










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkAngiologia e Cirurgia Vascular
versão impressa ISSN 1646-706X
Angiol Cir Vasc vol.8 no.3 Lisboa set. 2012
Transcutaneos Oxygen measurement as a predictor for foot ulcer healingin Diabetic patients
O valor preditivo da Pressão Transcutânea de O2 na cicatrização de lesões do pé diabético
Carolina Vaz, Joana Martins, Rui Guimarães*, Claudia Amaral*, Claudia Freitas*, Joaquim Muras*, Rui Carvalho*, Clara Nogueira, Tiago Loureiro, Luís Loureiro, Diogo Silveira, Sérgio Teixeira, Duarte Rego, Arlindo Matos,Rui de Almeida
Consulta Multidisciplinar do Pé Diabético*
Serviço de Angiologia e Cirurgia Vascular do Hospital de Santo António
Centro Hospitalar do Porto
|ABSTRACT|
Introduction: Transcutaneos oxygen tension (TcPO2) is a noninvasive method that reflects the balance between local oxygen supply and skin oxygenation and is particularly useful in evaluating diabetic vascular disease, because its measurements are not influenced by medial arterial calcifications. The aim of the present study was to determine the predictive value of TcPO2 for foot ulcer healing in diabetic patients submitted to a conservative treatment.
Material/Methods: 127 diabetic patients (135 limbs) with chronic foot ulcers were prospectively evaluated. The age was 67, 2 ± 11, 8 years (mean ± SD) and the diabetes duration was 17,6 ± 9,8 years (mean ± SD). TcPO2 mapping (mmHg) of the involved limb was obtained. Conservative ambulatory treatment was prescribed and wound healing was routinely evaluated. The patients were divided into three groups according to the clinical outcome: complete wound healing, improved wound healing and impaired wound healing.
Results: A significant correlation was found between the presence of infection and TcPO2 values, 26,24 ± 15, 04 (mean TcPO2 with infection ± SD) and 34, 14 ± 16, 9 (mean TcPO2 with no infection ± SD), p<0, 05 t test. Of the 55 limbs who deteriorated, 37 had TcPO2< 30 mmHg, while 39 of the 54 limbs with complete wound healing had TcPO2 ≤ 30 mmHg (p<0,02) (table 1).When a cutoff value of 30 mmHg was used for ulcer healing a positive predictive value of 75% was found.
Conclusions: This prospective study shows that TcPO2 evaluation is an accurately additional tool predictor to assess the ulcer healing outcome in diabetic patients.
Key-words: Transcutaneos oxygen tension, Diabetic foot
|RESUMO|
Introdução: A avaliação da pressão transcutânea de O2 (TcPO2) constitui um método não invasivo de diagnóstico que nos permite quantificar a difusão de oxigénio a nível tecidular. Dado que a sua leitura é independente da calcificação arterial a sua utilização na população diabética é de particular relevância.
O presente trabalho teve como objectivo avaliar o valor preditivo da TcPO2 relativamente á cicatrização de lesões do pé em doentes diabéticos submetidos a tratamento conservador.
Material e Métodos: 127 pacientes diabéticos (135 membros) com úlceras crónicas foram avaliados prospectivamente tendo-se procedido, respectivamente á medição dos valores da TcPO2. A idade média foi de 67, 2 ± 11, 8 anos (média ± dp) e o tempo médio de duração da diabetes foi 17,6 ± 9,8 anos (média ± dp). No follow-up final, os doentes foram divididos em três grupos, de acordo com a evolução clínica: cicatrização completa, melhoria da cicatrização e má evolução da cicatrização.
Resultados: Houve correlação significativa entre a presença de infecção e os valores de PTcO2 medidos, 26, 24 ± 15, 04 (média TcPO2 com infecção ± dp) e 34, 14 ± 16, 9 (média PTcO2 sem infecção ± dp), p <0,05. Dos 55 membros em que se verificou má evolução das lesões, 37 apresentavam TcPO2 <30 mmHg, enquanto que 39 dos 54 membros com cicatrização completa apresentavam TcPO2 ≥ 30 mmHg (p <0,02) (tabela 1). Sendo que estes valores nos permitiram determinar que a pressão transcutânea de oxigénio apresenta um valor preditivo positivo de 75% para valores superiores a 30 mmmHg.
