











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
Permalink
Introduction
Knowledge of the most common root canal system configuration and its possible variations is fundamental for a proper clinical evaluation and good treatment planning. The root canal system morphology may be complex, and being able to correctly identify the tooth anatomy increases the success rate for performing an adequate root canal disinfection and filling, which may ultimately improve the root canal treatment outcomes.1,2
Cone-beam computed tomography (CBCT) imaging represents a valuable method for the clinical assessment of the root canal configuration. It allows for an analysis of the anatomical details with reliable image resolution and, due to its three-dimensional nature, offers the possibility to evaluate na individual tooth in multiple views.3,4Currently, many CBCT prevalence studies analyzing the root canal anatomy in diferente countries are available in the literature due to the worldwide spread of this technology.5,6
The root canal system anatomy may vary according to the patient’s ethnicity and geographic origin.5,7-9 For instance, compared to other populations, the Asians presente a substantially lower prevalence of the second mesiobuccal canal (MB2) in maxillary molars and higher proportions of three-rooted morphologies and single-rooted configurations in mandibular first molars and second molars, respectively.5
In European populations, higher percentages of maxillary first premolars presenting two roots were noted.5 Moreover, mandibular second molar’s C-shaped morphologies have been reported in higher proportions in East Asian countries (39.6%), while lower percentage were noted in Europe (8.9%), Africa (9.2%), Latin America (9.7%), West Asia (9.9%), and North America (11.3%).9
Most of the available literature regarding the prevalence of different root canal system configurations is based on studies addressing one single sub-population from a specific country or geographic region, not allowing for an ethnicity association analysis. This lack of information for possible ethnic group’s anatomy variations is a matter of concern since it could be useful in endodontic therapy to help the clinician anticipate possible ethnic morphologic variations, thus avoiding potential complications. Brazil is considered a country with strong ethnic diversity.
It has one of the most heterogeneous populations in the world due to the coexistence of multiple ethnicities with a genetic inheritance deriving from the four main continental groups (Europeans, Africans, Asians, and Native Americans).10 The root and root canal anatomy among the diferente Brazilian sub-population groups has never been fully assessed, and related literature is lacking compared to other populations such as Asians and Caucasoids.7,11-13Consequently, as no attempt to gather previous results has been performed, the current knowledge about dental morphology in the Brazilian population is based on those individual studies with disperse data from the several sub-population groups. Within this background, this systematic review aimed to evaluate CBCT prevalence studies in order to comprehend the root and root canal configuration types in the Brazilian population.
Material and Methods
The present systematic review’s methodology has been registered in the International Prospective Register of Ongoing Systematic Reviews (PROSPERO) (CRD42019141229) and followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines.14 The review question considered the Condition, Context, and Population format (CoCo-Pop) for prevalence studies’ reviews,15 and stated: “What are the prevalence of Vertucci’s canal configuration types and the number of roots in each tooth groups in Brazilian human patients submitted to CBCT examinations?”
A systematic literature search was conducted in PubMed, ScienceDirect, Lilacs, and Cochrane Collaboration to identify all relevant cross-sectional studies (prevalence studies) on root and root canal anatomy using CBCT assessment. The terms used in each electronic database are summarized in Table 1.
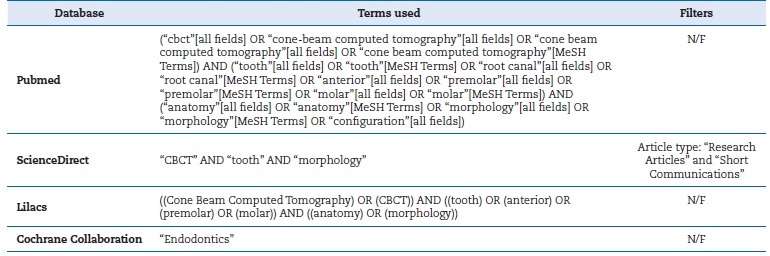
N/F: No filter
The full reference list of all relevant studies identified in the four electronic databases was hand searched. Moreover, three peer-reviewed endodontic journals (Journal of Endodontics, International Endodontic Journal, and Australian Endodontic Journal) and two peer-reviewed evidence-based dentistry journals (Evidence-Based Dentistry and Journal of Evidence-Based Dental Practice) were also investigated. Attempts were made to contact the authors of previous studies via email to gather additional information on scientific articles, gray literature, or any ongoing project that could be promptly accessed.
