










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkAngiologia e Cirurgia Vascular
versão impressa ISSN 1646-706X
Angiol Cir Vasc vol.14 no.2 Lisboa jun. 2018
ARTIGO ORIGINAL
Acute lower limb ischemia: 7 years of thromboembolectomies in the elderly
Isquémia aguda de membro inferior: 7 anos de tromboembolectomias em doentes com idade avançada
Mário Moreira1, Pedro Lima1, Mafalda Correia1, Bárbara Pereira1, Roger Rodrigues1, André Marinho1, Carolina Mendes1, Joana Moreira1, Óscar Gonçalves1
1Serviço de Angiologia e Cirurgia Vascular, Centro Hospitalar e Universitário de Coimbra
Autor para correspondência
ABSTRACT
Introduction: Acute lower limb ischemia (ALLI) is a common emergency in Vascular Surgery, with significant morbidity and mortality. Despite other therapeutic options, thromboembolectomy is still a valid option. The aim of this study is to assess the safety and efficacy of this surgical option in the treatment of ALLI, in elderly patients.
Methods: Retrospective, single center study covering the period between January 2010 and December 2016, including all patients at least 80 years old suffering with ALLI, treated by thromboembolectomy. Exclusion criteria were bilateral ALLI, previous revascularization procedures and additional revascularization procedures in the index event. Thirty day major amputation and mortality were the analyzed outcomes.
Results: We identified 254 patients. Thirty day postoperative major amputation rate was 9.4% (n=24) and mortality rate was 5.9% (n=15). Predictors of 30-day major amputation include prolonged ischemia time and increased ischemia severity. Previous diagnosis of arrhythmia is associated with lower amputation risk. No association between the studied covariates and mortality were obtained.
Discussion: Our study show ischemia time as leading factor determining limb salvage, emphasizing the importance of health professionals' awareness for this condition. Regarding perioperative mortality, we did not find significant association among studied covariates; this can be explained by small number of deaths, what can hinder statistical analyzes.
Conclusion: Thromboembolectomy is a valid option in ALLI treatment, even for elderly patients with multiple comorbidities. The difference between arrhythmia prevalence and patients taking anticoagulants expose a possible weakness in the management of these patients.
Keywords: Limb ischemia; acute; thromboembolectomy; elderly.
RESUMO
Introdução: Isquémia aguda de membro inferior é uma emergência frequente em Cirurgia Vascular, acarretando morbi-mortalidade significativa. Apesar de outras opções terapêuticas, a tromboembolectomia mantém-se uma opção válida. Pretendemos analisar a segurança e eficácia desta técnica, em doentes com idade avançada.
Métodos: Estudo retrospectivo, unicêntrico, incluindo os doentes com pelo menos 80 anos, admitidos por isquémia aguda de membro inferior, entre Janeiro de 2010 e Dezembro de 2016 e tratados através de tromboembolectomia. Excluídos doentes com isquémia bilateral, procedimentos prévios de revascularização e necessidade de outros procedimentos de revascularização no evento avaliado. Avaliamos a amputação major e a mortalidade ocorridas até ao 30º dia de pós-operatório.
Resultados: Identificamos 254 doentes. A taxa de amputação major foi 9.4% (n=24) e a taxa de mortalidade foi 5.9% (n=15). Tempo de isquémia prolongado e maior gravidade da isquémia estão associados a maior taxa de amputação. Diagnóstico prévio de arritmia associado a menor risco de amputação. Não observamos relações entre a mortalidade e as variáveis estudadas.
Discussão: Tempo de isquémia é o principal factor a determinar a viabilidade do membro, enfatizando a importância da consciencialização dos profissionais de saúde para esta patologia. Não obtivemos relação entre as variáveis estudadas e a mortalidade, mas a reduzida mortalidade pode ter impedido a análise estatística.
