











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
Permalink
Case
A 34-year-old man, presented to our institution with pain and motor weakness in the left thumb and digital extensors, after being severely assaulted by a knife in the left forearm, three weeks previously.
An ultrasound (figure 1) and MRI (figure 2) studies were performed for better characterization, showing a nodular area with 4 mm in caliber with a bulbous end appearance (figure 1) in a plane proximal to the Frohse's arcade, consistent with an amputation neuroma of the posterior interosseous nerve (figure 2). A biopsy was not made.
At surgery, dissection of the two heads of the supinator muscle was made, and the sectioned posterior interosseous nerve was identified. Neurostimulation of the nerve was unsuccessful and suture end to end was not possible. Consequently, the ends were brought together with a 4 mm neurotube and biological glue.
Nevertheless, after 6 months of physical rehabilitation with electrostimulation, the patient was still unable to extend the left thumb and fingers.
Discussion
Peripheral nerves are parallel unidirectional nerve axons encircled by perineurium, a connective tissue sheath. After focal traumatic injury, neural axonal tissue displays disordered proliferation at the site of trauma, resulting in a focal non-neoplastic area of enlargement called a traumatic neuroma.1
Two types of traumatic neuromas have been described, spindle neuromas and terminal neuromas. Spindle neuromas occur when the nerve trunk is injured but still intact, such as in traction injury or chronic repetitive stress. Terminal neuromas occur after transection of the nerve (such as limb amputation), presenting with a bulbous appearance at the end of the proximal fragment.1,2
Clinically, the most common symptom is pain. Physical examination may reveal a palpable mass at the site of previous trauma.
Ultrasound (US) and magnetic resonance imaging (MRI) are commonly used alone or in combination to study peripheral nerves and are the gold standard for radiologic diagnosis. By following the guidelines regarding soft tissue tumors in adults approved by the European Society of Musculoskeletal Radiology (ESSR) for peripheral nerve tumors, biopsy could be avoided in cases of purely benign lesions.2 US features such as a well marginated hypoechoic oval mass with echogenic strands in direct continuity with a nerve, allows to establish the possible neural origin of these soft tissue masses (figure 1).2
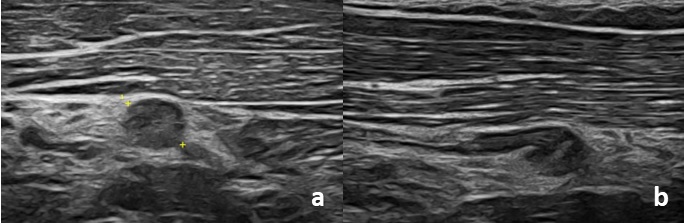
Figure 1: Along the course of the posterior interosseous nerve, immediately proximal to its entry into the arcade of Frohse, a hypoechoic nodular area of approximately 4 mm in diameter is identified (image a), without unequivocal distal continuity and with a bulbous end appearance (image b), suggestive of terminal neuroma (amputation neuroma).
On MR imaging, traumatic neuromas present normally with intermediate signal on T1-weighted images, and they tend to be isointense to hyperintense compared to muscle on proton density- and T2-weighted images, often approaching the hyperintense signal intensity of the associated nerve.2
Because intraneural fascicles may remain intact proximal to the injury site, traumatic neuromas often demonstrate clustered hypointense ring-like areas called the “fascicular sign” on T2-weighted images acquired perpendicular to the nerve, corresponding to nerve fascicles.
Variable contrast enhancement is seen.1,2
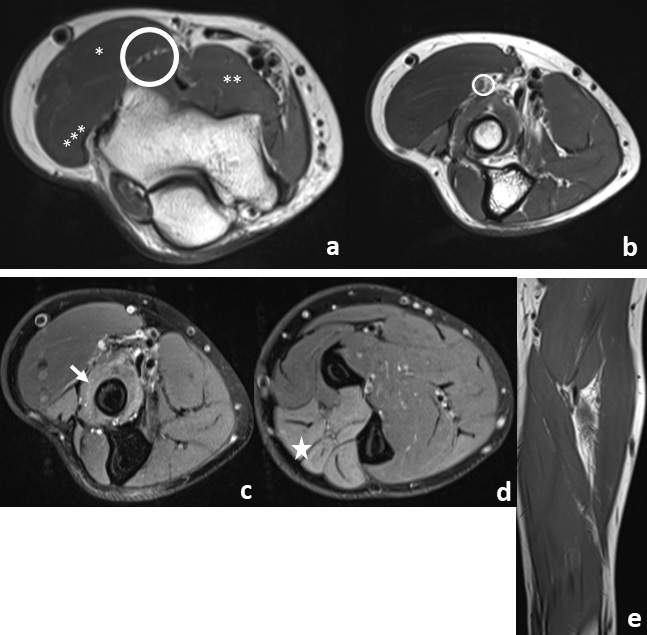
Figure 2 Image a - Axial PD-weighted image just above the elbow joint demonstrates the bifurcation of the radial nerve into the superficial radial nerve and posterior interosseous nerve (circle). The brachioradialis (*), brachialis (**), the extensor carpi radialis longus (***) are indicated. Image b - Axial PD-weighted image shows the posterior interosseous nerve, in a plane immediately proximal to its entry into the Frohse's arcade exhibiting a focal area of nodular thickening with approximately 4 mm in caliber, consistent with an amputation neuroma (circle). Image c, d and e - Axial PD-weighted fat suppressed and coronal T1 images show the supinator muscle (arrow) and extensor compartment muscles (star) with diffuse interstitial hyperintensity, indicating denervation edema in the territory of the posterior interosseous nerve, yet without associated atrophy or lipomatous infiltration (image e).
The treatment can be conservative including physical therapy, neuromodulation, alcohol ablation and medication, or surgical, by excision of the neuroma and repair of the nerve with direct anastomosis, graft, or conduit.1,3