Conclusão: Este estudo prospectivo demonstra que a avaliação PTcO2 constitui uma ferramenta adicional na avaliação da cicatrização das lesões dos doentes diabéticos.
Palavras-chave: Pressão Transcutânea de Oxigénio, Pé diabético
INTRODUCTION
Successful treatment of the patient with diabetes and limb-threatening ischemia requires an accurate assessment of limb perfusion[1,2]. Ankle and toe pressure measurements are presently regarded as optimal criteria for evaluating non diabetic patients.[3] In contrast, these methods often fail in diabetic patients due to the presence of medial arterial calcifications.
Transcutaneos oxygen tension (TcPO2) is a noninvasive method that reflects the balance between local oxygen supply and skin oxygenation[3,4] and is particularly valuable in diabetic vascular disease, since its measurements are not influenced by medial arterial calcifications. Used as a diagnostic adjunct in predicting wound healing in diabetic patients, it is also a tool to determine the decision to perform revascularization or amputation surgery.[5]
The aim of the present study was to determine the predictive value of TcPO2 for foot ulcer healing in patients with diabetes treated conservatively.
METHODS
An unconsecutive group of 127 diabetic patients (135 limbs) with chronic foot ulcers was studied prospectively from March 2004 to December 2008. All patients were referred to our multidisciplinary department of diabetic foot pathology and initially treated as one day clinic regimen with regular visits every 4-6 weeks. Clinical evaluation included surgical and medical history and risk factors for peripheral occlusive disease. Foot lesions or rest pain were assessed for the presence of sensory-motor neuropathy, infection and peripheral occlusive disease. Metabolic control was optimized when possible, and antibiotics were used when clinical signs of infection were present. The ulcers were debrided when considered necessary and a foot x-ray was performed in cases of suspected osteomyelitis.
TcPO2 monitor was used to simultaneously measure the TcPO2 values at the chest and in the proximity of the lesion with the patient resting in the supine position. The measuring site was carefully cleaned by a disinfection solution. The calibration time took an average 10 minutes and the laboratory room temperature was maintained at approximately 25ºC.
After a follow up time, the patients were divided into three groups according to the clinical outcome: complete wound healing, improved wound healing and impaired wound healing.
Statistical analysis was performed on SPSS (Statistical Package in the Social Sciences); Categoric data was presented as absolute frequencies and percent values. Values are expressed as mean ± standard deviation. Correlations between the TcPO2 values and other variables were analyzed with Pearson’s test. The cut-off values were provided by receiver operating characteristic (ROC) curves. Differences with p value less than 0.5 were considered statistically significant.
RESULTS
The diabetic patients evaluated had a mean age of 67, 2 ± 11, 8 years (± SD) and the diabetes duration was 17, 6 ± 9, 8 years (mean ± SD).
Fifty four of the patients were women (42, 5%), with a mean (SD) age of 68, 7 (± 10, 3 years); the mean (SD) age of the male population was 66, 0 (±12,7 )years. | TABLE I |
| TABLE 1 | Demographic and clinical characteristics of study population
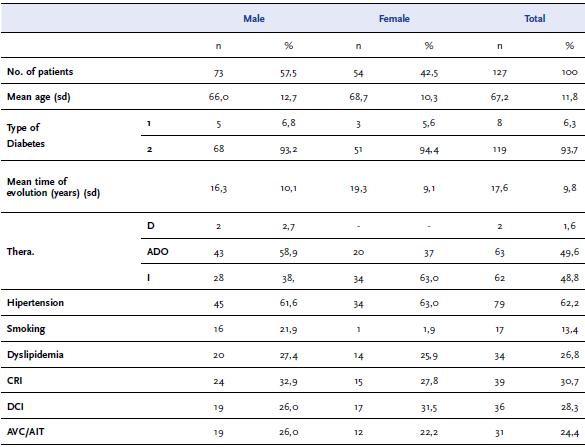
Six major cardiovascular risk factors were assessed, Hypertension being present in the majority of cases (62, 2%). | TABLE I |
Fifty nine of the ulcers (43, 7%) had associated necrosis and in eighty cases (59, 3%) signs of infection were present. A primary minor amputation was performed in 38 limbs (28, 1%).
