











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
INTRODUCTION
Cutaneous metastases from visceral neoplasms occur most frequently in relation to melanomas, breast carcinomas, and carcinomas of the respiratory tract.1,2They are often located on the scalp, and their topography may be closely related to the location of the primary neoplasm.1,2Hematogenous and lymphatic spread are more frequent but direct secondary invasion of the skin due to contiguity may occasionally occur. The condition is generally indicative of advanced neoplasia, and it rarely presents as the first disease manifestation.1,2
Cutaneous metastases from urinary tract tumours are observed in 1.1% of cases, 3.4% are from renal cell carcinomas, and only 0.84% from urothelial carcinomas, which originate in the inner lining of the urinary tract of the ureter, bladder, and urethra.²
CASE REPORT
A 50-year-old male construction worker, who was a severe alcoholic, with 35-year history of tobacco use, was observed at the dermatology outpatient clinic after referral from the surgical clinic. He reported, approximately 8 months prior, the progressive appearance of seven cutaneous asymptomatic nodules, with no associated systemic symptoms.
Cutaneous lesions progressively became painful, for which he used paracetamol and dipyrone, and he also reported epigastric discomfort, dyspnea, hematuria, constipation, and weight loss of 20 kg in 2 months.
During examination, we observed 7 painful tumors with stony consistency measuring from 3 to 8 cm in diameter, localized in the lower left quadrant of the abdomen (2), left hip (1), left axilla (1), frontotemporal region (2) and right inguinal region(1), four of them with ulceration, necrosis, and purulent exudate (2), (Fig. 1).
Histopathology of the skin biopsy revealed infiltration of atypical non-cohesive polygonal epithelioid cells with round vesicular nuclei and apoptotic bodies in the superficial and deep dermis and hypodermis without epidermal involvement.
Coagulation necrosis and widespread angiolymphatic invasion in small vessels of the superficial dermis were also observed (Fig. 2). Immunohistochemistry showed positive immunostaining for cytokeratins 5/6 and 7; p53; p63; p40;
GATA3, and CDX-2 (in rare cells) and negative immunostaining for cytokeratins 20, TTF-1, PAX-8, PSA, and MUC5AC, mammaglobin, estrogen receptors, and CEA, suggesting secondary cutaneous infiltration by a neoplasm of the transitional epithelium of the bladder or urinary tract, excluding metastasis from other primary sites, such as the lungs, colon, pancreas, prostate, breast, and stomach (Fig. 3).
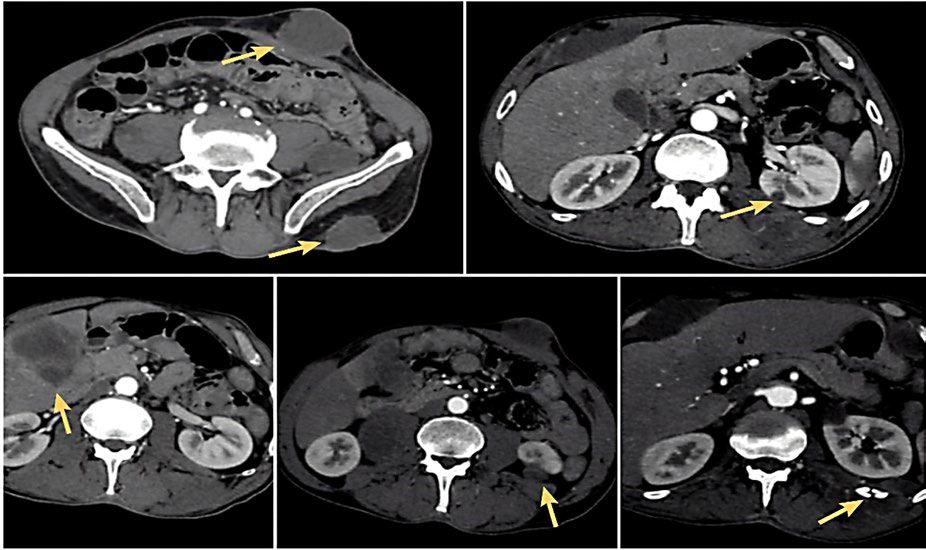
A computed tomography (CT) scan of the abdomen showed multiple solid lesions, namely a lesion located anterior to the rectum and posterior to the seminal vesicles (3.5cm) and an exophytic cortical lesion in the left kidney (3.2 cm), and other lesions on the V segment of the liver (5.4cm), right adrenal gland (3.3 cm), rectus abdominis muscle, and adjacent subcutaneous tissue (Fig. 4).