Conclusão: A tromboembolectomia é uma opção válida no tratamento da isquémia aguda do membro inferior, mesmo em doentes com idade avançada. A diferença entre a prevalência de arritmia e o número de doentes anticoagulados evidencia uma possível debilidade na abordagem destes.
Palavras-chave: isquemia de membro; agudo; tromboembolectomia; idosos
INTRODUCTION
Acute lower limb ischemia (ALLI), a common emergency in Vascular Surgery, results from the abrupt cessation of limb perfusion, resulting in a potential threat to the viability of the extremity. The classical description of patients is represented by the “six P´s”: pain, pallor, paralysis, pulse deficit, paresthesia and poikilothermia. Embolism and thrombosis are the most common causes. Embolism decreased in the last years, possibly related to a lower prevalence of cardiac valvular disease and better approach in the diagnosis and management of atrial fibrillation. On the other hand, thrombosis became more frequent paralleling atherosclerosis and aging population.
Rutherford classification1 for acute limb ischemia has been used to categorize disease severity and is useful in therapeutic approach and prognosis. The management is highly variable and depends on several factors, including the severity (Rutherford classification), the occlusion level, surgeon comfort with operative and interventional techniques, and availability of hospital endovascular capabilities and supplies. Paramount to successful treatment are prompt recognition and diagnosis, followed by rapid restoration of blood flow to the ischemic limb, to minimize risk of limb loss and reperfusion-related local and remote organ injury.
There are basically three management options( 1):
1) Medical treatment: anticoagulation
2) Surgical thromboembolectomy and correction of any underlying lesions
3) Minimally invasive/percutaneous approach.
Surgery and percutaneous approach yield similar results regarding mortality and limb salvage whereby none can be considered the standard approach.(2)(3)
Frequently, more than one management option is needed.
ALLI results in substantial morbidity and mortality. Even using newest endovascular approaches, significant mortality (7-20%) and 30-day amputation (10-25%) occurs.(4-6) This risk seems to be higher in elderly patients.
First successful thromboembolectomy is attributed to Georges Labey in 1911. The catheter currently used was designed years later by Fogarty. Despite other therapeutic options, thromboembolectomy is still a valid option. The aim of this study is to assess the safety and efficacy of this surgical option in the treatment of ALLI, in elderly patients.
METHODS
This is a retrospective, single center study covering the period between January 2010 and December 2016, including all patients at least 80 years old suffering with ALLI, treated by thromboembolectomy. Exclusion criteria were bilateral ALLI, previous revascularization procedures and additional revascularization procedures in the index event. Patient demographics (age, sex) and clinical characteristics (ischemia time: <12h, 12-24h, >24h; ischemia severity: Rutherford classification) were recorded, as well as comorbidities (diabetes, arrhythmia and anticoagulation drugs). Thirty day major amputation and mortality were the analyzed outcomes.
Surgical treatment: Heparin anticoagulation was usually started at the diagnosis and revascularization attempt with Fogarty catheter thromboembolectomy after common femoral artery exposure under local anesthesia and conscious sedation in majority of cases; sometimes approach to superficial femoral or distal popliteal arteries was used.
