










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkRevista Portuguesa de Enfermagem de Reabilitação
Print version ISSN 2184-965XOn-line version ISSN 2184-3023
RPER vol.1 no.1 Silvalde June 2018
https://doi.org/10.33194/rper.2018.v1.n1.05.4390
Articles
THE IMPACT OF LOWER URINARY TRACT SYMPTOMS ON PATIENTS WITH MULTIPLE SCLEROSIS
1- Centro Hospitalar e Universitário de Coimbra
2- Escola Superior de Enfermagem de Coimbra
This study aimed to describe the impact of lower urinary tract symptoms on the health-related quality of life of patients with Multiple Sclerosis, using Qualiveen, which assesses the impact, real and perceived, of urinary problems on the quality of life of people with spinal cord injury and multiple sclerosis. A quantitative, descriptive-correlational study was conducted with a nonprobability, convenience sample of 72 patients.
The most common lower urinary tract symptoms are mixed symptoms. Urinary urgency is the most frequent. The Impact of Urinary Problems on Quality of Life is evident. Higher scores were found among female patients, retired patients, patients requiring assistance for indoor and outdoor activities of daily living, and patients using protective devices. It is high correlated with the patient’s perception of how they urinate and moderate correlated with the number of lower urinary tract symptoms, the increased urinary frequency per day, and the years of evolution of lower urinary tract symptoms.
Lower urinary tract symptoms are a common problem in patients with Multiple Sclerosis, with an impact on their quality of life, with an urgent need, active and immediate intervention of the Rehabilitation Nurses.
Keywords: multiple sclerosis; urination disorders; quality of life
Este estudo pretendeu descrever o impacto que os Sintomas do trato urinário Inferior apresentam na Qualidade de Vida relacionada com a saúde das pessoas com Esclerose Múltipla, recorrendo ao Qualiveen, que avalia o impacto, tanto o real como o percecionado, dos problemas urinários na qualidade de vida das pessoas com lesão medular e com esclerose múltipla. É um estudo quantitativo, descritivo-correlacional. A amostra é não probabilística acidental constituída por 72 indivíduos.
Os sintomas do trato urinário inferior mais frequentes são os mistos sendo a urgência urinária o mais frequente. O Impacto dos Problemas Urinários na Qualidade de Vida é notório e apresentou maiores valores no sexo feminino, nos reformados, nos que necessitam de ajuda nas atividades de vida diária dentro e fora de casa e nas pessoas que usam dispositivos protetores. Apresenta correlação elevada com a perceção da pessoa sobre a forma como urina e correlação moderada com o número de sintomas do trato urinário inferior, a frequência urinária diária aumentada e os anos de evolução dos Sintomas do trato urinário Inferior.
Os sintomas do trato urinário inferior constituem um problema real das pessoas com Esclerose Múltipla e causam impacto real e percecionado na sua qualidade de vida, com necessidade urgente de intervenção ativa e imediata dos Enfermeiros de Reabilitação.
Palavras chave: qualidade de vida; esclerose múltipla; transtornos urinários
Este estudio pretendió describir el impacto que los Síntomas del Tracto Urinario Inferior presentan en la Calidad de Vida relacionada con la salud de las personas con Esclerosis Múltiple, con uso del Qualiveen, que evalúa el impacto, tanto el real como el percibido, de los problemas urinarios en la calidad de vida de las personas con lesions medulares y con esclerosis múltiple. Se trata de un estudio cuantitativo, descriptivo y correlacional. La muestra es no probabilística accidental y está constituida por 72 individuos.
Los Síntomas del Tracto Urinario Inferior más frecuentes son los mixtos, y la urgência urinária es la más frecuente. El Impacto de los Problemas Urinarios en la Calidad de Vida es notorio y presentó valores más elevados en el sexo femenino, en los jubilados, en los que necesitan ayuda en las actividades de la vida diaria dentro y fuera de casa y en las personas que usan dispositivos protectores. Presenta alta correlación con la percepción de la persona sobre la forma como orina, y correlación moderada con el número de Síntomas del Tracto Urinario Inferior, la frecuencia urinaria diaria aumentada y los años de evolución de los Síntomas del Tracto Urinario Inferior.
