










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkAngiologia e Cirurgia Vascular
versão impressa ISSN 1646-706X
Angiol Cir Vasc vol.16 no.3 Lisboa set. 2020
ORIGINAL ARTICLE
Pre-operative anemia as a predictive morbidity outcome - A retrospective analysis of a vascular surgery department
Anemia pré-operatória como factor predictor de morbilidade - Análise retrospectiva de um departamento de cirurgia vascular
Carolina Semião1, Clara Nogueira1, Jacinta Campos1,2, Andreia Coelho1,2, Rita Augusto1,2;Nuno Coelho1,2, Evelise Pinto1, João Ribeiro1, João Peixoto1, Alexandra Canedo1,2
1 Serviço de Angiologia e Cirurgia Vascular, Centro Hospitalar de Vila Nova de Gaia/Espinho, Vila Nova de Gaia, Portugal
2 Unidade de Angiologia e Cirurgia Vascular da Faculdade de Medicina da Universidade do Porto, Porto, Portugal
Endereço para correspondência | Dirección para correspondencia | Correspondence
ABSTRACT
Introduction: Anemia is associated with increased adverse outcomes during the early postoperative period because of high physiologic stress and increased cardiac demand. The aim of this study was to assess the relationship between pre-operative anemia and morbi-mortality outcomes in patients undergoing elective carotid endarterectomy (CEA), open aortic repair (OAR) or endovascular aneurysm repair (EVAR) of abdominal aortic aneurysms (AAA) and infrainguinal bypass surgery in chronic limb-threatening ischemia.
Methods: Retrospective analysis of all elective patients between 2016-2018, who underwent: CEA, OAR, EVAR and infrainguinal bypass surgery in chronic limb-threatening ischemia. Emergency procedures and transfusion of more than 4 units of red blood cells (RBC) were excluded. Hemoglobin levels were categorized according to the WHO definition for anemia: severe (< 8 g/dL), moderate (8-10.9 g/dL), mild (11-11.9 g/dL in women and 11-12.9 g/dL in men) and no anemia (e12 g/dL in women and e13 g/dL in men).
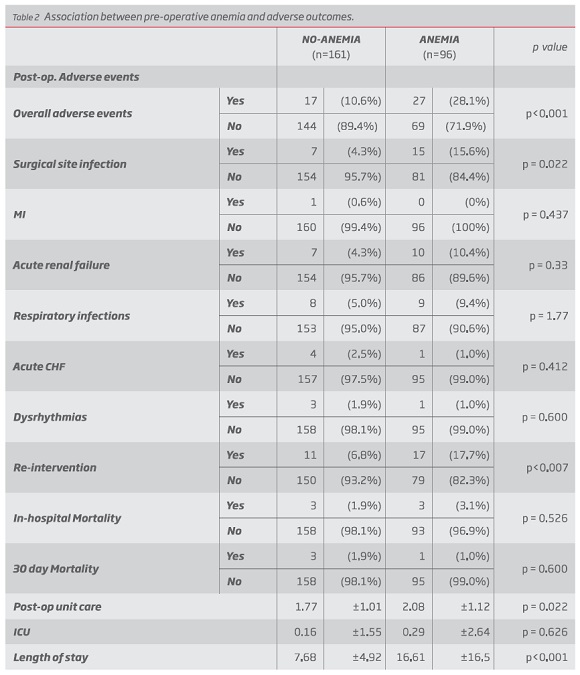
Results: Our study population comprised 257 patients, of which 74 (28%) underwent EVAR, 26 (10.1%) OAR, 67 (26.1%) CEA and 90 (35%) infrainguinal bypass. Pre-operative anemia was identified in 37.4% (n = 96) of the patients. Of those, 67.7% (n = 65) had mild anemia and 32.3% (n = 31) had moderate-severe anemia. Anemic patients have longer length of stay when compared with non-anemic patients (16.61±16.5; 7.68±4.92, respectively) (p = 0.022) and also longer stay in the post-operative care unite in comparison with patients with hemoglobin within the normal range (average 2.08 days ± 1.12; 1.77 days ± 1.01, respectively) (p<0.001). Pre-operative anemia was associated with the need of peri-operative transfusions (p < 0.001), as expected. In-hospital adverse events were influenced by the presence of anemia (p<0.001), namely surgical site infection (p = 0.002) and re-intervention (p<0.007). Patients who received blood transfusion peri-operatively were more prone to adverse outcomes (p<0.001), such as renal disfunction (p = 0.006), respiratory infections (p =0.015), surgical site infection (p = 0.001) and re-intervention (p = 0.001).
