










Serviços Personalizados
Journal
Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkRevista Portuguesa de Enfermagem de Reabilitação
versão impressa ISSN 2184-965Xversão On-line ISSN 2184-3023
RPER vol.1 no.2 Silvalde dez. 2018
https://doi.org/10.33194/rper.2018.v1.n2.02.4421
Articles
Metric Properties Of The Oxford Knee Score In People With Osteoarthritis After Knee Arthroplasty: Systematic Review Of Literature
1- Centro Hospitalar Lisboa Norte, EPE - Polo Hospital Santa Maria | Empresa de Cuidados Domiciliários Integrados com Base nas Novas Tecnologias - “Satélite Familiar”
2- Hospital de Santa Maria, Centro Hospitalar Lisboa Norte, E.P.E
3- Centro Hospitalar da Universidade de Coimbra
5- Hospital Curry Cabral, Centro Hospitalar Universitário Lisboa Central
6- Escola Superior de saúde Atlântica
Objective:
To evaluate the metric properties of the Oxford Knee Score (OKS) applied in people with osteoarthritis after knee arthroplasty.
Method:
Systematic review of the literature. The EBSCOhost platform was used to access the MEDLINE and LILACS database and the SCiELO platform. The descriptors were validated on the DeCS and MESH platforms, except for "Oxford Knee Score" and "responsiveness". We selected articles published in the last five years, available in Portuguese, English and Spanish.
Results:
There were eight articles that revealed that OKS is a valid, reliable and reproducible instrument. Responsiveness was the least studied metric property.
Conclusion:
The Oxford Knee Scale is adequate to evaluate the functionality and the impact of pain in people with Osteoarthritis after knee arthroplasty.
Descriptors: Validation Studies; Test Reproducibility; Knee; Osteoarthritis; Reliability; Nursing Assessment
Objetivo:
Avaliar as propriedades métricas da Oxford Knee Score aplicada em pessoas com osteoartrite após artroplastia do joelho.
Método:
Revisão sistemática da literatura. Recorreu-se à plataforma EBSCOhost que permitiu aceder à base de dados MEDLINE e LILACS e plataforma SCiELO. Os descritores foram validados nas plataformas DeCS e MESH, à exceção de “Oxford Knee Score” e “responsividade”. Foram selecionados artigos publicados nos últimos cinco anos, disponíveis em português, inglês e espanhol.
Resultados:
Obtiveram-se oito artigos que revelaram que o Oxford Knee Score é um instrumento válido, fiável e reprodutivo. A responsividade foi a propriedade métrica menos estuda.
Conclusão:
O Oxford Knee Score é adequado para avaliar a funcionalidade e o impato da dor em pessoas com Osteoartrite após atroplastia do joelho.
Descritores: Estudos de Validação; Reprodutibilidade dos Testes; Joelho; Osteoartrite; Avaliação em Enfermagem
Objetivo:
Evaluar las propiedades métricas de la Oxford Knee Score aplicada en personas con osteoartritis después de la artroplastia de la rodilla.
Método:
Revisión sistemática de la literatura. Se recurrió a la plataforma EBSCOhost que permitió acceder a la base de datos MEDLINE y LILACS y plataforma SCiELO. Los descriptores fueron validados en las plataformas DeCS y MESH, con excepción de "Oxford Knee Score" y "responsividad". Se seleccionaron los artículos publicados en los últimos cinco años, disponibles en Portugués, Inglés y Español.
Resultados:
Se han obtenido ocho artículos que revelaron que Oxford Knee Score es un instrumento válido, fiable y reproductivo. La responsividad fue la propiedad métrica menos estudiada.
Conclusión:
El Oxford Knee Score es adecuado para evaluar la funcionalidad y el impacto del dolor en personas con Osteoartritis después de la artroplastia de la rodilla.
