of life, through the improvement of functionality and autonomy, involving physical, social and emotional dimensions9. This systematic literature review is intended to identify: "What are the benefits of physical exercise for people with diabetes?". It was chosen because of its current prevalence, which gives it special importance in the area of expertise of the Specialist Nurse in Rehabilitation Nursing.
Thus, this systematic literature review (SLR) aims to assess the effects of physical exercise in people with diabetes.
MATERIAL AND METHODS
Nursing Research is a systematic, scientific and rigorous method that seeks to develop and deepen knowledge in this area, seeking to answer questions or solutions to problems for the benefit of the person, family and community10.
Scientific investigations in the field of nursing have been increasing, especially clinical research, with well-designed methods and a strong level of evidence, in order to support evidence-based practice (EBP)11.
SLR is a scientific methodology that makes it possible to identify, evaluate and abbreviate studies carried out by researchers, academics and health professionals. The starting point is a well-designed and formulated question using systematic and clear methods, also allowing for the collection and analysis of data from the studies that were included in the review12-13. For an analysis of all the available evidence, it is essential to follow the following steps: clearly define the objectives considering the eligibility criteria; explicit and reproducible methodology, systematic research that shows that all studies meet the eligibility criteria; evaluation of the authenticity of the results of the included studies12-13.
The research question of this study was conducted through the PICO method - Participant (Type of Participants); Intervention (Type of Intervention); Comparasion (comparison); Outcomes (Type of Results), as shown in table 1.
Table 1 PICO Method
| Participants (P) | People with diabetes |
| Intervention (I) | Physical activity |
| Comparison (C) | People with diabetes who do not exercise |
| Results (O) | Health benefits (e.g. well-being, quality of life…). |
Having said that, the following research question was defined for this Systematic Literature Review: “What are the benefits of Physical Exercise for People with Diabetes?”.
The research for the systematic review of the literature was defined as a function of the research question, the descriptors related to each of the components of the PICO strategy and keywords as shown in table 2. The descriptors were previously validated in the platform Descriptors in Health Sciences and Medical Subject Headings.
Table 2 PICO Method, Descriptors and Keywords
| Criteria | Starting Questions | Descriptors | Keywords |
|---|---|---|---|
| Participants (P) | People with Diabetes | Diabetes | |
| Intervention (I) | Physical exercise | Physical exercise Rehabilitation Nursing | Exercise Frequency, Intensity, Duration, Modality, Exercise Type |
| Comparison (C) | Diabetics who do not do physical exercise | ||
| Results (O) | Benefits to health | Glycemia quality of life |
The investigation took place in November 2018 through two independent surveys. Based on the aforementioned descriptors, the research was carried out in electronic database platforms: EBESCO host, Medline and Virtual Health Library.
Given the specificity of the topic and the large number of studies/articles found, it was necessary to define inclusion and exclusion criteria (Table 3) in order to help in the selection of studies/articles relevant to the development of the topic in question.
Table 3 Eligibility Criteria
| Elegibility criteria | Inclusion criteria | Exclusion criteria |
|---|---|---|
| Participants (P) | People with diabetes | People with other pathology |
| Intervention (I) | Physical exercise | |
| Study Design | Randomized Controlled Experimental Study | Systematic Literature Review, Other Quantitative Studies and Qualitative Studies |
| Time of publication | Article published between 2014 and 2018 | |
| Language | Article published in Portuguese, English and Spanish | |
| Article availability | Full article and open access | Incomplete article or incurring costs |
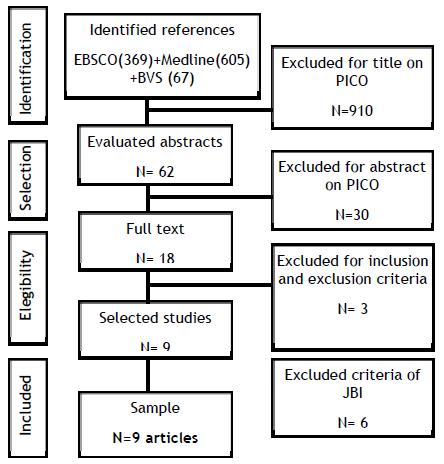
From the bibliographic research process carried out with this methodology, we obtained 1039 articles for the initial selection. Out of these, 910 were rejected by title or subject and 30 by abstract. Out of the resulting 18, 7 were excluded after analysis of the full text, as they did not meet the defined inclusion criteria, with the final result of 10 articles included that met the inclusion criteria.