Los Síntomas del Tracto Urinario Inferior constituyen un problema real de las personas con Esclerosis Múltiple y causan impacto en su Calidad de Vida, con necesidad urgente de intervención activa e inmediata de los enfermeros de rehabilitación.
Palabras clave: esclerosis múltiple; trastornos urinarios; calidad de vida
INTRODUCTION
The quality of life related to a person's health assumes, nowadays, a relevant role in the decision-making of health professionals1. This growing concern emerges from the human and biological sciences, valuing not only the elimination of disease symptoms, the increase in average life expectancy and the decrease in mortality2, but above all to provide the best quality of life (QL) possible to all people regardless of their health status.
Although Multiple Sclerosis (MS) differs from person to person, in its vast majority it causes lesions in the myelin sheath of nerve fibers, which causes limitations in the short/medium term. Despite the high probability of being fully visible and evident limitations, in some cases they can be discrete and subjective, being initially devalued by both the person and the physician, even before the diagnosis3.
These people have to start a re-adaptation process in order to be able to respond to the new demands and needs imposed by the disease.
Health professionals must be equipped with knowledge and skills to be awake even to the most discrete and subjective signs and symptoms that may occur during the course of the disease, so that they can intervene in order to lessen their impact on the person's quality of life4.
For the awareness process to take place, favoring the transition process, these people need to be helped to clarify concepts and to demystify beliefs. Health professionals, especially rehabilitation nurses, are professionals privileged by their proximity to people and by the knowledge they contain to help them in this process5.
MS, like so many other pathologies of the central nervous system, has been the subject of many studies. However, and contrary to what one might think, epidemiological studies are very scarce in Portugal5. In fact, research studies focus essentially on clinical trials, which fortunately translate into a significant increase in available therapies, which, in turn, ensure not only a delay in the occurrence of outbreaks, but also a delay in their progressive evolution of disease3. However, studies that analyze the dimension of the problem, with regard to the incidence/frequency of the most diverse signs/symptoms and the investigation of their interference in the quality of life of these people, are still very small in number6.
Developing the person's ability to be able to control some of the symptoms as well as the reaction to these same symptoms that result from the existence of MS lesions is a concern of health professionals, since we are talking about a young adult who, in addition to being permanently afraid of the course of his illness, needs to remain professionally active to remain psychologically healthy as well5.
Lower urinary tract symptoms (LUTS) reveal to be a major problem and an impacting cause regarding the incapacity of people with MS, affecting social relationships and their daily activities, decreasing their quality of life7.
The purpose of this study is to increase knowledge in this area, contributing to facilitate the health-disease transition process for people with MS in order to improve the quality of life of these people, enhancing their autonomy/independence, keeping them professionally active as long as they can. Answers are sought to the following questions: “What are the most frequent lower urinary tract symptoms in people with Multiple Sclerosis? What impact do lower urinary tract symptoms have on the quality of life of people with Multiple Sclerosis? Will lower urinary tract symptoms contribute, as referred to in literature, to a decrease in the quality of life of people with Multiple Sclerosis?”, with a general objective of “describing the impact that lower urinary tract symptoms have on the quality of life related to the health in people with multiple sclerosis”.
MATERIAL AND METHODS
The quantitative research method is used, as data were collected in a systematic, observable and quantifiable way8 through two questionnaires.
It is a level II study because the objective is not only to describe the variables, but also to identify the existence of relations between them8. The purpose of a descriptive studie is observe, describe and document the aspects of a situation; while in descriptive-correlational studies it is also important to explore and to determine the existence of relations between the variables, and then to describe these same relations; it is not the target of the investigation to establish a causal connection9.
In this study, two distinct questionnaires were used: a clinical questionnaire, in order to characterize the sample according to the date of diagnosis, year of symptom onset, date of onset of urinary symptoms and the presence of lower urinary tract symptoms. To analyze urinary symptoms, 13 questions were asked about the presence or not of lower urinary tract symptoms (storage, emptying and post-emptying) defined in 201510, using closed questions (Yes/No).
All participants who had at least one LUTS received the second questionnaire to measure the impact of LUTS on QL. To assess this impact, the Qualiveen - Português (European) questionnaire was used by Véronique Bonniaud, owned by Coloplast and Véronique Bonniaud, deposited at the Mapi Research Institute (http://www.mapi-research.fr/). The Portuguese (European) version was culturally validated for Portugal by us, awaiting publication in another scientific journal of this process. This validation allowed conceptual and linguistic equivalence, demonstrating that this instrument has excellent reliability (Cronbach's alpha of 0.96), as well as convergent and discriminant validity.