Conclusion: Pre-operative anemia evaluation should be incorporated into the preoperative risk assessment. Iron deficiency anemia is the most frequent type of anemia. In these cases, oral or IV iron supplementation pre-operatively is the preferential treatment, and might decrease the need of blood transfusions. Patients with iron deficiency without anemia also have indication to take oral iron supplementation. This situation urges the application of a well-structured protocol to optimize pre-operative hemoglobin, reduce intra-operative blood loss and improve anemic patients’ status in an effort to reach better outcomes.
Keywords: Pre-operative anemia; Iron supplementation; Patient Blood Management; Vascular surgery
RESUMO
Introdução: A anemia está associada a um aumento do número de eventos adversos no período pós-operatório precoce devido ao elevado stress fisiológico e aumento das necessidades cardíacas. O objetivo do presente estudo foi avaliar a relação entre a presença de anemia pré-operatória com os outcomes de morbi-mortalidade em doentes submetidos a cirurgia vascular electiva, nomeadamente endarterectomia carotídea, reparação cirúrgica de aneurisma da aorta abdominal, reparação endovascular de aneurisma da aorta abdominal (EVAR) e bypass infra-inguinal por isquemia crónica.
Métodos: Análise retrospectiva de todos os doentes intervencionados entre 2016 a 2018 a: endarterectomia carotídea, reparação cirúrgica de aneurisma da aorta abdominal, EVAR e bypass infra-inguinal por isquemia crónica. Foram excluídos todos os procedimentos realizados em contexto de urgência e aqueles com necessidade transfusional superior a 4 unidades de glóbulos rubros. Os níveis de hemboglobina foram categorizados de acordo com a definição da OMS para anemia: grave (< 8 g/dL), moderada (8-10,9 g/dL), ligeira (11-11,9 g/dL no sexo feminino; 11-12,9 g/dL no sexo masculino) e ausência de anemia (e12 g/dL no sexo feminino e e13 g/dL no sexo masculino).
Resultados: A população estudada incluiu 257 doentes, 74 (28%) dos quais foram submetidos a EVAR, 26 (10,1%) a reparação cirúrgica de AAA, 67 (26,1%) a endarterectomia carotídea e 90 (35%) a bypass infra-inguinal. A anemia pré-operatória foi identificada em 37,4% (n = 96) dos doentes. Destes, 67,7% (n = 65) apresentavam anemia ligeira e 32,3% (n = 31) tinham uma anemia moderada-grave. Os doentes anémicos apresentam um total de dias de internamento mais prolongado em comparação com aqueles sem anemia (16,61±16,5; 7,68±4,92, respectivamente) (p = 0,022), bem como um internamento mais prolongado na Unidade de Cuidados Pós-Anestésicos comparativamente aos doentes com hemoglobina dentro dos valores normais (2,08 dias ± 1,12; 1,77 dias ± 1,01, respectivamente) (p<0,001). A existência de anemia pré-operatória associou-se com o aumento das necessidades transfusionais peri-operatórias (p<0,001), tal como expectável. A ocorrência de eventos adversos foi influenciada pela presença de anemia (p<0,001), nomeadamente infecção da ferida operatória (p = 0,002) e re-intervenção (p<0,007). Os doentes com necessidade de suporte transfusional peri-operatório tiveram uma tendência para a ocorrência de um maior número de eventos adversos (p<0,001), tais como lesão renal aguda (p = 0,006), infecções do tracto respiratório (p =0,015), infecção da ferida operatória (p = 0,001) e re-intervenção (p = 0,001).
