











 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
Permalink
Introduction
Several case reports have previously shown that massive rotator cuff tears can lead to large cysts extending from the subacromial space through the acromioclavicular joint into a subcutaneous cyst, with a characteristic “geyser sign” on imaging.1-6 One single and recent study has reported extension through the deltoid muscle.7 However, to our knowledge, no cases of transdeltoid pseudo-cyst as the first manifestation of septic arthritis have ever been reported.
Case Report
A 79-year-old female, with a clinical history of arterial hypertension and dyslipidemia, under telmisartan + hydrochlorothiazide, 80 mg + 25 mg, and simvastatin, 20 mg, both once daily, presented to the Emergency Department (ED) with a two-day evolution of a painful tumefaction over her right shoulder (Fig. 1). She denied any history of recent trauma. During the physical examination, she showed limited passive and active range of motion. A mass could be palpated in the lateral side of her right shoulder, measuring about 5 cm, associated with local heat, redness, swelling and pain. The redness was extended to the armpit area and multiple adenopathies could be palpated in the axillary region, with 2 to 3 cm. The tympanic temperature was 37.5ºC. The medical records showed the patient had been admitted to the hospital 16 days before, after being bitten by a neighbor’s dog on her left leg; objective examination was then normal, and she was discharged medicated with oral antibiotic therapy (amoxicillin + clavulanic acid, 875 mg + 125 mg, every 12 hours, for 8 days) and appropriate wound dressings’ advice. Right shoulder ultrasound on admission was notable for a voluminous and heterogeneous, yet inconclusive, subcutaneous fluid collection. Puncture and drainage of the lesion were performed, resulting in 10 mL of a pasty serohematic fluid; cytological examination revealed a total cell count of 50320 cells/mL, with a predominance of polymorphonuclear leukocytes (92.7%). Blood tests were notable for an increase in C-reactive protein levels (34.3 mg/dL). Magnetic resonance imaging (MRI) of the right shoulder was performed, which revealed massive rupture of the rotator cuff tendons involving the entire supraspinatus and infraspinatus and the upper segment of the subscapularis muscle. Also, it was notable for blurring of the tendon of the long portion of the biceps and moderate effusion in the glenohumeral and acromioclavicular joint cavities, with fluid leakage into the subacromial/ subdeltoid bursa. The glenohumeral joint cavity demonstrated "decompression" to the subcutaneous cell tissue through a linear defect in the lateral aspect of the deltoid muscle body, where it presented as a collection measuring about 33 x 30 x 40 mm (Figs. 2 and 3). Blood and synovial fluid cultures were negative. The diagnosis of septic arthritis was presumed based on the clinical history and articular fluid cytological examination. The patient was initially proposed for surgical debridement and irrigation of the right shoulder, not only to improve the prognosis, but also to perform the culture of the synovial fluid collected during surgery and possibly target antibiotic therapy. However, given the clinical and analytical improvement of the patient condition during hospital stay, it was decided not to undergo surgical treatment.

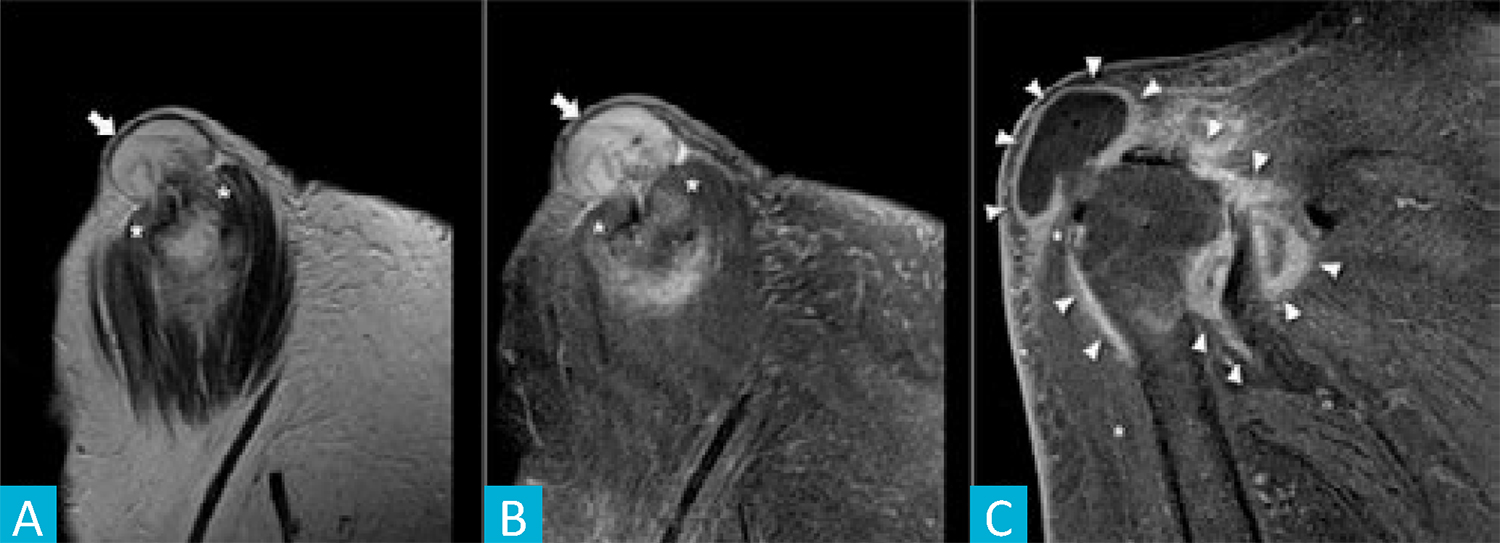
Figure 2: Pseudo-geyser. Sagital T2w weighted (A) and sagital T2w fat-saturated (B) MR images depicting the pseudo-geyser [arrow] protruding through a full thickness tear near the proximal insertion of the deltoid [asterisk]. Coronal T1w fat-saturated MR image after intravascular administration of gadolinium (C) showing the hyper-enhancement of the pseudo-geyser wall and the articular capsule, corresponding to the inflammatory/ infectious reaction.