Table 4 describes the process of combining descriptors and keywords for searching the databases. Figure 1 illustrates the PRISMA14 flowchart corresponding to the identification, analysis, selection and inclusion of articles.
Table 4 Boolean Conjugation
| Boolean Conjugation | Medline | BVS | EBSCOhost |
|---|---|---|---|
| ((exercise)OR(physical activity))AND(diabetes) | 605 | 67 | |
| ((Physical activity) OR (Exercise)) AND (Diabetes) | 369 | ||
| Total of articles | 1039 |
The articles selected for full reading were independently evaluated by two investigators, taking into consideration the methodological quality criteria proposed by the Joanna Brigggs Institute (JBI), Assessment and Review of Information15 and articles which met more than 75% of the criteria were selected.
The information was extracted from the articles on authors, year, country, sample, data on physical exercise (modality, frequency, intensity, volume and duration), conclusions and level of evidence. The levels of evidence of the included studies were classified according to the criteria of the Registered Nurses Association of Ontario, as shown below: Ib-Evidence determined from at least one randomized controlled study16-17.
RESULTS
In this SLR, 9 articles were published in the following years: 201420-21,23, 201519, 201624 and 201718,22,25-26. The sample of people with diabetes who underwent the intervention ranged between 1218 and 53626. The control group ranged between 518 and 14926. All studies included (Table 5) are experimental studies, with level of evidence Ib, that is, evidence obtained from a well-designed study and through at least one randomized controlled study15, which is therefore an added value for this SLR.
Table 5: Included articles
| Author, year, country | Participants | Objective | Intervention | Results | Level of evidence |
|---|---|---|---|---|---|
| Asuako,Benjamim; et al 18
2017 Gana |
12 people with diabetes treated at the KATH Diabetic Unit with a diagnosis of diabetes for less than fifty years, outpatient / age 20 to 68 years, sedentary and free from complications. 7 people in the intervention group (IG) 5 people in the control group (CG) |
To evaluate the effects of aerobic exercise on fasting plasma glucose and lipid profiles (FPG/LP) of people with diabetes | Eight weeks of aerobic training between August 2015 and March 2016 For 8 weeks: between August 2015 and March 2016 Modality: Walk without using a crosswalk Exercise Type: aerobic Exercise frequency: 3 times/week Intensity: moderate Exercise volume: Not defined Duration: 45 min Control Group: did not develop any physical activity |
- Weight loss of 4.85 kg (7.0%) - 4.08kg / m 2 (7.3%) reduction in BMI FPG reduced by 43.5% (5.28mmol / l) after eight weeks of training with aerobic exercises compared to the control group - Decrease of values in the profiles of LDL-C (0.33mmol / l, 11.9%), CT (0.47mmol / l, 5.3%) and T (0.48mmol / l, 29.4%) of IG patients and increased HDL-CC (0.16mmol / l, 7.1%) |
Level Ib Randomized and controlled study |
| Parra-Sánchez, J; et al 19
(2015) Spain. |
100 participants with type 2 diabetes Age between 65 and 80 years-old, sedentary 50% control group (IG) and 50% intervention group (CG). |
To analyze whether an exercise program can modify glycated hemoglobin (HbA1c), blood pressure (BP), body mass index (BMI), lipids, cardiovascular risk profile (CR), self-perceived health status (SHS) and pharmaceutical expenditure (PE). | For 3 months Primary Care: 2 rural health areas. Naval moral Health Area. Cáceres. Extremadura. Spain Modality: it was not defined Exercise type: controlled aerobic Exercise frequency: 2 times / week Intensity: it was not defined Exercise volume: it was not defined Duration: 50 min Control Group: they did not develop any physical activity |