Conclusão: O estudo da anemia deverá ser incorporado na avaliação do risco pré-operatório. A anemia por deficiência de ferro é o tipo mais comum de anemia. Nesta situação, a suplementação com ferro oral ou endovenoso no período pré-operatório é o tratamento preferencial, que poderá inclusive diminuir as necessidades transfusionais. Os doentes que apresentem ferropenia sem anemia, também têm indicação formal para iniciar suplementação de ferro. Estes resultados corroboram a necessidade de implementação de um programa bem estruturado, que vise a optimização da hemoglobina e do ferro no período pré-operatório, redução das perdas de sangue intra-operatórias e melhoria do status do doente anémico com o objetivo comum de atingir outcomes mais favoráveis.
Palavras-chave: Anemia pré-operatória; Suplementação com ferro oral e endovenoso; Patient blood management; Cirurgia vascular
Introduction
Anemia was previously perceived as an “innocent bystander,” accepted as part of aging and associated with chronic illnesses. It has become so frequent in our daily practice, that doctors might have faced it as “normal”.(4) But what is actually anemia? According to World Health Organization (5), anemia is a condition in which the number of red blood cells (RBC) is insufficient to meet the body’s physiologic needs. It is categorized according to the hemoglobin (Hb) levels as severe (Hb < 8 g/dL), moderate (Hb 8-10.9 g/dL) and mild (Hb 11-11.9 g/dL in women and 11-12.9 g/dL in men). Absence of anemia occurs when Hb e12 g/dL in women and e13 g/dL in men. Iron deficiency is the most frequent cause of anemia and its correction is often neglected.(6)
Recently, anemia has been acknowledged as a predictor of higher mortality and increased post-operative adverse outcomes, namely acute renal dysfunction, myocardial infarction, stroke, surgical site infection, and others.(7) International organizations developed the Patient Blood Management Program (PBM) to overcome the issues associated with pre-operative anemia and its potentially fatal consequences.(8)
Thus, our aim was to assess the relationship between pre-operative anemia and morbi-mortality outcomes in patients undergoing elective carotid endarterectomy (CEA), open aortic repair (OAR) or endovascular aneurysm repair (EVAR) of abdominal aortic aneurysms (AAA) and infrainguinal bypass surgery in chronic limb-threatening ischemia.
Methods
This retrospective analysis included every patients undergoing the following elective procedures (n = 257): 67 (26.1%) carotid endarterectomy (CEA), 26 (10.1%) open aortic repair (OAR) or 74 (28%) endovascular aneurysm repair (EVAR) of abdominal aortic aneurysms (AAA) and 90 (35%) infrainguinal bypass surgery in chronic limb-threatening ischemia, between 2016 and 2018. Emergency procedures and patients that required transfusion of more than 4 units of RBC preoperatively or intraoperatively were excluded to avoid inclusion of patients with blood loss anemia.
Hemoglobin levels were categorized according to the WHO definition for anemia. The pre-operative hemoglobin was defined as the last measurement obtained before surgery. Patients were older than 18 years and abled to sign or delegate a representative. Patient's demographics, preoperative laboratory data, perioperative transfusions and clinical outcomes were assessed.
Patients were classified as smokers (current or ex <1 year), former smokers (quit >1 year), or never smokers. Hypertension and diabetes were considered if previously diagnosed by a physician or under treatment. Hyperlipidemia was defined by medical history or when low-density lipoprotein (LDL) cholesterol >200 mg/dL. Chronic kidney disease (CKD) was considered when the glomerular filtration rate (GFR) was <60 mL/min. Coronary artery disease (CAD), including history of angina, myocardial infarction, was reviewed using hospital or primary care records. Congestive heart failure (CHF) was defined according to the most recent ACC/AHA guidelines as the clinical diagnosis of heart failure with ejection fraction d40%. Peripheral arterial disease was classified as a ankle-brachial index < 0.90 or > 1.30 (if diabetic), and was reviewed using hospital records. Chronic obstructive pulmonary disease (COPD) was defined as a forced expiratory volume in 1 second <70% or medication use.