The final study selection followed a two-stage assessment. In the first stage, study titles and abstracts were assessed and, considering pre-established inclusion/exclusion criteria (Table 2), labeled as ‘relevant’ or ‘irrelevant.’ In the second stage, the relevant studies’ full text was analyzed, and they were re-labeled according to the same criteria. The final pool of selected studies included the ones that overcame these two assessment stages after being identified in the electronic databases or by the manual search or being supplied by the authors. In order to assess the studies’ scientific merit, two evaluators (JM and DM) critically appraised the final pool of studies’ full texts independently, using the Joanna Briggs Institute (JBI) Critical Appraisal tool for systematic reviews of prevalence studies. The assessment discrepancies between evaluators were debated until mutual accordance was reached. Cohen’s kappa value was calculated to determine the inter-rater reliability between both evaluators (Table 3). A value above 0.61 was considered a good agreement. Each study’s risk of bias (RoB) was categorized according to the final JBI scores, as follows: ‘high’ RoB for scores equal or lower than 49%, ‘moderate’ for scores between 50% and 69%, and ‘low’ for scores higher than 70%.16,17
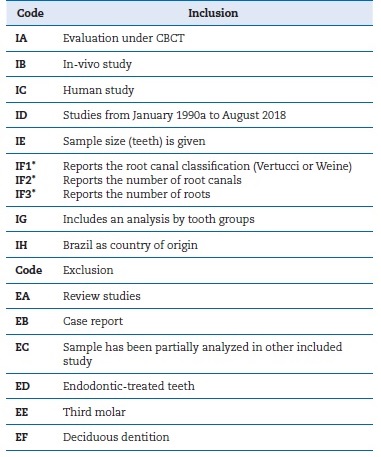
* Present, at least, one of the inclusion codes
a Decade of CBCT introduction
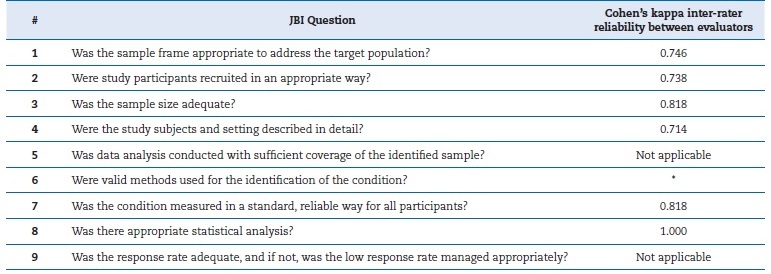
Table 3 Questions of the Joanna Briggs Institute (JBI) Critical Appraisal tool for systematic reviews of prevalence studies.
* No statistics were calculated because Observer B’s values were constant
No language restrictions were applied. The literature search was conducted between May and August 2018, updated on October 2019, and considered all available studies between January 1990 and September 2019.
Results
Twenty relevant studies were identified following the search strategy: nineteen provided by the electronic databases, and one identified manually. Ten authors were contacted by email with four replies (40.0% return rate), but no more studies were added. Of the twenty studies submitted to full-text assessment, three were excluded18,19,20(Table 4), and seventeen, with a global average JBI score of 51.3%, were pooled in the presente review.7,10-13,21-33Eight studies were classified with a high RoB, four with a moderate RoB, and the remaining five with a low RoB. According to the JBI levels of evidence, the present systematic review could be categorized as Level 4a (systematic review of descriptive studies). The PRISMA flowchart can be assessed in Figure 1.