Significant decrease in; HbA1c: 0.2 ± 0.4% (95% CI: 0.1 to 0.3); Systolic BP: 11.8 ± 8.5 mmHg (95% CI: 5.1 to 11.9), BMI: 0.5 ± 1 (95% CI: 0.2 to 0.8); Total cholesterol: 14 ± 28.2mg / dl (95% CI: 5.9 to 22.2); LDL: 18.3 ± 28.2mg / dl 95% CI: 10.2 to 26.3), RVC: 6.7 ± 7.7% (95% CI: 4.5 to 8.9), EP: 3.9 ± 10.2 € (95% CI: 0.9 to 6.8) and Increase in SHS: 4.7 ± 5.7 (95% CI: 3 to 6.3). |
Level Ib Randomized and controlled, blind study. |
| Dixit,Shenil ;et al20
2014 India |
87 People with type 2 diabetes with diabetic neuropathy 47 people in the control group with a mean age of 59.45 years 40 people in the intervention group with a mean age of 54.4 years |
To evaluate the effect of 8-week moderate-intensity aerobic exercise (40-60% of heart rate) on the quality of life of neuropathy in type 2 diabetes. | The study was conducted in a tertiary setting in Karnataka, India, from October 2009 to December 2010 For 8 weeks: between October 2009 and December 2012 Modality: treadmill Type of exercise: aerobic Intensity: moderate Exercise frequency: 5 to 6 days/week Volume: Not defined Duration: minimum 150 min/week and maximum 360 min/week Control Group: did not develop any physical activity |
When comparing the results of the control and the RANOV study group: No significant changes: - in the mean values of anthropometric measurements using RANOVA (p < 0.05) - (p < 0.05) in the mean values of glycemic control With significant changes:Significant difference: - (p < 0.05) in the mean values of MDNS -(p < 0.05) on quality of life measures -(p < 0.05) in the mean values of conduction velocity of the distal segment of the peroneal nerve (df = 1.62, F = 5.14 and p = 0.03) and of the sural sensory nerve (df = 1.60 , F = 10.16 and p \ 0.001) - for nerve conduction velocities in two groups, there was a significant difference between both groups (p < 0.05) |
Level Ib Randomized and controlled study |
| Taylor, J.; et al 2014 21 Arkansas |
21 people with type 2 diabetes aged between 18 and 69 years 10 people in the moderate intensity exercise training group (MOD group) 11 people in the high intensity exercise training group (HIGH group). |
To investigate the effects of moderate versus high-intensity exercise on fitness and physical condition in people with type 2 diabetes. | From September 2011 to August 2012. MOD Group: aerobic training Modality: treadmill Type of exercise: aerobic Intensity: 30% to 45% FC reserve Exercise frequency: 3 times/week Volume: Not defined Duration: 20min Endurance training Modality: resistance machines and weights Exercise type: resistance Intensity: 75% of 8-RM Exercise frequency: 2 times/week Volume: 4 sets of 8 reps Duration: Not defined HIGH group aerobic training Modality: treadmill Type of exercise: aerobic Intensity: 50% to 65% FC reserve Exercise frequency: 3 times/week Volume: Not defined Duration: 20 min Endurance training Modality: resistance machines and weights Exercise type: resistance Intensity: 100% of 8-RM Exercise frequency: 2 times/week Volume: 4 sets of 8 reps Duration: - Not defined |
Mean glucose levels before after exercise and after 1 hour after exercise MOD group 204.5 mg / dL (SD 92.3), 181.1 mg / dL (SD 84.2) and 172.0 mg / dL (SD 81.3 ) HIGH group 140.0 mg/d SD 34.4), 109.8 mg/dL (SD 17.9) and 118.5 mg/dL (SD 33.2). Little significant differences (but with improvements) between groups in relation to: exercise capacity, muscle strength and physical condition |
Level Ib Randomized and controlled study |
| Karimi, Hossein, et al 22
2017 Pakistan |
102 participants Experimental group (n = 51) with a mean age of 53.74 ± 8.75 years Control group (n = 51) with a mean age of 55.08 ± 7.67 years |