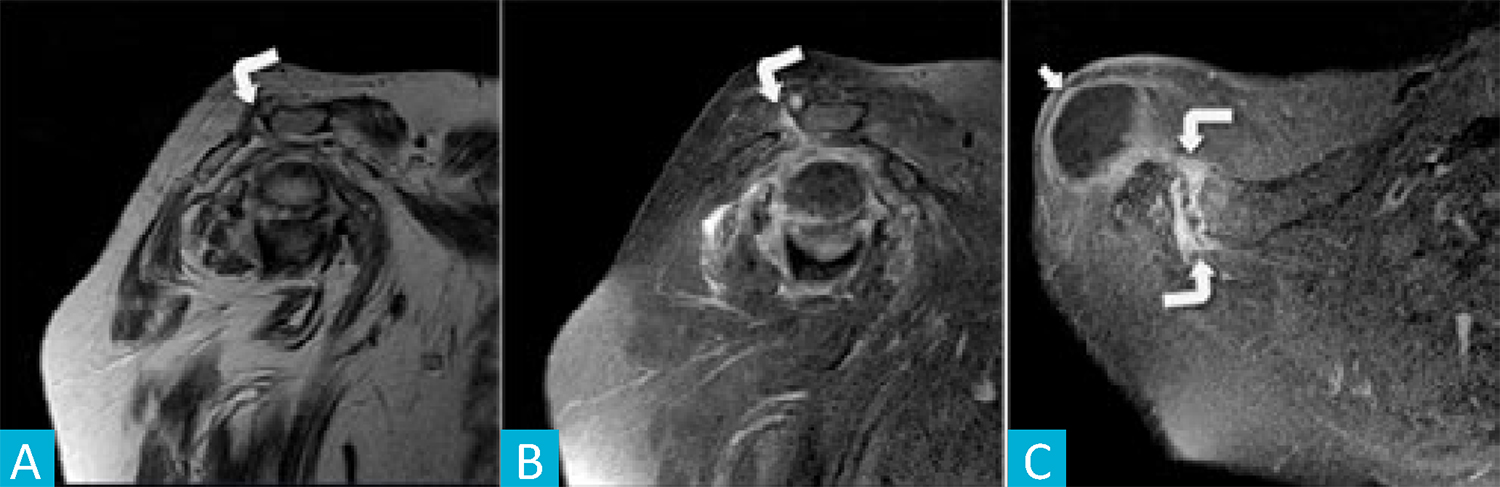
Figure 3: Pseudo-geyser. Sagital T1w (A), sagital T2w fat-saturated (B) and axial T1w fat-saturated after intravascular gadolinium (C) MR images depicting the acromioclavicular joint [curved arrow] with some degenerative changes, effusion and periarticular edema but with no relationship to the pseudo-geyser [arrow].
Conclusion
Septic arthritis, also known as infectious arthritis, represents a direct invasion of a joint space by various microorganisms, mainly bacteria,8 and the most common route of invasion of the joint is via the bloodstream.9 The MRI scan revealed a fluid-filled cyst extending from the subacromial space through the deltoid in the context of a long-standing massive rotator cuff tear, configuring a “pseudo-geyser sign” on imaging. Its growth and exuberant inflammatory signs were thought to be the result of an episode of septic arthritis in the context of apparent hematogenous spread due to the previous dog bite incident. Prior antibiotic exposure can justify not only the negative blood and synovial fluid cultures, but also the self-limited course of the disease. Though uncommon, septic arthritis is an orthopedic emergency that can cause significant joint damage, leading to increased morbidity and mortality. Clinicians should be aware of the signs and symptoms of septic arthritis, owing to the fact that the early diagnosis, prompt referral to the ED and treatment are crucial.4