Descriptores: Estudios de Validación; Reproducibilidad de los Resultados; Rodilla; Osteoartritis; Evaluación en Enfermería
INTRODUCTION
Nursing, like all sciences, has been going through political, social and economic transformations over time, in order to fit in with the development and globalization process of our decade. As such, there is a need to implement a practice based on scientific evidence, combining training with the profession, supporting health gains that come from nursing practice.1
In Rehabilitation Nursing, it is essential to use assessment tools to identify changes in activities of daily living, cognitive, sensory and motor, cardiorespiratory, nutrition, elimination and sexuality. The use of these instruments also allows nurses to monitor the progress of their intervention, documenting the effectiveness and benefit of the rehabilitation plan.2
The Oxford Knee Score (OKS) is an instrument consisting of a twelve-question questionnaire and has a two-dimensional characteristic, as it assesses the component of pain and functionality.3 This scale was developed and validated by researchers at the University of Oxford to function as an instrument to measure outcomes after knee arthroplasty in people with osteoarthritis (OA).4 The OKS is a commonly used instrument to assess symptoms and functional status in persons with knee OA.5
The use of OKS has been increasing, as is the need to be validated in different countries, given the increase in persons with knee OA. Statistical data demonstrates substantial growth in persons with OA.
In Portugal, rheumatic diseases have an approximate prevalence of 20 to 30%, and are the main cause of disability among elderly with impairment of joints that are important for functionality, such as the hand, knee, hip, spine and foot. Arthroplasty has improved the prognosis of the person with OA.6 This information is comparable to a study carried out in England, which states that the population of the United Kingdom is growing in number and age, and that OA Knee is more common in older people. The number of persons with knee OA is estimated to increase to 5.4 million in 2020 and 6.4 million in 2035.7
The aim of this systematic literature review (SLR) was to assess the metric properties of OKS, in order to verify if it is valid, reliable, reproductive and responsive when used in persons with OA.
MATERIALS AND METHODS
An SLR was chosen, as it uses a systematic, explicit and reproducible method based on a clearly formulated question, which allows the identification, evaluation and synthesis of primary studies.8,9
The research question was formulated from the PICo strategy,10 considering the recommendations of the Joanna Briggs Institute (JBI),11 where each dimension of the PICo10 contributed to define the inclusion criteria: Population (P) - People with osteoarthritis of the knee; Area of Interest (I) - metric properties of the Oxford Knee Score scale and Context (Co) - knee arthroplasty. Thus, the following research question was defined for this SLR: “What are the metric properties of the Oxford Knee Score scale in persons with OA of the knee?”.
The investigation took place during the month of October 2014, and two independent researches were carried out on database platforms: EBSCOhost which allowed access to the MEDLINE and LILACS databases; to the SCiELO platform. The descriptors were previously validated on the DeCS and MESH platforms:
Measurement/Psycometrics properties;
Validation/Validation;
Validity of results/Validity of results;
Reproducibility of tests/Reproducibility of tests;
Reliability/Reliability;
Knee/Knee, Osteoarthritis/Osteoarthritis.
However, the following keywords were used: Oxford Knee Score and Responsividade/Responsiveness, which are not validated as descriptors in both platforms, but which play a fundamental role in making the research as concise as possible.
The inclusion and exclusion criteria that allowed the selection of articles are described in table 1.
Table 1 Inclusion and Exclusion Criteria
| Selection criteria | Inclusion criteria | Exclusion criteria |
|---|---|---|
| Participants | Person with knee osteoarthritis | Person with other knee pathology and children |
| Area of interest | Validity, reliability, reproducibility and responsiveness | Do not mention at least one of these criteria |
| Study design | Quantitative study | Qualitative study, reviews, opinion articles |
| Publication period | Article published between 2009 and 2014 | |
| Language in which it is published | Article published in English, Portuguese and Spanish | |
| Document availability | Full article and free access | Incomplete article or payment is required |
The search was carried out using the Boolean combination of descriptors, identified in Table 2. The search was carried out by two reviewers independently, to ensure the rigor of the method and the reliability of the results. The articles to be included in the sample were selected in the following sequence: title reading, abstract reading and full text reading, following the PRISMA recommendations (Figure 1).
Table 2 Boolean conjugation
| Boolean Conjugation | Search results |
|---|---|
| Oxford Knee Score AND knee osteoarthritis | 34 |
| Oxford Knee Score AND assessment | 168 |
| Oxford Knee Score AND psychometrics | 16 |
| Oxford Knee Score AND validity | 23 |
| Oxford Knee Score AND reliability | 15 |
| Oxford Knee Score AND reproducibility | 19 |
| Knee AND pain AND physical function | 1323 |
| Oxford Knee Score AND validation AND cultural | 9 |
| Oxford Knee Score AND responsiveness | 4 |
| TOTAL | 1611 |
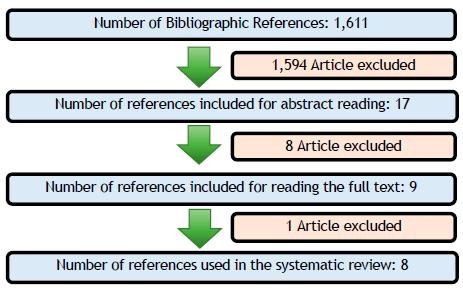
The eight articles presented ≥ 75% of the JBI evaluation criteria; therefore, they were considered of methodological quality and included in the SLR sample.