To determine the effects of a supervised structured aerobic exercise training program (SSAET) on interleukin-6 (IL-6), nitric oxide synthase 1 (NOS-1) and cyclooxygenase-2 (COX-2) in type 2 diabetes. | For 25 weeks From January 2015 to June 2016. SSAET combined with routine medication and diet plan was applied in the experimental group Control group treated with routine medication and diet plan Modality: treadmill Type of exercise: aerobic Intensity: Not defined Exercise frequency: Not defined Volume: Not defined Duration: 30 min in the first week increasing by 30 min each week for a total of 4 weeks |
The SSAET program, routine medication and eating plan improve IL-6 values in the experimental group, compared to a control group controlled by routine medication and eating plan, where deterioration in IL-6 was observed. . |
Level Ib Randomized and controlled study |
| Schreuder, TH; et al 23
2014 England and Netherlands |
15 males diagnosed with type 2 diabetes for at least 2 years -Exercise with double blocker (EX-ET) - Physical exercise with placebo (EX + placebo) |
To assess physical fitness in people with type 2 diabetes | For 8 weeks. All participants completed a questionnaire about their physician and medication use. All individuals underwent the same exercises: Modality: Bicycle and resistance machines Exercise type: aerobic and resistance exercise circuit Frequency: 3 times a week Intensity: moderate Volume: Not defined Duration: 60 minutes |
No effect of the 8-week intervention on glucose homeostasis was found. . |
Level Ib Randomized and controlled study |
| Leehey, DJ; et al 2016 24 USA |
36 male patients Age between 49-81 Groups: - Exercise + diet management (n = 18) - Diet alone (n = 18). |
To determine the effects of structured exercise physical fitness, kidney function, endothelial function, inflammation, and body composition in these patients. |
For 12 weeks Exercise + diet management group Modality: treadmill Exercise Type: Aerobic and Resistance Frequency: 3 times a week Intensity: Not defined Volume: Not defined Duration: Not defined Control group: diet only, no exercise |
No significant changes in: - urine albumin to creatinine ratio, - estimated glomerular filtration rate, - endothelial function, inflammation or body composition between groups. Controlled exercise improved exercise capacity in the obese diabetic person with CKD but not body composition or kidney function. |
Level Ib Randomized and controlled study |
| Otten,Julia; et al25
2017 Sweden |
32 people with type 2 diabetes (age 59 ± 8 years) followed a Paleolithic diet for 12 weeks. 2 groups: Paleolithic diet and standard care (SD) exercise recommendations Paleolithic diet with supervised exercise sessions of 1 h three times a week (PD-EX) |
To evaluate the effects of a Paleolithic diet with and without supervised exercise on fat mass, insulin sensitivity and glycemic control | Group (DP) Modality: brisk walking Exercise Type: aerobic Frequency: daily Intensity: moderate Volume: Not defined Duration: 30 minutes Group (PD-EX) Modality: brisk walking, sprints, leg press, seated leg extensions, leg curls, hip raises, flat and incline bench presses, seated rows, dumbbell rows, pull-downs lat shoulder raises, back extensions, burpees, sit- wall ups, step-ups and ball shots Exercise Type: aerobic and resistance Frequency: 3 times/week Intensity: moderate Volume: in resistance training 10 to 15 repetitions each exercise 2 to 4 sets Duration: 60min |
Diminuição: - Massa de gordura :5,7 kg (IQR: -6,6, -4,1; p <0,001); - da Leptina em 62% ( p<0,001); - Pressão Arterial - Triglicéridos - HbA 1C em 0,9% (-1,2, -0,6; p <0,001); Melhoria: - Sensibilidade à insulina e controle glicémico - Participantes sexo masculino diminuíram a massa magra em 2,6 kg |
Level IB Randomized and controlled study |
| Vlaar MA, et al 26 (2017) Netherlands |
536 South Asians aged 18 to 60 years at risk for diabetes Intervention group (n = 283): motivational interview, family session, cooking classes, supervised physical activity program Control group (n = 253) - received generic lifestyle advice |