Qualiveen consists of two sections, the first one with 30 questions that assess the impact of urinary changes on the person's health-related quality of life in 4 dimensions (Annoyances, Limitations, Concerns and Impact on quality of life). And the second, which contains 9 questions that assess the quality of life in general and one that assesses the person's perception of their way of urinate.
QL varies between -2 and +2 and negative values mean a decrease in QL. The dimensions of the impact on QL vary between 0 and 4. Regarding to the result, the closer to 4, the greater the impact of LUTS on QL.
The study sample is accidental non-probabilistic, and all people with MS and LUTS who attended the nursing consultation or day hospital of a Neurology service of a Central Hospital between the period of December 3, 2016 and January 14, 2017 were part of it. Data were collected by the author of this article, prior to the nursing consultation or scheduled treatment, in the reffered timeline. Since the objective is to study relationships between variables, a non-probabilistic sample may sufficient8.
Inclusion criteria were clinical diagnosis of MS, cognitive ability to answer questionnaires, age over 18 years-old, knowing how to read and write, and the exclusion criteria were pregnant women, women with gynecological pathology, people with a medical diagnosis of not medicated urinary tract infection, and if medicated, that they remain with alterations in the urination pattern potentiated by the infection, as well as men with diagnosed and untreated prostatic pathology.
The study was authorized by the Institution's Ethics Committee and informed consent was obtained from all participants.
In the statistical analysis, the variables that follow a normal distribution were represented by the mean (M) and the standard deviation (σ) was used as a measure of dispersion. Because most of the data do not show a normal distribution curve, we had to resort to the median (Md) and the interquartile range (IQR) was used as a measure of dispersion.
Qualitative variables were described by absolute (N) and relative (%) frequencies.
To explore the relations between quantitative or qualitative ordinal variables, Spearman's correlation coefficient (ρ) was determined and the test was evaluated for its significance, since in all the variables studied, at least one of them did not present normal distribution, which did not allow us to use the Pearson correlation coefficient11.
The variation of a variable that on average is explained by another is presented by the coefficient of determination, which is the squared elevation of ρ (ρ2), which varies between 0 and 1. It is usually represented in percentage terms and is considered relevant between 10% and 25%12.
To investigate the relationship between quantitative and qualitative nominal variables, since the data distribution does not present a normal distribution, we resorted to the use of non-parametric tests11,13. The Wilcoxon-Mann-Whitney test (U) was used, the asymptotic distribution was chosen when in each category n ≥ 10 or the exact distribution if n < 1012, for the investigation of the relationship between dichotomic nominal quantitative and qualitative variables. To investigate the relationships between nominal quantitative and qualitative variables, the Kruskal-Wallis test (H)12,13 was used, with the exact distribution being selected whenever in 3 groups on ≤ 5 and in all other situations the asymptotics distribution was used12.
A significance level of 5.00% (sig.=0.05) was adopted in this study, allowing us to affirm the existence of the tested relationships in 95.00%. We considered p ≥0.05: not significant; p<0.05: statistically significant, p<0.01 statistically highly significant and p<0.001 statistically highly significant14.
All analysis was performed using the IBM SPSS software (Statistical Package for the Social Sciences) Statistics version 23.0.
RESULTS
As the main objective of this investigation was not to identify the prevalence of LUTS in people with MS, it was considered pertinent to analyze this data. We noticed that of the 81 people who agreed to participate in the study, 72 had at least one LUTS, corresponding to 88.9%.
The sample subject to Qualiveen consisted of 72 people, 22 males and 50 females, aged between 25 and 71 years old (mean of 45.72 years old and standard deviation of 10.16 years old). The distribution by the variable and level of academic training is heterogeneous. With regard to employment status, 50% of individuals are retired, while 34.72% are professionally active (working for themselves or someone else) and the other 15.28% are unemployed. 72.2% live with a partner, 19.4% live with other people and 8.3% live alone. 70.8% do not need daily help at home and 72.2% do not need daily help outside home. 95.8% of people do not need help to urinate. 84.7% people walk, 12.5% use a manual wheelchair and 2.8% use another type of auxiliary device (crutch and walking stick).