The study of metric properties was carried out based on the criteria of Validity, Reproducibility and Responsiveness.12-13
RESULTS
After reading nine articles in full, one was eliminated and eight were used for this SLR. We surveyed information about the year, country, author, participants, interventions, results and the level of evidence (Table 3). All articles presented evidence level III, that is, evidence from well-designed experiments, such as non-randomized studies, cohort studies, time series or combined case-control studies.14
The eight articles analyzed come from several countries, namely, China,22 Korea,15 France,18-19 England,17 Japan,21 Portugal16 and Switzerland.20 Were published between 2009 and 2013. All present evidence level III 14. Samples ranged from 5121 to 18722 participants with knee OA. These studies verified the reproducibility, reliability and validity, however, three17,19,21 demonstrated responsiveness.
DISCUSSION
With regard to reproducibility, Naal et al.20 studied reliability through internal consistency (Cronbach's α of 0.83) and an intraclass correlation coefficient (ICC) of 0.91. Jenny and Diesinger18 verified the intra-observer reliability through the Cronbach's α value, which was 0.88, similar to the original scale,4 whose value was 0.87. Furthermore, the values of the inter-observer reliability were also similar.
In the study by Xie et al.22, reliability has a Cronbach's α value of 0.896. Reliability in the study by Takeuchi et al.21 was demonstrated through test-retest, with an ICC of 0.85, and internal consistency was assessed by Cronbach's α with a value of 0.90. The study by Jenny and Diesinger19, in evaluating internal reliability, revealed a Cronbach's α of 0.88 before surgery and 0.66 after surgery, and no significant associations for this phenomenon were demonstrated.
In the Portuguese version16, for internal consistency, Cronbach's α of 0.87. The reproducibility, measured by the CCI, was 0.97 and that proves to be adequate.
Harris et al.,17 verified the internal consistency, with Cronbach's α of 0.94 for OKS, 0.88 for the OKS-physical component (OKS-FCS) and 0.90 for the OKS-pain component (OKS-PCS). The test-retest revealed a CCI for the OKS of 0.93, for the OKS-PCS of 0.91 and for the OKS-FCS of 0.93. In the study by Eun et al.,15 the internal reliability was demonstrated with Cronbach's α of 0.932 and the inter-observer reliability by Cohen's kappa between 0.61-0.87. Through the test-retest, the CCI of 0.848 was obtained, demonstrating the reproducibility of the questionnaire.
In all the versions studied, the scale proved to be reliable, being superior to 0.70,12-13 except in the study by Jenny and Diesinger 19, in the evaluation after surgery.
In the validation and adaptation of the OKS to the German version, carried out by Naal et al.,20 the construct validity was assessed by comparing OKS and the Western Ontario and McMaster Universities Index (WOMAC), Knee Society Score (KSS) scales, Activities of Daily Living Scale (ADLS), Short Form - 12 (SF-12). A higher correlation was found between the German OKS and ADLS (ρ<0.001), this may be related to the specific characteristics of the knee assessed by the scale, while WOMAC focuses on the specificities of the disease. The lowest coefficient of relationship found was with the SF-12 (ρ= 0.02).