To investigate the effectiveness of an intensive, culturally-oriented lifestyle intervention to prevent DM2 and cardiovascular risk factors among South Asian Surinamese in primary care. | From May 18, 2009 to October 11, 2010 Intervention Group: Modality: Any physical activity; Exercise Type: Undefined Intensity: Moderate to Intense Frequency: - Not defined Intensity: Not defined Volume: - Not defined Duration: Not defined Control Group: received current guidelines for diet and physical activity |
A culturally targeted lifestyle intervention in primary care did not change eating behavior and physical activity in a group of South Asian people at risk for type 2 diabetes | Level Ib Randomized and controlled study |
DISCUSSION
The modalities of physical exercise most applied in the selected studies were: walking18,20-21,23-24, resistance machines, free weight22,25 and bicycle24. The type of physical exercise recommended for the diabetic person will depend on some factors, namely their baseline physical condition, preferences, available means or the presence of physical limitations19.
The analyzed studies resorted essentially to aerobic exercises, with the exception of the studies of Karimi et al.,22 and Otten et al.,25 that combined aerobic and resistance exercises. Some studies reported that the combination of aerobic physical exercise in addition to resistance training may be better than any of them separately20.
The frequency of exercise evidenced in the studies ranged between twice a week19 and 5 to 6 times a week20 and lasted between 30 minutes22 and 60 minutes24-25 for each session of exercise. The minimum frequency of exercise recommended by the American Diabetes Association is 150 minutes per week of moderate aerobic exercise over at least three days a week; the Spanish Diabetes Society, on the other hand, recommends exercise sessions lasting at least 45 minutes, three times a week, divided into pre-warming, the main phase and finally relaxation20.
Exercise intensity was not evaluated equally in the articles analyzed and not all made reference to this parameter. Asuako et al.,18 assessed intensity using the maximum heart rate, a value obtained using a pulse oximeter version 803, China, placed during exercise and using the online Pace Calculator application.
In the studies carried out by Dixit et al.,20 and Taylor et al.,21, the exercise intensity was evaluated using the Karvonen formula (Training heart rate = Rest heart rate + (Intensity) x (Maximum heart rate - Heart rate) at rest). Dixit et al.,20 used a heart rate monitor (Polar Electro Oy, Kempele, Finland) and used it to monitor heart rate continuously during aerobic exercise.
It should be noted that in the analyzed studies, the characterization of the exercise was not always complete (modality, type of exercise, frequency, intensity, volume and duration) which limited the analysis, somehow limiting the generalization of the results.
In the analysis performed, only two articles combined the study of exercise with a specific type of diet25-26.
Otten et al.,25 combined physical exercise with a paleolithic diet, a diet based on the consumption of lean meat, fish, seafood, eggs, vegetables, fruits, berries and nuts and excluding cereals, dairy products, vegetables, refined fats, refined sugars and salt. In previous studies, the paleolithic diet had beneficial metabolic effects on obesity and the type of diabetes25.
Vlaar et al.,26 combined physical exercise with a healthy diet based on the national food guidelines for South Asia and which includes 2 pieces of fruit/day, vegetables (200g/day), whole wheat (whole wheat products exclusively), rice (only brown rice) and 3 meals a day/regular time.
