











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
Permalink
Case Report
A 71-year-old male patient, admitted to our hospital due to transient ischemic attack, was noticed to have a painless exuberant mass in the right clavicle during physical examination. No other relevant physical finding was noted, and the patient had no other complaint or symptom.
A plain radiography of the right clavicle was performed showing bone enlargement with a sclerotic pattern (figure 1).
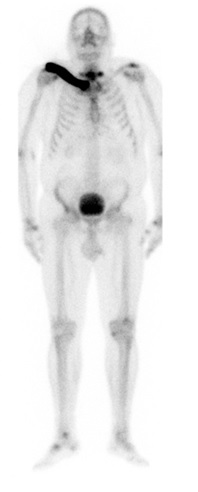
A shoulder computed tomography (figure 2) and a body radionuclide bone scintigraphy (figure 3) were later performed for further characterization with a coarsened trabecular pattern with cortical thickening and marked increased uptake of radionuclide being reported.
The biochemical study was also performed showing high alkaline phosphatase levels (260 U/L). The set of these findings suggests monostotic Paget´s disease, an atypical and rare location of the disease. In our case, the patient was treated with bisphosphonates (zoledronic acid 5 mg) and after one year of treatment, the alkaline phosphatase values were found to be in a normal range and no imagiological progression of the disease was noted (figure 1).
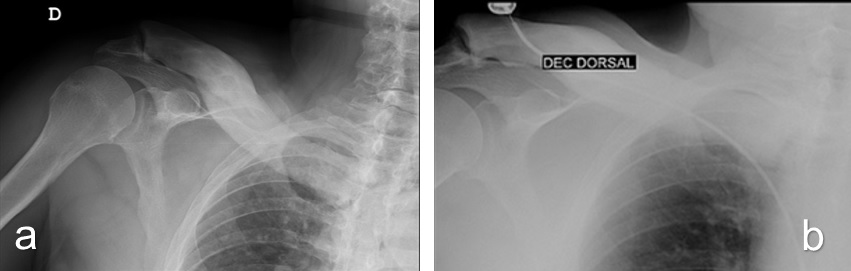
Figure 1: On conventional radiograph, a diffuse enlarged right clavicle is seen, with the loss of the medullary cavity, thickening of the cortex and a predominantly sclerotic pattern (image a). Note the stability after one year (image b), favouring the diagnosis of Paget´s disease.
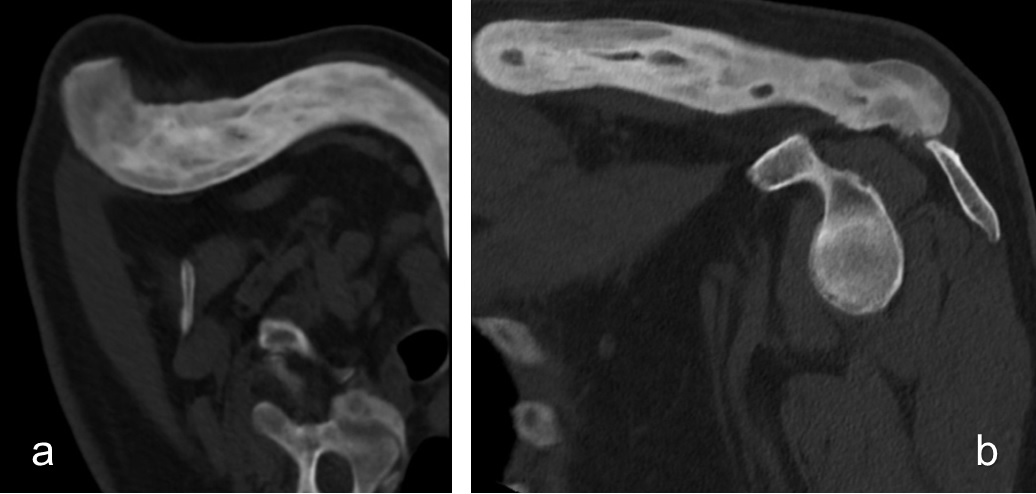
Figure 2: On computed tomography, a diffuse enlarged clavicle, with cortical thickening and coarse bone trabeculae is seen in axial view (a) and in coronal view (b).
Discussion
Paget disease of bone, which was first described in 1877 by Sir James Paget, is a chronic disease characterised by excessive abnormal bone remodelling. Prevalence increases with age, and it is more common in patients over 65 years of age. Certain geographical characteristics have been observed, being more common in the United Kingdom and Western Europe.1 It is commonly located in the pelvis, spine and skull, being the clavicle a rare site of involvement.2
Paget disease is associated with a plethora of radiological signs. Each phase has unique radiographic features that are normally sufficient to establish a diagnosis with confidence. All three phases may occur in the same bone in a synchronous or metachronous fashion. In most cases, the disease is an incidental finding on a radiological examination requested for other purpose.4
In fact, three phases have been described with a correlation between the radiological features of each phase and the histopathological appearances2:
-the lytic phase, in which osteoclasts predominate and there is osteolysis, giving the characteristic blade-of-grass appearance;
-the mixed phase, in which osteoblasts cause repair superimposed on the resorption, with subsequent development of trabecular, cortical thickening and enlargement of bone;
-the blastic phase, in which osteoblasts predominate and sclerosis is the dominant radiographic finding.
Bone scintigraphy, although being more sensitive than plain radiography, allowing the extent of disease to be determined, is not specific. An increased homogeneous tracer uptake is seen in all three phases of the disease,3 secondary to the high perfusion and high affinity of the tracer to the woven bone.4
Patients often have an elevated serum level of alkaline phosphatase (due to increased rate of bone formation), especially during the mixed and blastic phases, which may be used to monitor the level of activity and therapeutic efficacy.4) Increased serum and urine levels of hydroxyproline are more commonly seen in the lytic phase and are a precise marker of resorptive activity. Serum levels of calcium and phosphate are typically normal.2
It is important to note that bone turnover markers are not specific and the diagnosis is best established by a correlation of imaging, clinical and analytical findings.
Although osteosclerosis, bony enlargement, and a coarsened trabecular pattern are classical imaging features of Paget´s disease, they can be present in other pathologies, such as: chronic osteomyelitis, sclerotic bone metastasis (particularly from prostatic carcinoma), myelofibrosis, fluorosis, mastocytosis, renal osteodystrophy, fibrous dysplasia and tuberous sclerosis.
Nevertheless, additional findings in these other diseases validate the correct diagnosis, such as hepatosplenomegaly in myelofibrosis or mastocytosis, ligamentous ossification in fluorosis, focal radiodensity in mastocytosis and tuberous sclerosis, bowing deformities and ground-glass appearance in fibrous dysplasia, and subperiosteal and subchondral bone resorption in renal osteodystrophy.
Symptoms typically include localized pain, increased warmth (due to lesion hypervascularity), bone enlargement with bowing deformities and decreased range of motion. Mechanical compression of neurologic structures may occur and can cause deafness, visual abnormalities and other neurologic symptoms.2
Complications of Paget disease include the effects of osseous weakening (deformity and fracture), arthritis and neurologic symptoms. Sarcomatous transformation, seen as bone destruction extending through the cortex with an associated soft-tissue mass, is the most feared complication, and occurs in approximately 1% of cases.3
Symptomatic patients are normally treated with bisphosphonates. Analgesics and anti-inflammatory drugs may also be used for pain management. Subtle improvement of the radiographic appearance may be seen with the treatment.2
Recognition of the radiological spectrum of the appearances of Paget´s disease usually allows prospective diagnosis and differentiation of its associated complications, which helps guide therapy and improve patient management.