Table 3 Studies description
| Author, year, country | Participants | Objective | Results | EL |
|---|---|---|---|---|
| Eun IS, Kim OG, Kim CK, Lee HS, Lee JS. 2013, Korea15 | 142 participants subjected to knee arthroplasty | To validate the Korean version of OKS in people undergoing arthroplasty | In this study, reliability, validity and reproducibility were confirmed. Comparison with Visual Analog Scale and Short Form - 36. Responsiveness was not determined due to the short time in which the test-retest was performed. | III |
| Gonçalves RS, Tomás AM, Martins DI. 2012, Portugal16 | 80 participants who underwent knee arthroplasty for OA and who were undergoing treatment | To adapt OKS to the Portuguese version and validate its metric properties | The adaptation of OKS to the Portuguese language demonstrated reliability, reproducibility and validity. Comparison with Visual Analog Scale and Short Form - 36: Responsiveness was not assessed due to the impossibility of performing a sufficient number of retests. | III |
| Harris KK, Dawson J, Jones LD, Beard DJ, Price AJ. 2013, England17 | 134 participants with knee OA subjected to non-surgical treatment | To assess the validity of OKS when applied to people with knee OA undergoing non-surgical treatment | Comparison with Intermittent and Constant Osteoarthritis Pain, Knee Injury and Ostheoarthritis Outcome Score-Physical, Short Form -12 . OKS has proven to be a reliable, valid and responsive tool in people with OA without surgical indication. | III |
| Jenny JY, Diesinger Y., 2011, France18 | 100 participants with OA awaiting knee arthroplasty | To validate OKS for French version | OKS in the French version proves to be a valid and reliable tool, according to the authors, safer when used on a person awaiting surgery. Comparison with International Knee Society Score. Reproducibility was not ascertained, as was responsiveness. | III |
| Jenny JY, Diesinger Y., 2012, France19 | 100 participants with OA awaiting surgery and 100 undergoing knee arthroplasty surgery | To compare the validity of OKS applying it before and after knee arthroplasty | Comparison with American Knee Score. The scale is valid and responsive, however it offers safer results when applied to people awaiting surgery | III |
| Naal FD, Impellizzeri FM, Sieverding M, Loibl M, Von Knoch F, Mannion AF, Leunig M, Munzinger U., 2009, Switzerland 20 | 100 participants undergoing knee arthroplasty surgery for the first time | To validate OKS for German language and evaluation of its metric properties when applied to people with OA of the knee. | Comparison with Western Ontario and McMaster Universities Index, Knee Society Score, Activities of Daily Living Scale and Short Form-12. OKS validation for the German language is a valid and reliable tool for self-assessment of pain and physical function. | III |
| Takeuchi R, Sawaguchi T, Nakamura N, Ishikawa H, Saito T, Goldhahn S., 2011, Japan21 | 51 participants with knee pathology, without arthroplasty | To validate OKS for Japanese language and evaluate its metric properties | Comparison with Western Ontario and McMaster Universities Index and Short Form - 36. The OKS validated for the Japanese language proves to be a reliable, valid and reproducible tool. However, due to a low floor effect (9%) it was not possible to determine the responsiveness. | III |
| Xie F, Ye H, Zhang Y, Liu X, Lei T, LI SC.., 2011, China22 | 187 participants with OA | To assess the OKS for its validity and reliability in measuring health outcomes in people with OA | Comparison with Short-Form - 6D, EuroQoL Group 5-Dimension Self-Report Questionnaire score and Visual Analog Scale. Validity and reliability have been proven, however responsiveness has not been ascertained. | III |
In the study by Jenny and Diesinger,18 it was found that there is concurrent validity between the OKS and KSS questionnaire, and the correlation is negative, as the results of both scales are inverse.
Construct validity in the study by Xie et al. 22 was assessed using Spearman's correlation coefficient (ρ) and compared with the Short Form (SF) - 6D scale, with the EuroQol Group 5- Dimension Self-Report Questionnaire (EQ-5D) and Visual Analog Scale (VAS), with moderate to strong correlation between them. The correlation between the OKS and the mental health domain, assessed by the SF-6D, and the anxiety/depression domain assessed by the EQ-5D, was strong, contrary to what would be expected, compared to results from previous studies, such as Dunbar and collaborators23 in the validation of OKS for the Swedish version. This might mean that OA affects person's quality of life, not only physically but also psychologically.
In Takeuchi et al.,21 validity was demonstrated by construct validity through Spearman's correlation coefficient (ρ), comparing OKS with WOMAC (pain, stiffness and physical function) and SF-36 (physical function, physical state, physical pain, general health status, vitality, social function, emotional status and mental health). This showed convergent validity with WOMAC and SF-36 (function, physical state and pain) and divergent validity between OKS and SF-36 (general health, vitality, emotional aspect and mental health).
To assess validity, Jenny and Diesinger,19 used the Spearman correlation coefficient (ρ) between OKS and the American Knee Score (AKS); the result was negative either before or after surgery. It should be noted that the OKS results are inverse to those of the AKS, that is, lower results on the OKS indicate good knee condition and the opposite is true for the AKS. Thus, it is concluded that a negative correlation indicates a good clinical correlation in terms of construct validity, with a value of ρ <0.05 in most correlations.