Primary outcomes included mortality and morbidity. Specific morbidities included surgical site infection, defined as a documented wound infection requiring antibiotics; myocardial infarction (MI) was diagnosed when e2 of the following were present: increased cardiac enzyme levels (elevation of troponins levels at least 1 point above 99 percentile of reference value), development of typical electrocardiographic changes and typical symptoms of angina pectoris; pneumonia, defined as an infiltrate on the chest radiograph, hypoxemia, elevated leukocyte count, and productive sputum; acute renal failure AKI was diagnosed by an absolute increase in serum creatinine (at least 0.3 mg/dL) within 48 hours, or by a 50% increase in serum creatinine from baseline within 7 days, or a urine volume of less than 0.5 mL/kg/h for at least 6 hours; and dysrhythmias (atrial fibrillation and atrial flutter).
Statistical analysis
Statistical analysis was performed using the SPSS statistical software package 25.0 (IBM, New York, NY, USA). Continuous, normally distributed variables were expressed as mean ± standard deviation and analyzed using a t-test. Categorical variables were expressed as frequencies and analyzed using the chi-square test or the Fisher's exact test, as appropriate. A p value of 0.05 was considered to be statistically significant.
Unadjusted comparisons between patients who received perioperative transfusion and patients who did not receive perioperative transfusion were performed by the Fisher exact test for categorical variables and the two-tailed t-test for continuous variables (log transformation was applied to variables with skewed distribution). The adverse outcomes were compared between no transfusion and transfusion by Fisher exact test.
Results
Patient characteristics and outcomes
Of 257 patients, 218 (85.8%) were male and the mean age was 70.07 (standard deviation 9.3). The demographic characteristics of the study group are summarized in Table 1.

Pre-operative anemia was associated with the need of peri-operative transfusion (p < 0.001), as expected. When comparing all the post-operative adverse outcomes together, we observed that overall adverse events were associated with pre-operative anemia (p<0.001). Individually, renal disfunction (p = 0.043), surgical site infection (p = 0.002) and re-intervention (p = 0.012) were more frequent in anemic patients with statistical significance. (Table 2.)
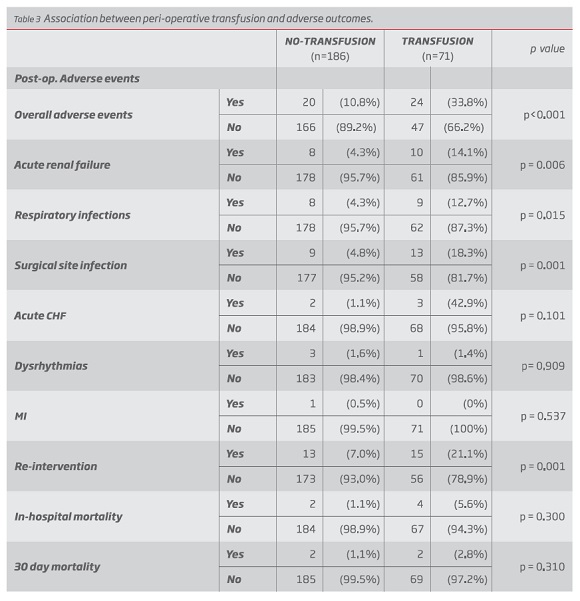
Patients who received blood transfusion peri-operatively were more prone to adverse outcomes (p < 0.001), such as renal disfunction (p = 0.011), pneumonia (p =0.023), surgical site infection (p = 0.001), re-intervention (p = 0.003), in-hospital mortality (p = 0.05) and overall adverse outcomes (p<0.001) (Table 3.)
Discussion
Vascular pathology is a systemic process, therefore vascular patients are a high-risk cohort with multiple comorbidities.
