










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkAngiologia e Cirurgia Vascular
versão impressa ISSN 1646-706X
Angiol Cir Vasc vol.14 no.2 Lisboa jun. 2018
CASO CLÍNICO
Ischaemia in the neonate–case report
Isquémia no recém-nascido — relato de um caso
Roger Rodrigues1, Gabriel Anacleto1, Carolina Mendes1, Juliana Varino1, André Marinho1, Bárbara Pereira1, Mário Moreira1, Mafalda Correia1, Pedro Lima1, Óscar Gonçalves1
1 Serviço de Angiologia e Cirurgia Vascular, Centro Hospitalar e Universitário de Coimbra
Autor para correspondência
ABSTRACT
Introduction: Peripheral ischaemia and gangrene in a neonate is rare,with fewer than a hundred cases reported in the literature. Neonatal limb ischaemia present considerable challenges in diagnosis and management. The published literature is limited to case reports and case series and there are no large trials comparing different therapies.
Objectives: The authors describe the case of a 4-day newborn transferred to the Pediatric Hospital for a gangrene of the lower limb.
Results: In this case the member was not salvageable. Treatment with Heparin was performed which is usually effective in cases of neonatal limb ischaemia, but in this case the evolution was not favorable.
The diagnosis was late and an amputation of the leg was performed. A multidisciplinary team of surgeons, paediatricians,occupational therapists, physiotherapists, working together provided the best support network and best treatment for this child.
Conclusions: Neonatal limb ischaemia is uncommon, but can have devastating consequences on the patient. Successful management is dependent on early recognition, rapid clinical assessment and appropriate therapy.
Initial supportive therapy may be appropriate with aggressive interventional treatment reserved for selective cases.
Interventional treatment includes thrombolysis using a tissue plasminogen activator which can be catheter directed or systemic, and surgical thrombectomy, particularly if larger vessels such as the abdominal aorta are involved.
Strategies for management are still evolving, and there is only a limited pooled experience available for review in the published literature.
Keywords: Gangrene, Lower Extremity, Neonate
RESUMO
A Isquémia aguda de um membro e gangrena no recém-nascido são uma condição rara e desafiadora.
Em crianças, o comprometimento vascular que afeta os membros no período pós-natal pode ser resultante de distúrbios da coagulação, sépsis, diabetes gestacional ou lesões iatrogênicas.
A abordagem clínica desses pacientes pode variar desde, terapia conservadora até a opções mais invasivas como trombólise e a tromboembolectomia cirúrgica em uma população selecionada.
Descrevemos o caso de um recém-nascido com uma gangrena do membro inferior.
Palavras-chave: Gangrena; Recém-nascido; trombose arterial
INTRODUCTION
Peripheral ischaemia and gangrene in a neonate is rare, with fewer than a hundred cases reported in the literature. Its aetiology is obscure, and, in many cases, no etiological factor can be found. Approximately 25% of neonatal gangrene cases have been reported to occur in infants of diabetic mothers.(1) This is usually seen in insulin dependent and poorly controlled diabetic mothers. Neonatal limb ischaemia present considerable challenges in diagnosis and management. The published literature is limited to case reports and case series and there are no large trials comparing different therapies.
CASE REPORT
A male infant, weighing 5.1 kg, was born to a 26 years old woman with gestational diabetes, at 37 weeks of gestation. It was a cesarean delivery and he cried at birth. There were no cardiotocographic abnormalities in labour. The umbilical cord was not twisted around the infant's body or limbs.
There were no placental infarcts.
12 hours after birth the pediatricians found that the left leg was pale and colder (Fig.1).

They maintained surveillance and 24 hours after delivery verified the appearance of erythrocyanotic patches (Fig.2).

On the third day of life and due to clinical worsening, he was transferred to the Pediatric Hospital (Fig.3).