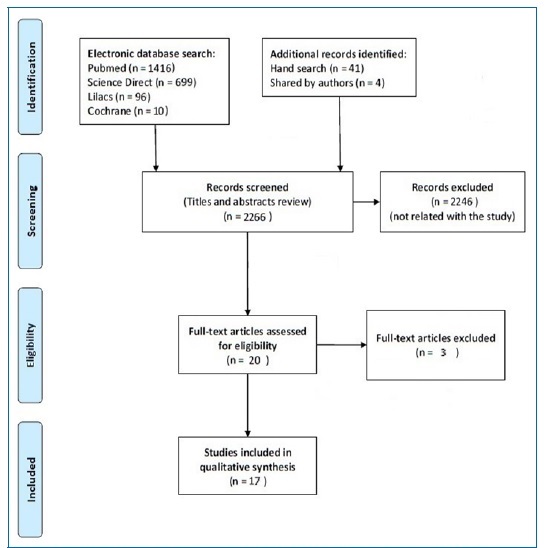
Figure 1 Flowchart of the literature search and the selection process of studies according to PRISMA statements for qualitative synthesis.
The final group of studies reported data from at least 4086 patients (one study did not state the number of patients).25At least 1518 females and 1860 males were screened (seven studies did not report gender),7,13,21,22,25,27,29and the average age was 43.3 years (ranging from 31.4 to 49.4 years), based on the seven studies that reported it.7,23,24,26,27,30,33The final data regarded 9745 teeth: 1800 anterior, 1780 premolars, and 6165 molars. The seventeen studies selected in the present review included information from eight Brazillian states (Ceara, Goias, Parana, Piaui, Rio de Janeiro, Rio Grande do Sul, Santa Catarina, Sao Paulo) (Figure 2) and were published in two different languages (English [n=15] and Portuguese [n=2]).
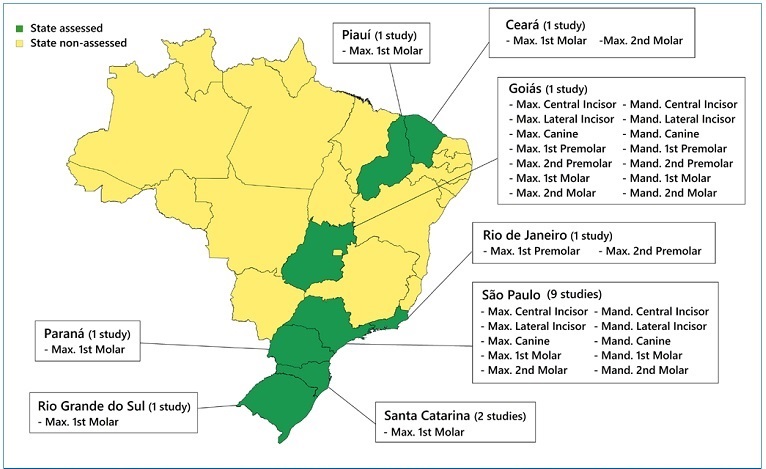
Figure 2 Representative image of the included studies according to tooth group and Brazilian sub-populations analyzed.
The CBCT settings, patient demographics, and results regarding the prevalence of root and root canal system configurations for all groups of teeth are summarized in Tables 5, 6, and 7. Anterior teeth were almost entirely single-rooted, except for mandibular canines, whose percentage of two roots was as high as 3.0%. Maxillary anterior teeth generally presented one single main canal, while mandibular incisors were associated with a high prevalence of a second root canal, representing a proportion of around 35.0% and 40.0% for the central and lateral incisors, respectively. The Vertucci’s Type III (1-2-1) was the most common two-canal variation for mandibular incisors. A high inconsistent (within sub-region) prevalence of the two-rooted configuration (between 17.0% in the Midwest region and 28.4% in the Southeast region) and two root canals (from 50.1% in the Southeast region to 75.0% in the Midwest region) was noted in maxillary second premolars. The mandibular premolars’ most common anatomy was one root with a single root canal, even though the first mandibular premolar presented 30.0% of cases with at least two root canals.