Considering the diagnosis of cutaneous metastases from a poorly differentiated urothelial carcinoma, possibly originating in the bladder and/or urinary tract, the patient started chemotherapy with carboplatin and paclitaxel but he died within 2 weeks.

Figure 1 Ulcerated tumors in the abdominal region (A), left axilla (B), left frontotemporal region (C), large subcutaneous tumors in the right frontotemporal region (D) and right inguinal region (E).
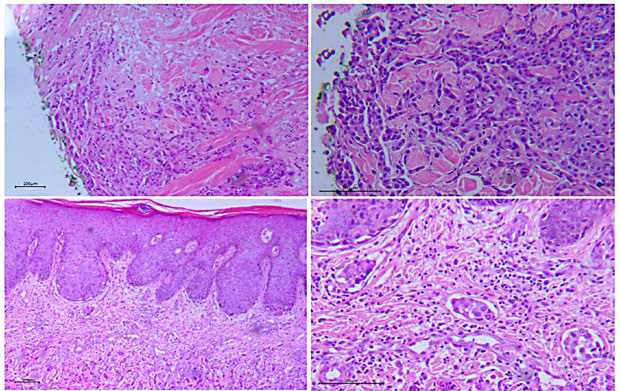
Figure 2 Histopathology of a skin biopsy showing dermal infiltration by polygonal neoplastic cells in A - (40× H&E), with more detail in B - (100×H&E), preservation of the epidermis in C - (40× H&E) and angiolymphatic invasion by nests of neoplastic c ells in D - (100× H&E).
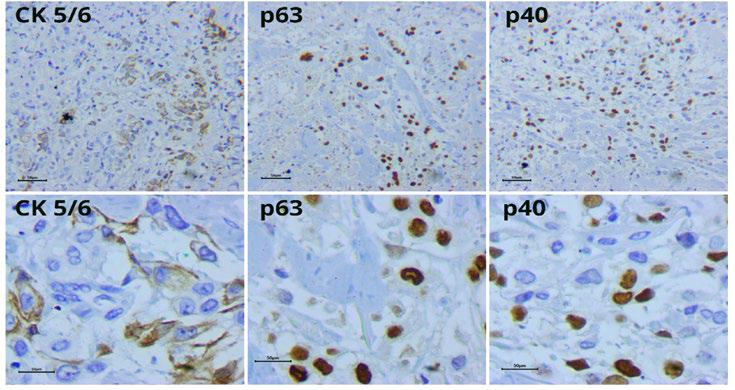
Figure 3 Immunohistochemistry with positive focal immunostaining for CK5/6, p63, and p40 (100× and 400× H&E).
DISCUSSION
Cutaneous metastases generally present as single or multiple nodules and tumors, with stony consistency; they may ulcerate and present a necrotic aspect, as observed in our patient.² Occasionally, they present as erythematous, sclerodermiform or papulonodular lesions.² Diagnosis can be difficult due to similarities with primary cutaneous lesions, such as hemangiomas, keratoacanthomas,3 sarcoidosis, leprosy, boils, sebaceous cysts, and opportunistic infections.4 Histopathology usually shows neoplastic cells that infiltrate the dermis and preserve the epidermis and may invade dermal vessels,5 which is also the pattern of urothelial carcinomas,6 as in the reported case. The immunohistochemistry profile with positivity for cytokeratins 5/6/7 and p63 is concordant with other cases in the literature, but cytokeratin 20 which, along with cytokeratin 7, is positive in 89% of transitional cell bladder cancers,7 was not positive in this case.
Urothelial neoplasms occur mostly in the bladder (90%), are approximately 3 times more frequent in men between the fifth and seventh decade. Main risk factors are tobacco smoke (which is also associated with higher disease spread through the urothelium to adjacent structures, as observed in the present case), occupational exposure to aromatic amines, cyclophosphamide, improper use of paracetamol, chronic irritation secondary to infected nephrolithiasis, and cystitis caused by Schistosoma haematobium.9,10,11
Symptoms related to urothelial neoplasia are scarce, the main one being macroscopic hematuria,2 which became apparent in this case only after cutaneous metastasis. Most patients are diagnosed during routine examination or due to metastatic lesions,12 that are mainly localized in the head, face, neck, trunk, abdomen, suprapubic region or extremities.7 Nevertheless, only approximately 20% of these cutaneous metastases occur at the initial presentation.8 They generally develop late in the evolution of the disease and cutaneous involvement indicates a poor prognosis.
In this case cutaneous lesions were the presenting sign of an urothelial carcinoma but they occurred only after disease dissemination and were, therefore, associated with a very poor prognosis. Recognition of cutaneous metastases can be
important to the diagnosis of internal malignancies, particularly in early stages, when treatment may have a favorable impact on prognosis.