In validating the OKS for the Portuguese version,16 the construct validity of the OKS was measured using the Spearman correlation coefficient (ρ), in which the OKS was correlated with SF-36 and VAS, verifying that the three measures assess similar constructs. Since OKS varies from best to worst state, SF-36 varies from worst to best state, and in turn VAS varies from best to worst state, it was expected that OKS would relate negatively to SF-36 and positively to VAS. This correlation was confirmed by a value of ρ=0.05. OKS was negatively related to SF-36 for values between -0.28 and -0.77; in turn, OKS was positively related to VAS for values between 0.39 and 0.44. The negative relationship of OKS with SF-36 is a good correlation, and the inverse of passes with the correlation between OKS and VAS.
For Harris et al.,17 the OKS and subscales, the OKS-PCS (pain) and OKS-FCS (physical function), are likely to be applied in people with knee OA without surgical indication, as a way to monitor the evolution (improvement or deterioration) of pain and physical function. In this sense, to demonstrate the construct validity, the OKS was compared with the Knee injury and Osteoarthritis Outcome Score-Physical (KOOS-PS), Intermittent and Constant Osteoarthritis Pain (ICOAP) and SF-12, using Spearman's correlation coefficient. This comparison revealed a strong correlation between OKS, KOOS-PS and ICOAP, being higher than predicted compared to SF-12 PCS in the pain domain and, as expected, a weak correlation with SF-12 MCS (mental component). It was also shown that OKS-PCS is more correlated with ICOAP than with KOOS-PS and that OKS-FCS is more correlated with KOOS-PS than with ICOAP, providing evidence for convergent and divergent validity. In the study by Eun et al.,(15) the validity of OKS was obtained through the concurrent validity of r=0.692 and ρ<0.001 between OKS and VAS, and the construct validity between OKS and SF-36 (r=-0.74), this being considered convergent, in the domains of physical function and pain, and divergent in the other domains.
The validity of the OKS in all studies was verified by the correlation with scales that assess the same construct, that is, through the concurrent/divergent validity,12-13 with moderate to strong and significant correlations with the scales used in the comparisons. . That is how the validity of the OKS was verified in people with OA in the postoperative period of knee arthroplasty.
Regarding responsiveness, Takeuchi et al.,21 verified the floor effect and ceiling effect, which correspond, respectively, to the worst score and the best score.12-13 In the questionnaires evaluated, the sample corresponding to the floor effect was very low (9%), and it is not possible to determine the responsiveness.
In the study by Jenny and Diesinger,19 responsiveness was assessed through the applicability of OKS before and after knee arthroplasty, and it was concluded that the group of people awaiting surgery had a null floor effect and a low ceiling effect. Inversely, in the group of people undergoing surgery, it was found that the floor effect was substantial and that the ceiling effect was null. The ceiling effect suggests that people awaiting surgery suffer from severe pain and functional disability; after surgery, the strongly present floor effect suggests that there is an improvement in physical and functional well-being, but it does not allow us to understand differences in results between two different people.
In Harris et al.,17 these scales were applied on the first day and three months later, and OKS revealed that 15% of people showed deterioration in their health status, 30% showed improvement in their health status and 55% did not reflect any change, thus confirming its responsiveness.
OKS is reliable, reproducible and valid.15-22 These results are similar to versions validated for other languages, such as Chinese, 24 Dutch, 25 Italian,26 Swedish23 and Thai.27
The OKS allows self-assessment of pain and physical function in people with knee OA20, however, it offers safer results when applied to people who have not yet undergone surgery.19
In this review, it is verified that the Portuguese version of the OKS is a reliable, reproductive and valid instrument to be used in the Portuguese population.16
Regarding responsiveness, it was only demonstrated in two studies.17,19
Practical implications for future investigations
The study of the metric properties of OKS reveals that it is effectively a reliable instrument, valid in several languages, including European Portuguese, when used before any procedure, whether surgical or non-surgical. However, it is suggested that the verification of OKS responsiveness be considered in future studies.
The use of a valid, reliable, reproducible and responsive scale in clinical practice allows us to guarantee the objectivity and accuracy of the results obtained, helping the rehabilitation nurse to make more appropriate clinical judgments and verify the gains obtained with their intervention.