RESULTS
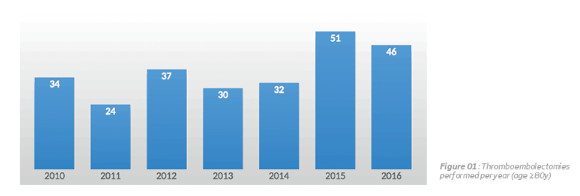
We identified 254 patients. Figure 1 show annual event distribution. Tabel 1 summarizes patient demographics and clinical characteristics
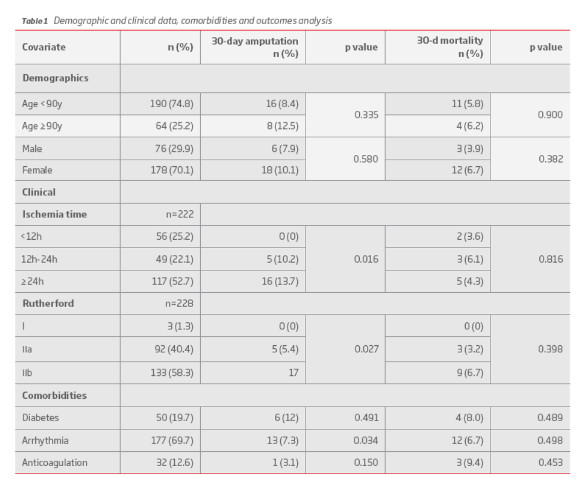
The patients were an average age of 86 (80-101), 74.8% were younger than 90 years old and 70.1% were female. Ischemia time was more than twenty-four hours in 52.7%; ischemia severity was Rutherford IIb in 58.3%. Arrhythmia was present in 69.7%, and 12.6% were taking anticoagulation drugs. Thirty day postoperative major amputation rate was 9.4% (n=24) and mortality rate was 5.9% (n=15). Predictors of 30-day major amputation include prolonged ischemia time and increased ischemia severity. Previous diagnosis of arrhythmia is associated with lower amputation risk. No association between the studied covariates and mortality were obtained.
DISCUSSION
Our study show ischemia time as leading factor determining limb salvage. Previous studies(7)(8) support this finding. Within different variables that can influence ALLI outcomes, ischemia time is probably the most “modifiable”, emphasizing the importance of health professionals' awareness for this condition to allow timely diagnosis and treatment.
Casillas-Berumen et al(6) recently published a multicenter study (n=1749) whose goal was to assess perioperative morbidity for emergent thromboembolectomy in ALLI and develop a risk prediction model for perioperative mortality; thirty day mortality was 13.9% and identified predictors were male gender, age > 70y, reduced functional capacity, chronic kidney disease and cardiac insufficiency.
Regarding perioperative mortality, we did not find significant association among studied covariates; this can be explained by small number of deaths, what can hinder statistical analyzes. The group mortality rate was unexpectedly low (5.9%) compared with other studies(5)(6), especially because we are focusing on elderly patients. Similarly good results were presented by Galzerano et al(9) in nonagenarians with ALLI, with low 30-day amputation (6.2%) and mortality (5.9%), but study group was smaller (n=15). Future research to better understand these findings could focus on ALLI turndown for surgery on the same period.
Age has been considered to negatively influence outcomes. (5)(6) In our study, we achieve quite good results, considering analyzed patients age. Even comparing octogenarians with nonagenarians, no significant difference was found regarding limb salvage and mortality.
Thromboembolectomy has some drawbacks like inability to vascularize all leg arteries, especially using femoral approach. Back-bleeding is considered an unreliable guide to distal patency. For that matter, Shin et al(10) evaluate limb salvage after thromboembolectomy finished as soon as Doppler signals were detected at one artery at ankle level and noticed that one week later Doppler signals at ankle level could be detected in more than one artery. Completion angiography and other interventional procedures for treatment of ALLI were performed in our center during this period, but these patients were excluded from this study, as previously stated; these procedures needs special facilities such as radiological intervention room or C-arm radiological equipment, and it also needs trained personnel to operate the radiological machines, not always available. In some cases, the patients cannot undergo radiological intervention due to impaired renal function or allergy to contrast dye. In addition, some previous studies suggest that complications (bleeding and access site related) are more frequent with interventional procedures than with surgical thromboembolectomy, and this issue seems more substantial in the elderly.
Common femoral artery approach was performed under local anesthesia and conscious sedation in most cases, by a longitudinal incision. Local anesthesia seems better tolerated by elderly patients with cardiac disease; regional anesthesia is usually contraindicated due to previous heparin administration; general anesthesia is necessary in uncooperative patients or when additional procedures are needed. Data is scarce regarding the optimal anesthetic approach; most series reflect surgeon´s preference in favour of local anesthesia. However, Morris-Stiff et al(11) found absence of an anesthesiologist and operations performed under local anaesthetic to be associated with increased risk of mortality – deepen this issue is necessary. Postoperative care monitoring is crucial as circulation restoration may cause reperfusion injuries leading to cardiac and renal complications; also important is assessment of intra-compartment pressure and performing fasciotomy when indicated.