The median years of MS evolution since diagnosis is 12 years, with an IQR of 14.3 years. As a minimum of years of evolution of MS we have 1 year and a maximum of 37 years.
Taking into account only the 80.6% of cases with LUTS who know the date of onset of symptoms, these cases presented as inaugural symptoms in 12.1% and 63.8% occurred as symptoms before the date of diagnosis, while 24, 1% of cases occurred after diagnosis. 23.6% have already undergone treatments for LUTS, and 4.2% have already undergone surgical intervention.
Out of the individuals who are part of the sample, 90.3% spontaneously urinate, 6.9% use self-catheterization, 2.8% resort to bladder emptying by another person, 15.3% resort to abdominal pressure to urinate, 1, 4% have urinary incontinence and 1.4% have permanent bladder drainage.
In the last 6 months, 19.4% of individuals report having presented a change in the way they urinate.
The use of protective means, absorbent (dressing, diaper or underwear)/external urinary device, occurs in 58.3% of the sample. Out of these, 1.4% because they are permanently incontinent, 38.1% use them because they have regular losses between urinations and during rest as a precaution.
By analyzing the LUTS, we considered only 71 individuals, since 1 individual had continuous bladder drainage and did not respond to the LUTS perception questionnaire. We found in the 71 individuals that the highest frequencies are the presence of 4 LUTS as shown in table 2.
Table 1 Sample distribution in different variables
| Variables | N | % | Mean | Standard deviation | Median | IQR | |
|---|---|---|---|---|---|---|---|
| Gender | Female | 50 | 69.00 | ||||
| Male | 20 | 30.60 | |||||
| Age | (25-71) | 45.72 | 10.16 | ||||
| Employment Status | Retired | 36 | 50.00 | ||||
| Cohabitation | Companion/other | 66 | 91.70 | ||||
| Help outside the home | No | 52 | 72.20 | ||||
| Help at home | No | 51 | 70.80 | ||||
| Help to urinate | No | 69 | 95.80 | ||||
| Ways of moving | Walking | 63 | 87.50 | ||||
| Years of evolution of MS | (1-37) | 12.00 | 14.30 | ||||
| Years after the first occurrence of symptoms | 1st Symptoms led to the diagnosis | 35 | 48.60 | ||||
| Years after the first occurrence of lower urinary tract symptoms | Inaugural | 7 (58) | 12.10 | ||||
| Before the date of diagnosis | 37 (58) | 63.80 | |||||
| Medical treatment of urinary problems | Yes | 17 | 23.60 | ||||
| Bladder emptying | Spontaneously | 65 | 90.30 | ||||
| Use of protective devices | Yes | 42 | 58.3 | ||||
| Reason for using the protective device | Precaution | 25 | 59.50 | ||||
| Quality of life | -0.10 | 0.83 |
Table 2 Distribution of the number of LUTS per individual in the sample
| Number of LUTS per individual | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | Total |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N | 7 | 3 | 7 | 13 | 5 | 8 | 12 | 4 | 4 | 7 | 0 | 0 | 1 | 71 |
| % | 9.86 | 4.23 | 9.86 | 18.31 | 7.04 | 11.27 | 16.90 | 5.63 | 5.63 | 9.86 | 0 | 0 | 1.41 | 100 |
The most frequent symptom is urinary urgency in 69% of individuals. 50% of individuals reported nocturia, frequency and feeling of incomplete emptying, more than 40% of individuals reported urgent incontinence, urinary incontinence, slow urinary stream and altered urinary stream, more than 30% reported hesitation, stress urinary incontinence and intermittent urinary flow, 28.6% reported needing abdominal effort to initiate urination and 16.7% had nocturnal enuresis.
The vast majority (73.3%) have mixed LUTS (emptying and storage), and only 2.8% have only empty LUTS and 23.9% only storage LUTS.