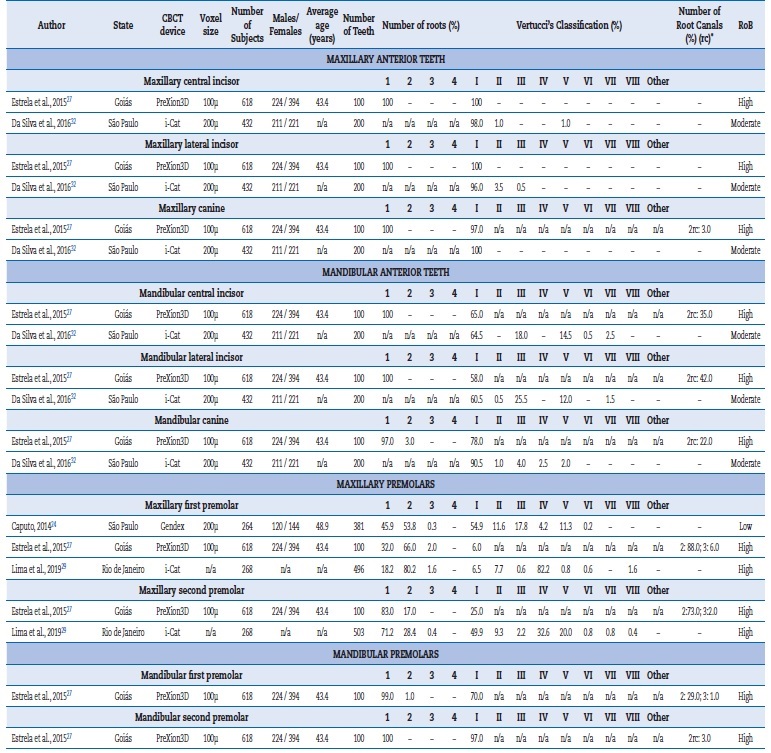
n/a, not available; RoB, Risk of Bias; CBCT, Cone Beam computed tomography; * If no Vertucci’s classification was provided
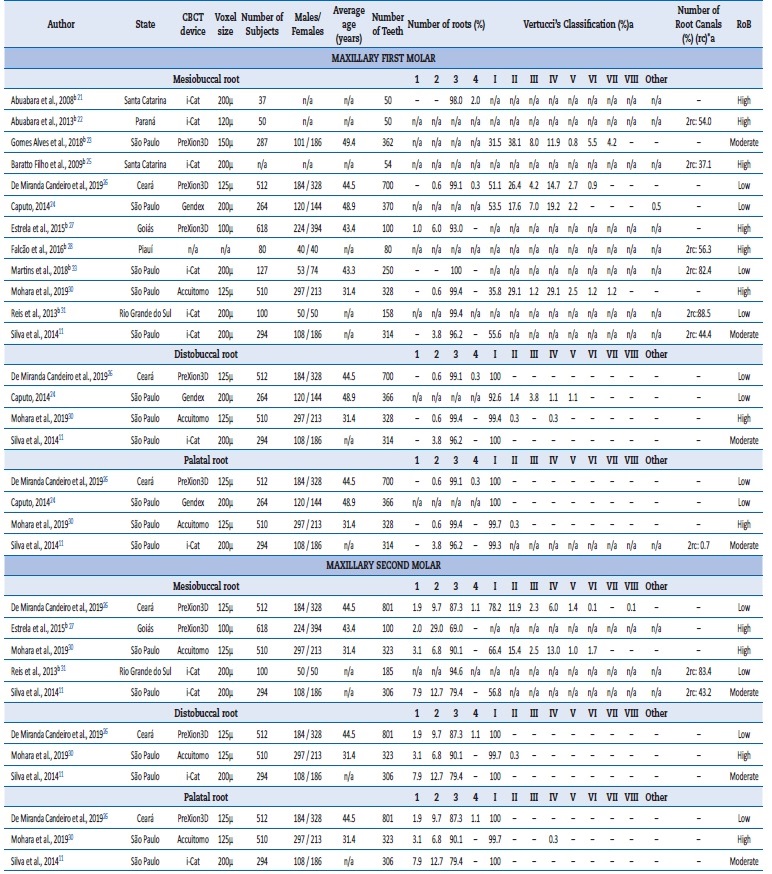
n/a, not available; RoB, Risk of Bias; CBCT, Cone Beam computed tomography; * If no Vertucci’s classification was provided; a Data regarding maxillary molars with independent roots; b The studies presenting data regarding the number of roots and/or mesiobuccal root canal configuration are displayed only in the mesiobuccal root section
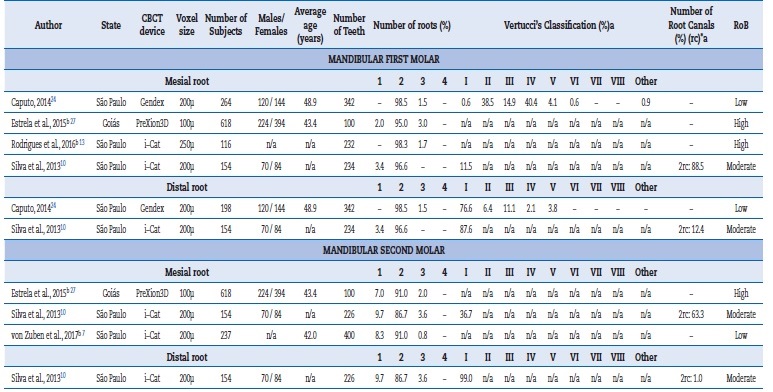
n/a, not available; RoB, Risk of Bias; CBCT, Cone Beam computed tomography; * If no Vertucci’s classification was provided; a Data regarding mandibular molars with independent roots; b The studies presenting data regarding the number of roots and/or mesial root canal configuration are displayed only in the mesial root section
Maxillary molars showed mostly a three-rooted configuration (between 96.2% and 100% of cases) with a high proportion of MB2 ranging from 37.1% to 88.5% and 21.8% to 83.4% for the first and second maxillary molars, respectively, depending on the sub-population. The most common Vertucci’s classifications in the maxillary first molars’ mesiobuccal root were Type I and II, followed by Type IV. Distobuccal and palatal roots generally presented a single root canal. Maxillary second molars also showed a considerable number of single (between 1.9% and 7.9%) and two-rooted (between 6.8% in the Southeast region and 29.0% in the Midwest region) configurations. Regarding the mandibular teeth, the two-root configuration was the most common for both first (between 95.0% and 98.5%) and second (between 86.7% and 91.0%) molars. However, the mandibular second molar also showed a high percentage of single-rooted teeth (between 7.0% and 9.7%). The mandibular molars’ mesial root presented mostly two root canals, mainly as Vertucci’s Types II and IV. Mandibular first molars presented a high prevalence of a second canal in the distal root (between 12.4% and 23.4%), mainly as Vertucci’s classification Type III, followed by Type II.
Discussion
Populations with different demographic origins may express variations in their dental morphology.7,33The present study performed a systematic review aimed to analyze the root and root canal configuration of the heterogeneous Brazilian population, based on the available anatomy prevalence studies using CBCT performed on different Brazilian sub-populations.