This scale can be used before surgery and four weeks after surgery, as this is the period that is included in the scale, that is, it addresses how the person feels in the last four weeks, regarding pain and the performance of activities of daily living. (3.28)
CONCLUSION
After analyzing and interpreting the articles included, the results found allow us to answer the defined research question. However, it is not possible to compare all the included studies, as they are not homogeneous in the sample, in the various concepts they assessed, as well as in the different strategies used.
Despite the geographic, cultural and socioeconomic differences, where the different studies were carried out, it should be noted that it was possible to assess the metric properties of the OKS when applied to persons with OA.
The assessment of internal consistency was demonstrated using Cronbach's α, which was found to be greater than 0.70 in all selected studies, thus demonstrating the reliability of the scale, except in one study carried out postoperatively. Validity was demonstrated by construct validity, using Spearman's correlation coefficient (ρ), when comparing the OKS with other scales selected for each study. Reproducibility was also only confirmed in a few studies using the CCI, obtained through test-retest. Responsiveness was not ensured in all analyzed studies, as not all of them had established a floor effect and/or ceiling effect, or a sufficient period of time to assess change in health status.
REFERÊNCIAS
1 Gomes JAP, Martins MM, Gonçalves MN. Qualidade e Enfermagem de reabilitação em unidade de internamento. In B Gomes, MC Rocha, MM Martins, MN Gonçalves (Orgs.). Investigação em Enfermagem de Reabilitação: um novo conhecimento para guiar a prática de cuidados. Porto: ESEP-Enfermagem Porto; 2014 Feb 28. [ Links ]
2 Ordem dos Enfermeiros. Regulamento das Competências Especificas do Enfermeiro Especialista em Enfermagem de Reabilitação. Lisboa. Ordem dos Enfermeiros. 2010. [ Links ]
3 Williams DP, Blakey CM, Hadfield SG, Murray DW, Price AJ, Field RE. Long-term trends in the Oxford knee score following total knee replacement. Bone Joint J. 2013 Jan;95(1):45-51. [ Links ]
4 Dawson J, Fitzpatrick R, Murray D, Carr A. Questionnaire on the perceptions of patients about total knee replacement. Bone Joint Surg. British volume. 1998 Jan;80(1):63-9. [ Links ]
5 Cheung RT, Ngai SP, Ho KK. Chinese translation and validation of the Oxford Knee Scale for patients with knee osteoarthritis. Hong Kong Physiother J. 2017 Dec 1;37:46-9. [ Links ]
6 Lucas R, Monjardino M. O estado da Reumatologia em Portugal. Porto: Observatório Nacional das Doenças Reumáticas. 2010 Apr. [ Links ]
7 Arthritis Research UK. Osteoarthritis in General Practice: Data and Perspectives. Arthritis Research UK; 2013. [ Links ]
8 Fink A. Conducting research literature reviews: from the Internet to paper.4th Edition. Los Angeles: Sage Publications; 2014. [ Links ]
9 Sousa LMM, Firmino CF Marques-Vieira CMA, Severino S, Pestana HCFC. Revisões da literatura científica: tipos, métodos e aplicações em enfermagem. Rev Port Enferm Reabil.2018; 0:46-55. Disponível em: http://www.aper.pt/ficheiros/revista/rpernv1n1.pdf [ Links ]
10 Sousa LM, Marques JM, Firmino CF, Frade F, Valentim OS, Antunes AV. Modelos de formulação da questão de investigação na prática baseada na evidência. Rev Invest Enferm.2018; S2(23):31-39. [ Links ]
11 Joanna Briggs Institute (2011). Joanna Briggs Institue's user manual: version5.0 system for the unified management. Assessment and Review of Information. Adelaide: The Joanna Briggs Institute. 2011. Available in http://www.joannabriggs.org/assets/docs/sumari/SUMARI-V5-User-guide.pdf [ Links ]
12 Sousa LM. As propriedades psicométricas dos instrumentos de hétero-avaliação. Enformação. 2015;6:20-4. Disponível em http://hdl.handle.net/10884/998 [ Links ]