The observation that around 70% of patients had a known diagnosis of arrhythmia, but only a minority were therapeutically anticoagulated, identifies a major potential target for preventive efforts. Patients with known arrhythmia seem to have more favourable prognosis concerning limb salvage. We are unable to justify this finding – further research is warranted. The retrospective nature of the review precluded complete data collection for all variables and testing of any a priori hypotheses or management algorithms. The study group is single centre, analysing a group of patients managed by a sole working team with similar management approaches. Given to the difficulties in identifying patients treated in other fashions, we only included those patients treated with a thromboembolectomy.
CONCLUSION
Thromboembolectomy is a valid option in ALLI treatment, even for elderly patients with multiple comorbidities. The difference between arrhythmia prevalence and patients taking anticoagulants expose a possible weakness in the management of these patients.
REFERENCES
1. Rutherford RB. Clinical Staging of Acute Limb Ischemia as the Basis for Choice of Revascularization Method: When and How to Intervene. Semin Vasc Surg. 2009;22(1):5-9 [ Links ]
2. Branco BC, Montero-Baker MF and Mills JL. The pros and cons of endovascular and open surgical treatments for patients with acute limb ischemia. J Cardiovasc Surg. 2015;56:1-2 [ Links ]
3. Wang JC, Kim AH and Kashyap VS. Open surgical or endovascular revascularization for acute limb ischemia. J Vasc Surg. 2016;63(1):270-8 [ Links ]
4. Norgren L, Hiatt WR, Dormandy JA, Nehler MR, Harris KA and Fowkes FGR, on behalf of the TASC II Working Group. Inter-Society Consensus for the Management of Peripheral Arterial Disease (TASC II) Eur J Vasc Endovasc Surg. 2007;33:S1eS70
5. Kempe K, Starr B, Stafford JM, Islam A, Mooney A, Lagergren E, et al. Results of surgical management of acute thromboembolic lower extremity ischemia. J Vasc Surg. 2014;60(3):702-7 [ Links ]
6. Casillas-Berumen S, Sadri L, Farber A, Eslami M, Kalish J, Rybin D, et al. Morbidity and mortality after emergency lower extremity embolectomy. J Vasc Surg. 2017;65(3):754-759 [ Links ]
7. Henke PK. Contemporary Management of Acute Limb Ischemia: Factors Associated with Amputation and In-Hospital Mortality. Semin Vasc Surg. 2009;22:34-40 [ Links ]
8. Karapolat S, Dag O, Abanoz M and Aslan M. Arterial Embolectomy: A Retrospective Evaluation of 730 Cases over 20 Years. Surg Today. 2006;36:416–419 [ Links ]
9. Galzerano G, de Donato G, Setacci F, Sirignano P, Sauro L, Cappelli A, et al. Acute limb ischemia in nonagenarians. J Cardiovasc Surg. 2013;54(5):625-31. [ Links ]
10. Shin HS, Kyoung K, Suh B, Jun S, Park JK. Acute Limb Ischemia: Surgical Thromboembolectomy and the Clinical Course of Arterial Revascularization at Ankle. Int J Angiol. 2013;22:109–114 [ Links ]
11. Morris-Stiff G, D'Souza J, Raman S, Paulvannan S, Lewis MH. Update experience of surgery for acute limb ischaemia in a district general hospital–are we getting any better? Ann R Coll Surg Engl. 2009;91:637–640 [ Links ]
Correio eletrónico: mariodpmoreira@gmail.com (M. Moreira).
Recebido a 22 de janeiro de 2018
Aceite a 06 de junho de 2018