By analyzing the articles, we found that there are important health gains for people with diabetes associated with the practice of physical exercise. The most used variables in most studies and which show these gains were glucose20, HbA1c19-25, body weight18-25 and cholesterol18-19, associated with more controlled glycated hemoglobin values and lower cardiovascular risk, also improving the psychosocial health status and decreasing pharmaceutical costs 19.
Practical implications
Physical exercise has a positive effect on the health of the diabetic person, however, the type of exercise, duration, frequency and intensity to use in reducing blood glucose should be clarified in future experimental studies.
Sedentary lifestyle and obesity in people with diabetes are factors that mark physical fitness. In this sense, nurses, doctors and other caregivers should promote greater encouragement and monitoring (intra- and extra-hospital) in order to improve these people's adherence to physical activity in general and to physical exercise in particular. It should be noted that physical activity is defined as any body movement produced by muscle contraction that results in energy expenditure above the resting level, and physical exercise is characterized by planned, organized and repeated body movements, with the objective of maintaining or improving one or more components of physical fitness27.
Rehabilitation Nursing can have a decisive role in increasing the practice of physical exercise in people with diabetes. And specialist nurses in rehabilitation nursing must participate in the production of evidence in this area, participate in decision-making related to health, as well as in the construction of health policies aimed at adopting healthy lifestyles related to the practice of physical exercise in people with diabetes.
Study limitations
The studies that integrated this SLR had some limitations, namely: the small sample size, limiting the generalization of the results, not all articles analyzed characterized physical exercise and those that did did not address all criteria, specifically, frequency, volume , duration and intensity. Regarding intensity, few studies have used scales to describe intensity as low, moderate or vigorous, which makes this assessment less objective. In addition, there is little scientific production on this topic, which was an obstacle to the realization of this RSL. Finally, it refers to the reduced number of databases accessed, as well as the language and time frame used, which can contribute to the reduced number of studies identified and included in the last step.
CONCLUSION
With this SLR and after analyzing the 9 studies, we can conclude that exercise brings benefits to people with diabetes, namely in terms of reducing fasting plasma glucose, glucose hemoglobin values, reducing body weight and cholesterol, as well as improving the person's quality of life.
This study allowed increasing knowledge in rehabilitation nursing, as well as contributing to the assessment of the benefits of structured physical exercise in people with diabetes. However, there were gaps in the description of exercises in terms of modality, frequency, intensity, volume, duration and progression. Further studies are recommended, with a more robust sample, where interventions within the scope of physical exercise are more objectively described, as well as the assessment instruments that allow not only to define exercise intensity, but also to demonstrate prescription-sensitive gains exercise performed by specialist nurses in rehabilitation nursing.
REFERÊNCIAS BIBLIOGRÁFICAS