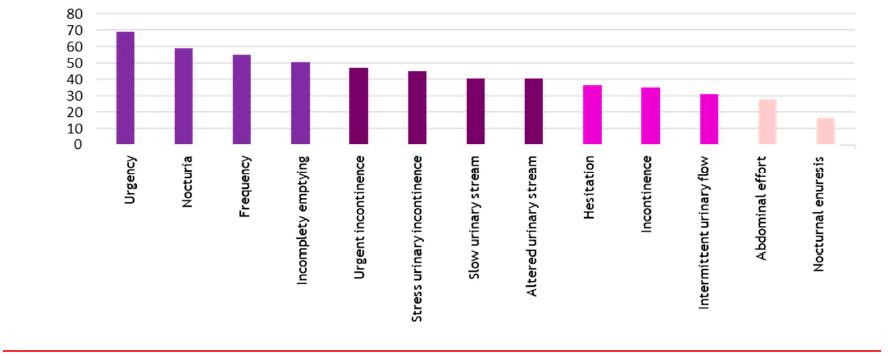
Table 3 Number of LUTS storage and LUTS emptying per individual
| 0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | Total | ||
|---|---|---|---|---|---|---|---|---|---|---|
| LUTS Storage | n | 2 | 12 | 16 | 10 | 11 | 8 | 10 | 2 | 71 |
| % | 2.82 | 16.90 | 22.54 | 14.08 | 15.49 | 11.27 | 14.08 | 2.82 | 100 | |
| LUTS Emptying | n | 17 | 9 | 16 | 11 | 7 | 6 | 5 | - | 71 |
| % | 23.94 | 12.68 | 22.54 | 15.49 | 9.86 | 8.45 | 7.04 | - | 100 | |
Regarding urinary frequency, 41.4% urinate 9 or more times a day, up to a maximum of 15 times, while 59.4% urinate more than twice during the night, up to a maximum of 7 times.
Analyzing the impact of urinary problems on health-related quality of life (IUPQL), the median of the sample is 1.33, with an IQR of 1.66, with a minimum value of 0.00 in the sample and a maximum value of 3.44. We found that only 4.2% had no impact on quality of life and 25% had an IUPQL above 2.00.
In the annoyances dimension, the median is 1.22, the IQR 1.95, with a minimum value of 0.00 and a maximum of 4.00. In the dimension limitations, the median is 1.25 to 2.38 IQR, with a minimum value of 0.00 and a maximum value of 3.75. In the area of concerns, the median is 1.56, the IQR 1.63, with a minimum value of 0.00 and a maximum value of 3.00. Regarding the impact on daily life, the median is 0.80, the IQR 1.95, with a minimum of 0.00 and a maximum of 4.00.
The mean quality of life of the sample was -0.1 with a standard deviation of 0.834 with a minimum of -2.00 and a maximum of 1.56.
Regarding the person's perception of their way of urinating, we found 9.7% who considered to urinate very well, 29.2% who considered to urinate relatively well, 22.2% considered to urinate neither good nor bad, 15 .3% consider to urinate relatively badly and 23.6% consider to urinate very badly.
In order to understand the existence or not of relations and correlations, several variables were crossed using statistical tests.
Several relations were found in the sample, significant relations, where the IUPQL is higher in women (Mann-Whitney test, p=0.045 ) and in people who need daily help at home (Mann-Whitney test, p=0.023), very significant relations, where the IUPQL is higher in retired people (Kruskal-Wallis test, p=0.005) and in people who need daily help outside home (Mann-Whitney test, p=0.002) and we found a relations highly significant where the IUPQL is higher in those using protective devices (Mann-Whitney test, p=0.00).
We found moderate, highly significant correlations, where the variation in the IUPQL result is explained in 30.69% by the number of LUTS (ρ <0.001, rho=0.554) and is explained in 19.27% by the daytime urinary frequency (p<0.001, rho=0.439). We identified a very significant correlation, where the variation in the IUPQL result is explained in 19.01% by the years of evolution of urinary tract symptoms (p<0.01, rho= 0.436). We found a high correlation, highly significant, where the variation in the IUPQL result is explained in 64.16% of the person's perception of the way they urinate (p<0.001, rho= -0.801).
Other weak but not relevant correlations were found (IUPQL with years of symptom evolution, years of MS evolution and nocturnal urinary frequency) and non-existent correlations and relationships (IUPQL with age, education, cohabitation, form of displacement, help to urinate , years after the first occurrence of lower urinary tract symptoms, medical treatment of urinary problems).