The vascular surgery team was contacted, at that moment the child was apparently in pain and agitated. Both axillary and femoral pulses were palpable.
The leg was cold, with erythrocytosis, and with multiple skin blisters. It had no signs of infection and had no hyperthermia.
Echocardiogram was normal. A consultation by the paediatric cardiology team excluded any structural cardiac abnormality. An Doppler ultrasound was performed and revealed occlusion of the right superficial femoral artery.
The infant's Leukocytes was 18, 8 x 10 9/L and platelet count was 31 x 10 9L.
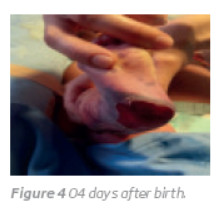
Treatment with Heparin and antibiotics were prescribed. It was apparent that the involved part of the limb was not salvageable (Fig.4).
On the seventh day of life, the infant underwent amputation of the right leg and made an uneventful recovery.
DISCUSSION
Arterial occlusion in the newborn is a rare and challenging condition.
Various conditions have been implicated as a cause for the ischaemic episode. Thromboembolism may be a cause and may be associated with maternal diabetes.(2)
The first published report of peripheral gangrene in an infant of a diabetic mother was by Valderrama et al. in 1972. The reason for this association is not exactly known but coagulation abnormalities have been proposed as the likely cause for arterial as well as venous thrombosis. Venous thrombosis and thromboembolism are well established complications in infants of diabetic mothers.(3)
Decreased production of prostacyclin and low levels of antiplasmin has been shown in infants of diabetic mothers.(4)
Other predisposing factors include prematurity hyper-coagulable state,umbilical artery cannulation, intravenous hyperosmolar infusions, sepsis, thermal abnormality, and in utero arterial thrombosis.(5)
Neonatal gangrene can affect either upper limbs or lower limbs. Rarely, either upper limbs or both lower limbs can be affected. The extent of the gangrene is also variable ranging from one or more toes or fingers to part of the limb and rarely the whole limb may be involved.(6) In our patient, the right leg was gangrenous suggesting thrombosis at the level of the superficial femoral artery.
The treatment of ischaemic complications depends on the anatomical site and mechanism of the ischaemia as well as on the general health and physiological state of the patient. Thrombolysis is the preferred initial management, especially if the patient is extremely unwell. A combination of a thrombolytic agent with an anticoagulant was recommended by Arshad and McCarthy in neonates with limb thrombosis and complete clot lysis was reported in 75% of cases.(7) However, information regarding its use in childhood and infancy is limited and most reports group arterial and venous thrombosis in a diverse age range together. Given the rarity of acute limb ischemia in pediatric patients, physicians and surgeons caring for those patients are usually guided by consensus guidelines that mostly extrapolate from the adult literature.(8)
Operative management should be reserved for cases where medical management has failed or if the risk of bleeding from thrombolysis is unacceptably high, for example, recent cardiovascular surgery or cerebral haemorrhage. Operative treatment may be technically challenging due to the size of the vessels involved, and microsurgical vascular techniques can be a useful adjunct, particularly in extremely low-birth-weight neonates.(9)(10)
Stavorovsky et al treated successfully a seven day old dehydrated male infant with acute ischemia of the leg due to acute thrombotic occlusion of an external iliac, common and superficial femoral, and popliteal arteries with early thrombectomy and arterioplasty.(11)
In this case diagnosis was late and an amputation of the leg was performed.
Amputation should be delayed for as long as possible since the eventual line of demarcation may be some way distal to the original line of ischaemia.
It is also important to differentiate between dry and wet gangrene.
Wet gangrene is most likely the result of venous thrombosis and these patients are more likely to develop superadded infection.(6)
Amputation should be undertaken with full consideration given to future prosthetic limb application and prevention of joint contracture. If possible, the procedure should be carried out by a surgical team experienced in paediatric amputation.(9)
In children with idiopathic arterial thrombosis, there would be a potential for a hypercoagulable state to have an effect on long-term management, and therefore, testing might be an appropriate consideration(8)
A multidisciplinary team of surgeons, paediatricians, occupational therapists, physiotherapists, working together provided the best support network and best treatment for this child.
CONCLUSIONS
Neonatal limb ischaemia is uncommon but can have devastating consequences on the patient. Successful management dependents on early recognition and diagnosis, rapid clinical assessment and appropriate therapy.
Initial supportive therapy may be appropriate with aggressive interventional treatment reserved for selective cases.
Supportive treatment includes adequate intravenous hydration and antibiotics if infection is suspected.
Interventional treatment includes thrombolysis using a tissue plasminogen activator which can be catheter directed or systemic, and surgical thrombectomy, particularly if larger vessels such as the abdominal aorta are involved.
Strategies for management are still evolving, and there is only a limited pooled experience available for review in the published literature.
REFERENCES
1. Moazzam A, Riaz M, Brennen M. Neonatal gangrene in an extremity of an infant of a diabetic mother. BJOG. 2003 Jan; 110:74-6 [ Links ]
2. Long DK, Lorant D. Multiple arterial thrombi and in utero leg gangrene in an infant of a diabetic mother. J Perinatol 2002; 22: 424-427 [ Links ]
3. Valderrama E, Gribetz I, Strauss L. Peripheral gangrene in a newborn infant associated with renal and adrenal vein thrombosis. J Paediatr 1972 ;80: 101–103 [ Links ]
4. Stuart MJ, Sunderji SG, Allen JB. Decreased prostacyclin production in the infant of the diabetic mother. J Lab Clin Med 1981; 98: 412–416 [ Links ]
5. Vasquez P, Burd A, Mehta R, et al. Resolution of peripheral artery catheter-induced ischemic injury following prolonged treatment with topical nitroglycerin in a newborn: a case report. J Perinatol 2003;23(4):348e50. [ Links ]
6. Al-Salem A, Naga M, et al. Neonatal gangrene of the extremity: A report of three cases and review of the literature. Journal of Pediatric Surgical Specialties 8.4-2014 [ Links ]
7. Arshad A, McCarthy MJ. Management of limb ischaemia in the neonate and infant. Euro J Vascular Endovascular Surg 2009; 38:61-5. [ Links ]
8. Kayssi, Ahmed, Shaikh F, Roche-Nagle G, et al. "Management of acute limb ischemia in the pediatric population." Journal of vascular surgery 60.1 (2014): 106-110 [ Links ]
9. Friedman J, Fabre J, Netscher D, et al. Treatment of acute neonatal vascular injuries e the utility of multiple interventions.J Paediatr Surg 1999;34(6):940e5. [ Links ]
10. Theile RJ, Coombs CJ. Microvascular and thrombolytic revascularization of an arm in a 32-week gestation neonate: case report and review of the literature. J Reconstr Microsurg 1996;12(2):539e42 [ Links ]
11. Stavorovsky M, Iellin A, Spirer Z. Acute ischemia of the limb in a newborn treated successfully by thrombectomy. Am J Surg. 1975 Mar; 129:337-40. [ Links ]
Correio eletrónico: roger.cc@hotmail.com (R. Rodrigues).
Recebido a 14 de junho de 2017
Aceite a 24 de maio de 2018