13 Sousa LM, Marques-Vieira C, Severino S, Caldeira S. Propriedades psicométricas de instrumentos de avaliação para a investigação e prática dos enfermeiros de reabilitação. In C. Marques-Vieira, L. Sousa (Eds). Cuidados de Enfermagem de Reabilitação à Pessoa ao Longo da Vida. Loures: Lusodidacta. 2017:113-122. [ Links ]
14 Pereira ÂL, Bachion MM. Atualidades em revisão sistemática de literatura, critérios de força e grau de recomendação de evidência. Rev Gaúcha Enferm. 2006 Dec 31;27(4):491-498. [ Links ]
15 Eun IS, Kim OG, Kim CK, Lee HS, Lee JS. Validation of the Korean version of the Oxford Knee Score in patients undergoing total knee arthroplasty. Clin Orthop Relat Res. 2013 Feb 1;471(2):600-5. [ Links ]
16 Gonçalves RS, Tomás AM, Martins DI. Cross-cultural adaptation and validation of the Portuguese version of the Oxford Knee Score (OKS). Knee. 2012 Aug 1;19(4):344-7. [ Links ]
17 Harris KK, Dawson J, Jones LD, Beard DJ, Price AJ. Extending the use of PROMs in the NHS-using the Oxford Knee Score in patients undergoing non-operative management for knee osteoarthritis: a validation study. BMJ open. 2013 Aug 1;3(8):e003365. [ Links ]
18 Jenny JY, Diesinger Y. Validation of a French version of the Oxford knee questionnaire. Orthop Traumatol Surg Res. 2011 May 1;97(3):267-71. [ Links ]
19 Jenny JY, Diesinger Y. The Oxford Knee Score: compared performance before and after knee replacement. Orthop Traumatol Surg Res. 2012 Jun 1;98(4):409-12. [ Links ]
20 Naal FD, Impellizzeri FM, Sieverding M, Loibl M, Von Knoch F, Mannion AF, Leunig M, Munzinger U. The 12-item Oxford Knee Score: cross-cultural adaptation into German and assessment of its psychometric properties in patients with osteoarthritis of the knee. Osteoarthr Cartil. 2009 Jan 1;17(1):49-52. [ Links ]
21 Takeuchi R, Sawaguchi T, Nakamura N, Ishikawa H, Saito T, Goldhahn S. Cross-cultural adaptation and validation of the Oxford 12-item knee score in Japanese. Arch Orthop Trauma Surg. 2011 Feb 1;131(2):247-54. [ Links ]
22 Xie F, Ye H, Zhang Y, Liu X, Lei T, LI SC. Extension from inpatients to outpatients: validity and reliability of the Oxford Knee Score in measuring health outcomes in patients with knee osteoarthritis. Int J Rheum Dis. 2011 May;14(2):206-10. [ Links ]
23 Dunbar MJ, Robertsson O, Ryd L, Lidgren L. Translation and validation of the Oxford-12 item knee score for use in Sweden. Acta Orthop Scand. 2000 Jan 1;71(3):268-74. [ Links ]
24 Xie F, Li SC, Lo NN, Yeo SJ, Yang KY, Yeo W, Chong HC, Fong KY, Thumboo J. Cross-cultural adaptation and validation of Singapore English and Chinese Versions of the Oxford Knee Score (OKS) in knee osteoarthritis patients undergoing total knee replacement. Osteoarthr Cartil. 2007 Sep 1;15(9):1019-24. [ Links ]
25 Haverkamp D, Breugem SJ, Sierevelt IN, Blankevoort L, Dijk CN. Translation and validation of the Dutch version of the Oxford 12-item knee questionnaire for knee arthroplasty. Acta Orthop. 2005 Jan 1;76(3):347-52. [ Links ]
26 Padua R, Zanoli G, Ceccarelli E, Romanini E, Bondi R, Campi A. The Italian version of the Oxford 12-item Knee Questionnaire-cross-cultural adaptation and validation. Int Orthop. 2003 Aug 1;27(4):214-6. [ Links ]
27 Charoencholvanich K, Pongcharoen B. Oxford knee score and SF-36: translation & reliability for use with total knee arthroscopy patients in Thailand. J Med Assoc Thai. 2005 Sep 1;88(9):1194. [ Links ]
28 Sousa L, Carvalho M. Pessoa com osteoartrose na anca e joelho em contexto de internamento e ortopedia. In C. Marques-Vieira; L. Sousa (Eds.). Cuidados de Enfermagem de Reabilitação á Pessoa ao Longo da Vida. Loures: Lusodidata; 2017: 405-420. [ Links ]
Received: August 25, 2018; Accepted: November 26, 2018; Published: December 06, 2018
 Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