1 Kerner W, Brückel J. Definition, Classification and Diagnosis of Diabetes Mellitus. Exp Clin Endocrinol Diabetes. 2014 Jul;122(07):384-6. Acessível em https://doi.org/10.1055/s-0034-1366278 [ Links ]
2 American Diabetes Association. 2. Classification and diagnosis of diabetes. Diabetes care. 2015 Jan 1;38(Supplement 1):S8-16. Acessível em https://doi.org/10.2337/dc15-S005 [ Links ]
3 World Health Organization. Global report on diabetes. Geneva: World Health Organization; 2016. Acessível em: http://apps.who.int/iris/bitstream/handle/10665/204871/9?sequence=1 [ Links ]
4 Zimmet P, Alberti KG, Magliano DJ, Bennett PH. Diabetes mellitus statistics on prevalence and mortality: facts and fallacies. Nat Rev Endocrinol. 2016 Oct;12(10):616-22. https://www.nature.com/articles/nrendo.2016.105 [ Links ]
5 Observatório Nacional da Diabetes. Diabetes Factos e Números o ano de 2015-Relatório Anual do Observatório Nacional da Diabetes. Sociedade Portuguesa de Diabetologia. 2016. [ Links ]
6 Colberg SR, Sigal RJ, Yardley JE, Riddell MC, Dunstan DW, Dempsey PC, Horton ES, Castorino K, Tate DF. Physical activity/exercise and diabetes: a position statement of the American Diabetes Association. Diabetes Care. 2016 Nov 1;39(11):2065-79. Acessível em https://doi.org/10.2337/dc16-1728 [ Links ]
7 Biazzon AC. Influência da atividade física no tratamento da diabetes mellitus tipo 1 e tipo 2. Rev Saúde Biol. 2018 Mar 14;12(2):68-73. http://revista2.grupointegrado.br/revista/index.php/sabios2/article/view/1744/983 [ Links ]
8 Kirwan JP, Sacks J, Nieuwoudt S. The essential role of exercise in the management of type 2 diabetes. Cleve Clin J Med. 2017 Jul;84(7 Suppl 1):S15. Acessível em https://dx.doi.org/10.3949%2Fccjm.84.s1.03 [ Links ]
9 Petronilho F, Machado M. Teorias de Enfermagem e Autocuidado: Contributos para a Construção do Cuidado de Reabilitação. in Marques-Vieira CM, Sousa LM (Eds). Cuidados de Enfermagem de Reabilitação à pessoa ao longo da vida. Loures: Lusoditacta; 2017:3-14. [ Links ]
10 Ordem dos Enfermeiros. Investigação em enfermagem: Tomada de posição. Lisboa: Ordem dos Enfermeiros; 2006. [ Links ]
11 Danski MT, de Oliveira GL, Pedrolo E, Lind J, Johann DA. Importância da prática baseada em evidências nos processos de trabalho do enfermeiro/Importance of evidence-based practice in nurse's work processes. Ciênc Cuid Saúde. 2017 Apr;16(2). DOI: 10.4025 [ Links ]
12 Sousa LMM, Firmino CF, Marques-Vieira CMA, Severino S, Pestana HCFC. Revisões da literatura científica: tipos, métodos e aplicações em enfermagem. Rev Port Enferm Reabil. 2018; 1(1): 46-55. [ Links ]
13 Galvão TF, Pereira MG. Systematic reviews of the literature: steps for preparation. Epidemiol Serv Saúde. 2014 Mar;23(1):183-4. Acessível em http://dx.doi.org/10.5123/S1679-49742014000100018 [ Links ]
14 Moher D, Shamseer L, Clarke M, Ghersi D, Liberati A, Petticrew M, Shekelle P, Stewart LA. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev. 2015 Dec;4(1):1. Acessivel em https://doi.org/10.1186/2046-4053-4-1 15. . Joanna Briggs Institute's. User Manual: Version 5.0 System for the Unified Management. Assessment and Review of Information. Joanna Briggs Institute's. 2011. Acessível em: http://joannabriggs. org/assets/docs/sumari/SUMARI-V5-User-guide [ Links ]
15 Joanna Briggs Institute's. User Manual: Version 5.0 System for the Unified Management. Assessment and Review of Information. Joanna Briggs Institute's. 2011. Acessível em: http://joannabriggs. org/assets/docs/sumari/SUMARI-V5-User-guide [ Links ]
16 Sousa LM, Marques-Vieira CM, Severino SS, Antunes AV. Metodologia de Revisão Integrativa da Literatura em Enfermagem. Rev Inv Enferm. 2017; S2(21):17-26 Disponível em: http://hdl.handle.net/20.500.12253/1311 [ Links ]
