











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
Permalink
A 73-year-old male presented to the emergency department with diffuse abdominal pain. Physical and analytical evaluation revealed abdominal distension, meteorism and elevated C-reactive protein. Contrast-enhanced computed tomography (CECT) was performed revealing dilated bowel-loops with air fluid levels found in between two points of transition: proximally, a jejunum-jejunal intussusception adjacent to a jejunal lipoma; distally, an ileo-ileal intussusception with enlarged lymph nodes in its mesenteric fold (Fig.s 1 and 2). No pneumatosis intestinalis was present. The patient underwent urgent laparotomy exploration with resection of 40 cm of ischemic bowel.
Closed-loop obstruction (CLO) accounts for only 19% of cases of small bowel obstruction (SBO) and implies a segment of bowel that is obstructed at two points along its course, normally adjacent and resulting from a single constricting lesion.1,2 Adult intussusceptions (AI) are relatively rare, and most are related to an organic lesion serving as a lead point. Both are associated with a higher risk of ischemia requiring timely diagnosis and surgery.3,4
In small-bowel AI, usually a benign intraluminal lesion, such as lipoma or hamartomatous polyp, incites abnormal peristaltic movement and leads to the telescoping of one bowel segment (intussusceptum) into the adjacent segment (intussuscipiens).3,5 Patients usually present with acute or partial and recurring SBO. CECT can readily provide the diagnosis by noting the pathognomonic bowel-within-bowel appearance, which presents as a sausage-shaped or a target-like mass, when imaged in a right angle to the bowel wall or longitudinally, respectively. Identification of an intraluminal lead mass is often possible. However, determining the underlying etiology, especially when the mass is separate from the bowel, can be difficult.3,5 Few cases are reported of multiple intussusceptions in the same patient.6,7
In this case, there were two distant intestinal intussusceptions with lead points creating a CLO, with no evident signs of ischemia on CECT but detected intraoperatively.
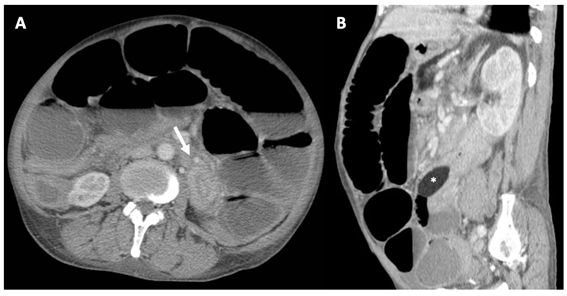
Figure 1: Closed-loop obstruction caused by two intestinal intussusceptions: Jejunum-jejunal intussusception. Admission contrast enhanced-computed tomography (CT) shows multiple distended bowel loops with air-fluid levels and the characteristic target-like lesion in the proximal jejunum in the axial plane (arrow in A). It is easily identifiable as being attributed to a well-marginated mass with fat attenuation compatible with a jejunal lipoma, seen in the sagittal reconstruction distal to the tapered lumen of the intussusceptum (asterisk in B).
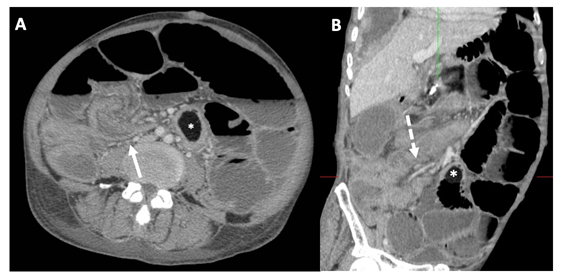
Figure 2: Closed-loop obstruction caused by two intestinal intussusceptions: Ileo-ileal intussusception. The same CT shows, in an inferior axial plane, invagination of a distal ileal loop with its mesenteric fold into the lumen of a contiguous portion of the bowel (arrow in A). Multiple mesenteric lymph nodes were present, as seen in this coronal reconstructed image (dashed arrow in B), probably responsible for the intussusception. Also shown is the jejunal lipoma (asterisks in A and B).