Major vascular surgery procedures are undoubtfully associated with blood loss, even in elective, well-controlled environment. In some cases, blood transfusions are unnecessary and harmful for patients. Therefore, it is important to minimize the chances of jeopardizing the patient’s outcome.
In this study, more than one third of patients were diagnosed with anemia pre-operatively. Reviewing vascular literature, a similar frequency of anemia can be found, and its prevalence can be as high as 50%.(9) These patients were more prone to the overall adverse outcomes in the post-operative period, and we also found an association between pre-operative anemia and surgical site infections. We hypothesized there was no statistical significance regarding other adverse outcomes because of the low number of patients included in the study. Some studies have shown that anemic patients were more likely to be older, with lower body mass index and reduced glomerular filtration rates. All these findings raise the question of whether pre-operative hemoglobin level is reflecting some sort of frailty, poor nutritional status, or underlying chronic disease among patients suffering from CLI, all of them known risk factors influencing life expectancy.
We were surprised to find that treating anemia with transfusion was associated with increased morbidity. In our population, there was a clear association between transfusion and adverse outcomes, such as acute renal dysfunction, respiratory infections, surgical site infections and overall adverse outcomes as well. Also, patients receiving peri-operative transfusions, not only had a greater length of stay, but also an association with in-hospital mortality. (10) Supporting our findings, in vascular literature perioperative transfusion is independently associated with potentially fatal postoperative outcomes such as pneumonia and sepsis, transfusion-associated lung injury, cardiac events, surgical site infections, myocardial infarction, TIA/stroke and higher postoperative 30-day mortality. It is described that blood transfusions have an immunomodulatory effect, directly suppressing the immune system, which may play a role in the increased number of infections observed in the transfused patients.(11, 12) In addition to that, blood age may make difference in outcomes, as outlined by studies in cardiac surgery patients, in which transfusion of older blood (median of 20 days) was associated with increased morbidity and mortality compared with transfusion of “fresher” blood (median, 11 days).(7)
Considering the high prevalence of anemia and the wide use of blood transfusions pre-operatively with poor outcomes, several international organizations created the Patient Blood Management program. PBM aims to reduce the need for blood transfusions preemptively to improve patient safety and outcome, and consists of three pillars: treatment of preoperative anemia, reduction of perioperative blood loss and optimization of anemia tolerance.(13) In addition, the use of restrictive, evidence-based, and patient-centered transfusion triggers is an integral part of PBM. The pioneer countries implementing PBM, have already reached remarkable results that should encourage us to embrace this paradigm shift. According to a study driven by one of the founders of PBM, Dr. Spahn, it has proved to progressively reduce the adjusted in-hospital mortality (28%), hospital length of stay (15%), hospital-acquired infections (21%), and myocardial infarction or stroke (31%). Regarding transfusions of red blood cells (RBCs), there was an impressive reduction of 41%.(8) The most outstanding achievement was the decrease in the percentage of elective patients admitted with anemia from 20.8% to 14.4%. Undoubtfully, these results can only be attributed to a consistent identification and treatment of existing anemia and iron deficiency in the weeks before hospitalization.
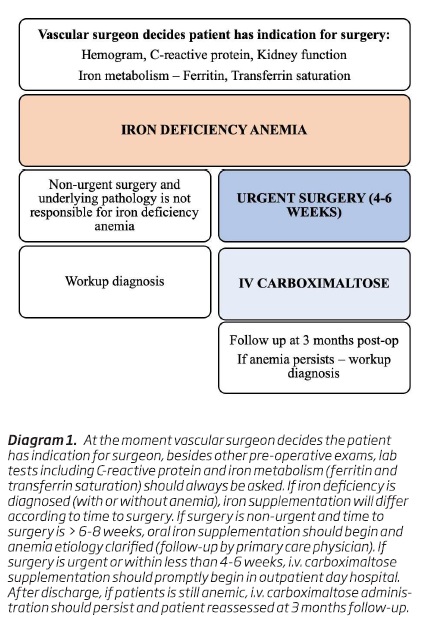
Since iron deficiency is the most frequent cause of anemia, it’s supplementation should be addresses. Currently, oral/intra-venous (i.v.) iron supplementation is the treatment of choice in iron deficiency anemia.(14) Iron deficiency should be identified in lab test regarding iron metabolism (ferritin <30 ng/ml and/or transferrin saturation <20%) thoroughly treated. Iron supplementation therapy offers symptomatic improvement by the 3rd day, with the maximum hematopoietic response being observed by the 3rd week of treatment. Hemoglobin usually increases within 2-3 weeks of starting iron supplementation.(14) The diagnosis and treatment of anemia and iron deficiency should begin as early as possible in the peri-operative period, and ideally as soon as the decision to undertake surgery is made.