Considering the anatomic distribution of the lesions, 71,8% were digital, 15, 5% were plantar and 12, 7% were at the dorsum of the foot. No significant differences were found between ulcer distribution and final prognosis.
Significant correlations were found between the presence of infection and TcPO2 values: 26, 24 ± 15, 04 (mean TcPO2 with infection ± SD) and 34, 14 ± 16, 9 (mean TcPO2 with no infection ± SD), p<0, 05 t test.
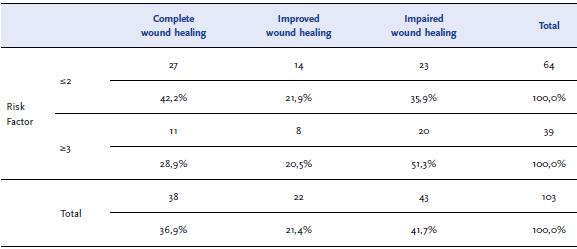
Regarding the outcome of the ulcers it was found that patients with two or less risk factors, had in 64, 1% of the cases a good prognosis with improved or completed ulcer healing in contrast with the patients with three or more risk factors that in 51, 3% of the cases had impaired ulcer healing | TABLE II |. Ten of them (50%) deteriorated and necessitated major amputation. Statistical analysis did not find a significant correlation between these two variables but it reveals an important tendency, also smoking was not associated with poor prognosis.
| TABLE 2 | Correlation between final prognosis and risk factors
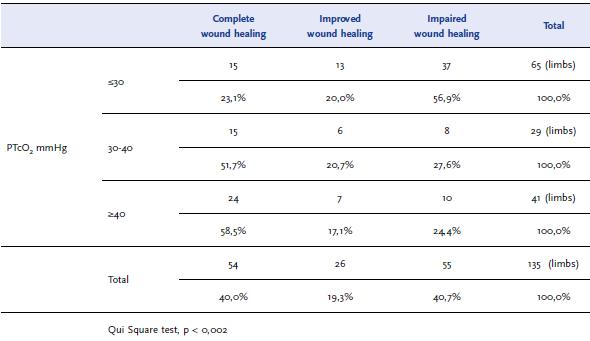
In the overall series according to the TcPO2 measurements | TABLE I |, of the 55 limbs who deteriorated, 37 had TcPO2< 30 mmHg, while 39 of the 54 limbs with complete wound healing had TcPO2 ≥ 30 mmHg (p<0,02).
When a cutoff value of 30 mmHg was used it provided a positive predictive value of for ulcer healing 75%.
DISCUSSION
There is no doubt that in diabetic patients with chronic foot ulcers the assessment of the healing potential of the lesion is of paramount importance, in order to achieve successful treatment. The critical issue appears to be the parameter that should be used to evaluate this entity.
TcPO2 measurements has been used over the past decade to assess the adequacy of distal perfusion[6,7] in order to determine ulcer healing capability in the presence of significant peripheral vascular disease.
In our study all the diabetic patients had several risk factors associated. In contrast to other studies smoking was not associated with poor prognosis regarding ulcer healing, but the association of 3 or more risk factors revealed a tendency towards worst ulcer healing.[8,9]
We found that infected lesions were associated with lower TcPO2 values when compared with no infected lesions. (p<0, 05 t test)
It is reported in some series[10,11], that infection may confound the accuracy of TcPO2 mapping; if Transmetatarsal TcPO2 level is less than 30 mmHg in an ulcer associated with infection the test should be repeated after antibiotic administration.
It is also described by Yamada[8] et al that the main limitation during the TcPO2 measurement is the ulceration or tissue loss associated in diabetic foot ulcers; In his series TcPO2 could not be measured in 36 out of 211 patients because of the major tissue loss reported but that difficulty was not reported in our study.