DISCUSSION
The data obtained reveal very interesting findings and some surprising ones. This is a young adult sample, with proportions of incidence in the sexes according to the literature, with years of disease evolution of a median of 12 years and in which the first symptoms of the disease were in almost half of the sample those that led to the diagnosis of MS. We found higher IUPQL values in women. Nowadays, women still assume two distinct roles, family and professional, the impact occurs in both spheres, which may justify the findings found15.
Although the correlation found between the years of evolution of MS symptoms and IUPQL is weak and with little relevance, it is an obvious relationship due to the usual evolution of this disease, almost always with worsening of existing deficits.
We found a higher IUPQL in people who need help both at home and away from home, a relationship that we understand, since in the presence of difficulty in performing activities of daily living due to fatigue, musculoskeletal changes, among many others, the presence of a LUTS causes greater concern/limitation/inconvenience. The presence of LUTS, which enhance concerns/limitations/inconveniences, results in a decrease in QL.
Half of the people in the sample are retired. Physical limitations resulting from MS, particularly those resulting from fatigue (one of the main symptoms), result in the impossibility of performing professional tasks in the normal time4,16. In terms of employment, unfortunately these people, for the most part, do not find a suitable workplace for the limitations presented, which leads to them becoming professionally inactive, although many of them have skills. The employment situation is related to the IUPQL, and we found higher values in retired people.
With regard to LUTS, as reported in the literature17,18, these can be the inaugural of the disease, and we found 12.10%, in which the LUTS were initial to the diagnosis, while 63.8% the LUTS appeared even before the diagnosis. We consider these data very important, as it requires a greater appreciation of these symptoms. One author19 states that LUTS are often undervalued and not associated with the disease, and this study only shows that they are symptoms of the disease and that they can be present in the earliest stages. However, unlike a study we consulted20, we found a statistically significant correlation, positive and moderate, in which, the years of evolution of urinary symptoms explain 19.01% of the variation in the IUPQL. In any case, this relations is explainable considering that the older the person is with LUTS, even if they do not evolve or worsen, the greater will be the concerns, limitations, fears and impact on daily life, which will possibly lead to people value these symptoms more, which causes greater impact on their quality of life conditioned by urinary problems.
Although almost all people in our sample urinate spontaneously, half feel the need to constantly use a protective device, and most of them just in case. These people, even controlling urination, seem to feel a concern about the occurrence of urinary loss, which influences their lives, compatible with the relationship found, in which the highest values of the IUPQL are in people who use individual protection.
The more types of LUTS felt by people (90% have more than one LUTS), the higher the IUPQL explained in 30.69%. In previous studies20,21 that analyzed this relationship, a moderately statistically significant relationship was also found in 2004 and a strong statistically significant relationship in the 2006 study, the concerns felt and the greater the impact on the quality of life of the person with MS and LUTS.
The vast majority of the sample, 73.3%, has mixed LUTS, which is similar to a study22 that found the prevalence of both symptoms to be 70%. In another study8 the prevalence of mixed symptoms is 50%.
Urinary urgency is found in more than half (69%) of our sample, a value similar to that found in a study23 in which urinary urgency had a frequency of 83%, and in another study24 which found 70.2% of urinary urgency present in people with MS.
One of the LUTS that does not have a consensus in the literature is incontinence. A frequency of 83%23, 75%19, 59%6, and only 10%25 was found in the consulted studies. In this study, incontinence is found with a frequency of 35.2%, being the tenth LUTS most frequently found.
The existence of a correlation between the increased daily urinary frequency and the IUPQL would be expected, considering that this is a symptom that causes changes in the person's daily dynamics, which can cause disturbances at personal and professional level, but such correlation was not verified. Was also expected to find a correlation of IUPQL with nocturia/nocturnal urinary frequency as it interferes with sleep and rest, but such relationship was not verified. It would be importante in the future, studies to deepen this subject.
The existance of a significant impact of urinary problems on the quality of life of people with MS are results coincident with the results obtained in a study carried out in 201626.
In all Qualiveen dimensions tehre are consequences for QL. The area that has the greatest consequences on the person´s quality of life due to urinary problems are limitations, followed by concerns, annoyances and then impact on quality of life. In the study of 201626 the areas with the greatest impact on pleople´s lives due to urinary problems appear in exactly same order.