Oral iron replacement should be targeted to patients with iron deficiency with or without anemia whose surgery is scheduled 6-8 weeks after diagnosis, preferably by the primary care physician.(13) Daily (100-200 mg) treatment with oral iron and nutritional advice should be initiated immediately in patients with iron deficiency and no contra-indications. Lab tests should be repeated to ensure treatment is being successful, and after 4 weeks there should be an increase of 1 g/dL of hemoglobin. After Hb stabilization, the patient should continue supplementation during 4-6 months until iron stores are replaced (ferritin > 50 ng/ml, ST e 30%). The primary reason for failure of iron therapy is poor compliance, often related to the frequent gastrointestinal side effects of oral iron. Sufficient data exist to support intravenous iron as efficacious and safe. Intravenous iron (carboximaltose) should be used as front-line therapy in patients who do not respond to oral iron or are not able to tolerate it, or if surgery is planned for < 6 weeks after the diagnosis of iron deficiency. Anytime before surgery until the patient is in the operating room is eligible for i.v. iron supplementation, although if it is administered more than 10 days before surgery it will increase hemoglobin and accelerate the maturation of erythroid cells. Carboximaltose should be administered intravenously by infusion over at least 15 minutes and up to 750 mg can be delivered in a single dose. Each dose should be separated by at least 7 days for a cumulative dose of 1,500 mg.
If the patient is discharged and anemia persists, another i.v. iron supplementation should be administered before discharge and the patient should have a hematology follow-up appointment at 3 months. Besides that, a workup diagnosis with the primary care physician has to be performed to exclude other etiologies.
A systematic review demonstrated that patients receiving i.v. iron supplementation recover faster than others. Although anaphylaxis is a potential side-effect, it is rare with the most recent formulas of i.v. iron, but still it’s administration should be under medical supervision and it requires an informed consent. It is important to keep follow-up after the patient is discharge and anemia etiology should always as possible be clarified.
Erythropoietin, with or without iron, has been used to treat non-iron deficiency anaemia and to increase red cell mass in patients who refuse blood transfusions or who are at high risk of postoperative anaemia, such as patients with renal failure. Administration of EPO and oral iron in mildly or non-anaemic patients has reduced the perioperative transfusion requirements in patients treated with EPO more than in controls. Its theoretical thrombotic risk does not seem to be increase with EPO supplementation, and therefore it can be performed in vascular patients.
Blood transfusion is reserved for symptomatic patients requiring emergent hemoglobin increased and cardiovascular instability, but is not routinely recommended in anemic patients pre-operatively. Erythropoietin and iron supplementation should be considered for pre-operative optimization in patients with anemia of other causes than iron deficiency.
These findings led to the introduction of a PBM protocol in our department. We suggest the incorporation of pre-operative anemia evaluation in the preoperative risk assessment. Iron supplementation before surgery has showed to improve patients’ symptoms, quality of life and well-being, besides the reduction of blood transfusions. This could only be possible thanks to a tight team work between vascular surgeons, nurses, hematologists, anesthesiologists, nutritionists and clinical pathologists working together to achieve better outcomes for the patients.