Our findings corroborate other studies [8,12,13,14] showing that measurements of less than 30mmHg are associated with a high risk of healing failure with conservative treatment and that other treatment option such as a revascularization procedure should be considered in these patients.
According to our study an absolute TcPO2 level of 30 mmHg or greater appears to be an accurate cut off point for the selection of conservative versus surgical treatment for almost all diabetic foot problems; it reflects a predictive positive value of 75%. We believe that the conservative management scheme however requires diligent patient follow-up, with proper outpatient wound care, debridements and minor foot amputations when necessary.
CONCLUSION
The etiology of chronic diabetic foot ulcers is multifactorial, and prediction of ulcer healing is a difficult problem to solve.
The results of the present study show that TcPO2 evaluation is a good additional tool predictor to assess the ulcer healing outcome in diabetic patients.
| TABLE 3 | TcPO2 values by classes in relation to wound outcome
REFERENCES
[1] Vincent E. de Meijer, Hans P. van’t Sant, Sandra Spronk et al , Reference value of transcutaneos oxygen measurement in diabet patients compared with non diabetic patients, J Vasc Surg 2008; 48: 382-8
[2] La pression transcutanée d’oxygène ( TcPO2 ): Intèrêts et Limites, Diabetes & Metabolism, 1998, 24, 371-376
[3] L. Norgren, W. R. Hiatt, J.A. Dormandy et al, Inter-Society Consensus for the management of Pheripheral Arterial Disease (TASC II), Eur J Vas Surg, 2007,33, S1-S70 [ Links ]
[4] Majid Kalani, Kerstin Brismar, Bengt Fagrell et al, Transcutaneos Oxygen Tension ans Toe Blood Pressure as Predictors for Outcome of Diabetic Foot Ulcers, Diabetes Care, 1999; 22:147-151 [ Links ]
[5] Kathleen Rich, The effects of leg/body position on transcutaneous oxygen measuremnts after lower- extremity arterial revascularization, J, Vasc Surg 2007; 26:6-14 [ Links ]
[6] Luís M. Alvim Serra et al, Pé Diabético, Manual para a prevenção da Catástrofe, 2008 [ Links ]
[7] National Healing Corporation, Wound healing perspectives, 2004, 1:4 [ Links ]
[8] Tetsuya Yamada, Takashi Ohta, Hiroyuki Ishibashi et al, Clinical reliability and utility of Skin perfusion pressure measurement in ischemic limbs-Comparison with other noninvasive diagnostic methods, J vasc Surg 2008; 47:318-23 [ Links ]
[9] E. Faglia, G. Clerici, M. caminiti et al, Preditive Values of Transcutaneos Oxygen tension for Above the ankle Amputation in Diabetic Ptients With Critical Limb Ischemia, Eur J Vasc Endovasc Surg, 2007, 33:731-736 [ Links ]
[10] Jeffrey L. Ballard, Clifford C. Eke, T. J. Blunt, A prospective evaluation of transcutaneos oxygen measurements in the management of diabetic foot problems, J. vasc Surg 1995; 22:485-92 [ Links ]
[11] T. J. Blunt and Allen Holloway, TcPO2 as na accurate oredictor of therapy in Limb Salvage, Ann Vasc Surg, 1996; 10:224-227 [ Links ]
[12] Amanda I. Adler, Edward J. Boyko, Jessie H. Ahroni et al, Lower Extremity Amputation in Diabetes, Diabetes Care, 1999, 22: 7 [ Links ]
[13] Cao P, Eckstein HH, De Rango P, Setacci C, Ricco JB, de Donato G, Becker F, Robert-Ebadi H, Diehm N, Schmidli J, Teraa M, Moll FL, Dick F, Davies AH, Lepäntalo M, Apelqvist J. Chapter II: Diagnostic methods. Eur J Vasc Endovasc Surg. 2011 Dec;42 Suppl 2:S13-32. Review. [ Links ]
[14] Faglia E, Clerici G, Caminiti M, Quarantiello A, Curci V, Somalvico F., Evaluation of feasibility of ankle pressure and foot oximetry values for the detection of critical limb ischemia in diabetic patients, Vasc Endovascular Surg. 2010 Apr;44(3):184-9 [ Links ]