CONCLUSION
The presence of LUTS in people with MS is often undervalued, both by people themselves and by health professionals, essentially if they are shown together with other more evident and more disabling symptoms, these remain in the background.
This study showed us that LUTS have a negative impact on the QL of people with MS and also revealed that these people have multiple LUTS, with urinary urgency being the most frequently found.
The IUPQL is higher among women, retired people, those who need daily help inside and outside the home, and those who wear protective devices.
A high correlation was found between the IUPQL and the person's perception of the way they urinate. Several moderate correlations were found between the IUPQL and the number of LUTS, increased daily urinary frequency and years of evolution of urinary tract symptoms.
We were concerned to understand which LUTS caused the highest IUPQL, but due to the size of the sample we were not able to use statistical tests that would allow us to unveil these responses, from our point of view, it will be an added value to study these relationships in future studies.
Rehabilitation nurses are professionals who have the ability to transform this knowledge into useful tools in order to increase the quality of life of people with Multiple Sclerosis and LUTS. This promotes early diagnoses, develops preventive actions, preventing complications and avoiding disabilities, maintaining or recovering the personal and professional activity of the person with LUTS and MS.
Once this problematic is identified, it will make sense to change professional practices and acquire new behaviors, that is, questioning the presence of LUTS in all people with MS, even without manifestations of its presence, both in order to prevent future complications such as higher Urinary tract Infection , with a view to referring to an earlier medical diagnosis or to teach, instruct and train these people to deal with their LUTS in order to lessen their impact on their quality of life, reducing inconveniences, limitations, concerns and impact on daily life.
Monitoring the effectiveness and efficiency of implemented interventions is an asset in order to assess their individual suitability. For this monitoring of results it may be important to use Qualiveen.
Qualiveen is a strong tool for diagnosing and evaluating the results of interventions implemented by nurses.
It is suggested in future studies to identify which nursing interventions allow reducing the IUPQL of people with MS.
REFERÊNCIAS
1 Stohrer M, Blok B, Castro-Diaz D, Chartier-Kastler E, Popolo G, Kramer G.et al. Orientações sobre disfunção neurogénica do tracto urinário inferior. 2009. Recuperado de http://www.apurologia.pt/guidelines/Disf-Neurog-Tract-Urin-Inf.pdf [ Links ]
2 Nader BB. Tradução, validação e adaptação cultural do questionário qualiveen short form (Dissertação de mestrado). Universidade Estadual de Campinas, Faculdade de Ciências Médicas, Brasil; 2016. [ Links ]
3 Guimarães J, Sá MJ. Esclerose múltipla e outras doenças inflamatórias e desmielinizantes do sistema nervoso central. In M.J. Sá (Ed.) Neurologia Clínica: Compreender as doenças neurológicas (2ª ed.). Porto, Portugal: Edições Universidade Fernando Pessoa; 2014:373-432. [ Links ]
4 Barrett M, Ben-Zacharia A, Blaschuk C, Costello K, Easterling C, Gutierrez A, Uchil A, Et al. Nursing Management of the Patient with Multiple Sclerosis: AANN, ARN, and IOMSN Clinical Practice Guideline Series. Illinois, Estados Unidos da América: Teva Neuroscience; 2011. [ Links ]
5 Sá JC, Cordeiro C. Esclerose Múltipla. Porto, Portugal: Ambar; 2008. [ Links ]
6 Pavan K, Miguez PB, Marangoni BE, Tilbery CP, Lianza S. Comportamento da incontinência urinária em pacientes com esclerose múltipla e a sua influência na qualidade de vida. Med Reabil. 2010;29(1):1-5. [ Links ]