Conclusion
These findings strongly suggest the need for a prospective randomized controlled trials but in the meanwhile we should adopt measures to improve the patients’ pre-operative status in order to reach better results after surgery. Pre-operative anemia evaluation should be incorporated into the preoperative risk assessment. Iron deficiency anemia is the most frequent type of anemia. In these cases, oral or IV iron supplementation pre-operatively is the preferential treatment, and might decrease the need of blood transfusions. Patient Blood Management has proven to be safe and efficacious in improving patient outcome by optimizing the patient pre-operatively. For this reason we, as physicians, should gather our efforts in a way to convert these measures into Patient Best Management.
REFERENCES
1. Simmons, J.D., et al., Elevated levels of plasma mitochondrial DNA DAMPs are linked to clinical outcome in severely injured human subjects. Ann Surg, 2013. 258(4): p. 591-6; discussion 596-8. [ Links ]
2. McMillan, M.T., et al., Risk-adjusted Outcomes of Clinically Relevant Pancreatic Fistula Following Pancreatoduodenectomy: A Model for Performance Evaluation. Ann Surg, 2016. 264(2): p. 344-52. [ Links ]
3. DeMatteo, R.P., et al., Long-term results of adjuvant imatinib mesylate in localized, high-risk, primary gastrointestinal stromal tumor: ACOSOG Z9000 (Alliance) intergroup phase 2 trial. Ann Surg, 2013. 258(3): p. 422-9. [ Links ]
4. Dakour-Aridi, H., et al., Anemia and postoperative outcomes after open and endovascular repair of intact abdominal aortic aneurysms. J Vasc Surg, 2019. 69(3): p. 738-751 e2. [ Links ]
5. Cotton, B.A., et al., A randomized controlled pilot trial of modified whole blood versus component therapy in severely injured patients requiring large volume transfusions. Ann Surg, 2013. 258(4): p. 527-32; discussion 532-3. [ Links ]
6. Nutritional anaemias. Report of a WHO scientific group. World Health Organ Tech Rep Ser, 1968. 405: p. 5-37. [ Links ]
7. Obi, A.T., et al., The association of perioperative transfusion with 30-day morbidity and mortality in patients undergoing major vascular surgery. J Vasc Surg, 2015. 61(4): p. 1000-9 e1. [ Links ]
8. Leahy, M.F., et al., A pragmatic approach to embedding patient blood management in a tertiary hospital. Transfusion, 2014. 54(4): p. 1133-45. [ Links ]
9. Gupta, P.K., et al., Preoperative anemia is an independent predictor of postoperative mortality and adverse cardiac events in elderly patients undergoing elective vascular operations. Ann Surg, 2013. 258(6): p. 1096-102. [ Links ]
10. Trentino, K.M., et al., Associations of nadir haemoglobin level and red blood cell transfusion with mortality and length of stay in surgical specialties: a retrospective cohort study. Anaesthesia, 2019. 74(6): p. 726-734. [ Links ]
11. Bernard, A.C., et al., Intraoperative transfusion of 1 U to 2 U packed red blood cells is associated with increased 30-day mortality, surgical-site infection, pneumonia, and sepsis in general surgery patients. J Am Coll Surg, 2009. 208(5): p. 931-7, 937 e1-2; discussion 938-9. [ Links ]
12. O'Keeffe, S.D., et al., Blood transfusion is associated with increased morbidity and mortality after lower extremity revascularization. J Vasc Surg, 2010. 51(3): p. 616-21, 621 e1-3.
13. Spahn, D.R., Patient Blood Management: Success and Potential in the Future. Ann Surg, 2016. 264(2): p. 212-3. [ Links ]
14. Task Force on Patient Blood Management for Adult Cardiac Surgery of the European Association for Cardio-Thoracic, S., et al., 2017 EACTS/EACTA Guidelines on patient blood management for adult cardiac surgery. J Cardiothorac Vasc Anesth, 2018. 32(1): p. 88-120. [ Links ]
Endereço para correspondência | Dirección para correspondencia | Correspondence
Correio eletrónico: anasemiao1@gmail.com (A. Semião).
Recebido a 15 de junho de 2019. Aceite a 14 de outubro de 2020.