17 Registered Nurses Association of Ontario (RNAO). Falls Prevention: Building the Foundations for Patient Safety. A Self Learning Package. Toronto: Registered Nurses Association of Ontario; 2007. [ Links ]
18 Asuako B, Moses MO, Eghan BA, Sarpong PA. Fasting plasma glucose and lipid profiles of diabetic patients improve with aerobic exercise training. Ghana Med J. 2017;51(3):120-7. Acessível em http://dx.doi.org/10.4314/gmj.v51i3.5 [ Links ]
19 Parra-Sánchez J, Moreno-Jiménez M, Nicola CM, Nocua-Rodríguez II, Amegló-Parejo MR, del Carmen-Peña M, Cordero-Prieto C, Gajardo-Barrena MJ. Evaluación de un programa de ejercicio físico supervisado en pacientes sedentarios mayores de 65 años con diabetes mellitus tipo 2. Aten Primaria. 2015 Nov 1;47(9):555-62. Acessível em https://doi.org/10.1016/j.aprim.2015.01.006 [ Links ]
20 Dixit S, Maiya A, Shastry B. Effect of aerobic exercise on quality of life in population with diabetic peripheral neuropathy in type 2 diabetes: a single blind, randomized controlled trial. Res Qual Life. 2014 Jun 1;23(5):1629-40. Acessível em DOI 10.1007/s11136-013-0602-7 [ Links ]
21 Taylor JD, Fletcher JP, Mathis RA, Cade WT. Effects of moderate-versus high-intensity exercise training on physical fitness and physical function in people with type 2 diabetes: a randomized clinical trial. Phys Ther. 2014 Dec 1;94(12):1720-30. Acessivel em https://doi.org/10.2522/ptj.20140097 [ Links ]
22 Karimi H, Rehman SS, Gillani SA. Effects of Supervised Structured Aerobic Exercise Training Program on Interleukin-6, Nitric Oxide Synthase-1, and Cyclooxygenase-2 in Type 2 Diabetes Mellitus. J Coll Physicians Surg Pak. 2017 Jun 1;27(6):352-5. Acessível em: https://inis.iaea.org/search/search.aspx?orig_q=RN:48076473 [ Links ]
23 Schreuder TH, Duncker DJ, Hopman MT, Thijssen DH. Randomized controlled trial using bosentan to enhance the impact of exercise training in subjects with type 2 diabetes mellitus. Exp Physiol. 2014 Nov 1;99(11):1538-47. Acessível em https://doi.org/10.1113/expphysiol.2014.081182 [ Links ]
24 Leehey DJ, Collins E, Kramer HJ, Cooper C, Butler J, McBurney C, Jelinek C, Reda D, Edwards L, Garabedian A, O'Connell S. Structured exercise in obese diabetic patients with chronic kidney disease: a randomized controlled trial. Am J Nephrol. 2016;44(1):54-62. Acessível em https://doi.org/10.1159/000447703 [ Links ]
25 Otten J, Stomby A, Waling M, Isaksson A, Tellström A, Lundin-Olsson L, Brage S, Ryberg M, Svensson M, Olsson T. Benefits of a Paleolithic diet with and without supervised exercise on fat mass, insulin sensitivity, and glycemic control: a randomized controlled trial in individuals with type 2 diabetes. Diabetes Metab Res Rev. 2017 Jan;33(1):e2828. Acessível em https://doi.org/10.1002/dmrr.2828 [ Links ]
26 Vlaar EM, Nierkens V, Nicolaou M, Middelkoop BJ, Busschers WB, Stronks K, van Valkengoed IG. Effectiveness of a targeted lifestyle intervention in primary care on diet and physical activity among South Asians at risk for diabetes: 2-year results of a randomised controlled trial in the Netherlands. BMJ open. 2017 Jun 1;7(6):e012221. Acessível em https://doi:10.1136/ bmjopen-2016-012221 [ Links ]
27 Santa-Clara H, Pinto I, Santos V, Pinto R, Melo X, Almeida JP, Pimenta N, Abreu A, Mendes M. Atividade física e exercício físico: especificidades no doente cardíaco. Rev Factores de Risco. 2015, 35:28-35. Acessível em. http://hdl.handle.net/10400.17/2154 [ Links ]
Received: March 05, 2019; Accepted: June 27, 2019
 Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