7 Amarenco G, de Sèze M, Ruffion A, Ismael SS. Clinical and urodynamic evaluations of urinary disorders in multiple sclerosis. Annals of physical and rehabilitation medicine. 2014 Jul 1;57(5):277-87. doi: /10.1016/j.rehab.2014.05.006 [ Links ]
8 Fortin M. Fundamentos e etapas do processo de investigação. Loures, Portugal: Lusodidacta; 2009. [ Links ]
9 Polit DF, Beck CT, Hungler BP. Fundamentos de pesquisa em enfermagem: Métodos, avaliação e utilização (5ª ed.). Porto Alegre, Portugal: Artemed; 2004. [ Links ]
10 Khalaf KM, Coyne KS, Globe DR, Armstrong EP, Malone DC, Burks J. Lower urinary tract symptom prevalence and management among patients with multiple sclerosis. Inter J MS care. 2015 Jan;17(1):14-25. doi: 10.7224/1537-2073.2013-040. [ Links ]
11 Hill MM, Hill A. Preparação final do questionário. Investigação por questionário. (2º Ed.). Lisboa, Portugal: Edições silabo; 2012. [ Links ]
12 Pestana MH, Gageiro JN. Análise de dados para ciências sociais: a complementaridade do SPSS. (6ª ed.). Lisboa, Portugal: Edições Sílado; 2014. [ Links ]
13 Marôco J. Análise estatística com o SPSS Statistics (5º Ed.). Sintra. ReportNumber, Lda; 2011. [ Links ]
14 D'Hainaut L. Conceitos e Métodos de Estatísticas II (4º ed.). Lisboa, Portugal: Fundação Calouste Gulbenkian; 1992. [ Links ]
15 Cruz S, Almeida A, Ferreira S, Mendes AC. Qualidade de vida em doentes com esclerose múltipla: estudo da influência da vulnerabilidade e da resiliência ao stress na sua avaliação. Psiquiatr Clin. 2004;25(2):107-14. [ Links ]
16 Sá MJ. Esclerose múltipla. Sumário de lição elaborado nos termos da alínea c) do nº2 do artigo 4º do Regulamento nº 307/2008, publicado no Diário da Republica, 2ª Série, nº110, de 9 de Junho de 2008. Porto, Portugal: Universidade Fernando Pessoa, Faculdade de Ciências da Saúde; 2012. [ Links ]
17 Coelho MM. Avaliação urodinâmica na esclerose múltipla. Acta Urol. 2009;3:9-14. [ Links ]
18 Silva TO, Monteiro LA. Perturbações miccionais da esclerose multipla. Acta Urol. 2006; 23(1): 61-7. [ Links ]
19 Bonniaud V, Parratte B, Amarenco G, Jackowski D, Didier JP, Guyatt G. Measuring quality of life in multiple sclerosis patients with urinary disorders using the qualiveen questionnaire1. Arch Phys Medi Rehabil. 2004 Aug 1;85(8):1317-23. [ Links ]
20 Bonniaud V, Bryant D, Parratte B, Gallien P, Guyatt G. Qualiveen: a urinary disorder- specific instrument for use in clinical trials in multiple sclerosis. Arch Phys Medi Rehabil. 2006 Dec 1;87(12):1661-3. [ Links ]
21 Onal B, Siva A, Buldu I, Demirkesen O, Cetinel B. Voiding dysfunction due to multiple sclerosis: a large scale retrospective analysis. Int Braz J Urol. 2009 Jun;35(3):326-33. [ Links ]
22 Fria AM, Cuzzati BA, Lopes GA, Lima RA. Disfunção Urinária em Paciente Portadora de Esclerose Múltipla. Rev Neurocienc. 2013;21(2):247-50. [ Links ]
23 Blosfeld CE, SOUZA SD. Tratamento da incontinência urinária em mulheres com esclerose múltipla (EM): série de casos. Rev Neurocienc. 2012;20(1):58-67 [ Links ]
24 Khan F, Pallant JF, Shea TL, Whishaw M. Multiple sclerosis: prevalence and factors impacting bladder and bowel function in an Australian community cohort. Disabil Rehabil. 2009 Jan 1;31(19):1567-76. [ Links ]
25 Ciudin A, Franco A, Diaconu MG, Peri L, Vivas V, Gozalez MA, Alcaraz A. La calidad de vida de los pacientes con esclerosis múltiple: Traduccion y validacio de la version en castellano de qualiveen. Ann Urol, 2012; 20-23. [ Links ]
26 Denys P, Phe V, Even A, Chartier-Kastler E. Therapeutic strategies of urinary disorders in MS. Practice and algorithms. Ann Phys Rehabil Med. 2014 Jul 1;57(5):297-301.. doi: 10.1016/j.rehab.2014.05.003 [ Links ]
Received: May 28, 2018; Accepted: June 20, 2018; Published: June 23, 2018
 Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