The results identified similarities as well as differences between the analyzed sub-populations. The CBCT was chosen as the assessment tool for the presente study because it provides an accurate three-dimensional imaging analysis of each tooth’s external and internal dental anatomy. Moreover, it estimates the collected data with the clinical setting findings since it is used for both endodontic diagnosis and treatment.6 CBCT has demonstrated to be a reliable resource for the analysis of root canal configuration prevalence and is currently considered the most reliable clinical approach to estimate the proportion of individuals presenting with a specific dental morphology.5,34 Furthermore, regarding epidemiological studies’ methodologies, CBCT can perform non-destructive analysis of the patients’ full dentition, consecutively collected in a specific sub-population,5,6 allowing the collection on large sample sizes with a reduced sampling bias. However, the risks and benefits of using CBCT should always be considered. The focus of interest - the root canal anatomy of teeth - must include a smaller field of view (FOV) to ensure increased resolution for anatomical details and reduced radiation exposure.4 Also, the ALARA principles (As Low As Reasonably Achievable) must always be considered before image diagnosing exams.4
After the qualitative synthesis of the included studies, a tendency for single root and single root canal configurations was observed for maxillary anterior teeth. This finding agrees with previous clinical CBCT studies assessing diferente sub-populations from diverse origins or different ethnic backgrounds.5,8,27,32,35,36Moreover, it is in agreement with ex-vivo studies within the Brazilian population.37,38
Regarding the mandibular anterior teeth, a high prevalence of a second root canal was noted, which corroborates previous literature assessing non-Asian countries,5,8,39,40while Chinese tend to present lower percentages.8,41-43However, it should be noted that two Brazilian sub-populations (from Goias and São Paulo) in the present study showed percentages higher than those reported by previous studies in sub-populations from other regions.5 The present study reported a second root canal proportion of around 35.0% and 40.0% for the central and lateral incisors, respectively, while in the mandibular canines it ranged between 9.5%32 and 22.0%.27 Considering that most of these mandibular anterior teeth’ root canal systems were classified as Vertucci’s Type III or V, the complexity of detecting an additional canal in a narrow root and a single canal entrance should be highlighted. In this sense, the use of a dental operative microscope to identify extra root canals should be considered, although this equipment might present limitations when assessing the internal morphology of mandibular incisors with
two canals.44 In these cases, imaging evaluation could be more useful, especially when performing an adequate double-angulation periapical radiography technique or a tomography examination.45 Therefore, knowledge of anatomy, adequate equipment use, and clinical awareness is critical for the proper endodontic treatment of mandibular anterior teeth, especially in population groups with higher chances of presenting a second root canal, such as the Brazilian or the Israeli populations.46
Regarding the premolars’ anatomy in the Brazilian population, the mandibular premolars presented a less complex morphology with fewer roots and root canals than the maxillary premolars. Moreover, except for the maxillary first premolar, all other premolars groups were mostly single-rooted teeth.
The high percentages of the two-rooted configuration in maxillary first premolars observed in the present study for Brazilian sub-populations, ranging between 53.8%24 and 80.2%29, agree with results from European populations (ranging from 49.2%8 to 62.4%47), being higher when compared to Asian countries (from 16.8%8 to 30.1%48). It was also observed that maxillary first premolars presented a two-rooted configuration in 80.2% of the Southeast region of Brazil’s sample (Rio de Janeiro)29compared to 66.0% in the Midwest of Brazil’s sample (Goias).27
This may demonstrate a regional anatomic behavior within Brazil regions. Nevertheless, further studies are necessary to confirm this tendency. It would be interesting to assess the Northwestern states of the country, such as Acre, Amazonas, or Rondonia, whose population’s ethnicity is more influenced by the original Brazilian natives compared to the Eastern states due to not being so exposed to the immigration of the past four centuries that brought foreign ethnic groups to Brazil.
As for the maxillary second premolar, higher proportions of two-rooted configurations were noted in the Brazilian population, ranging from 17.0%27 to 28.4%29, compared to Asian studies, which present percentages ranging between 0.8%8 and 13.5%.49 Moreover, these results in the Brazilian sub-populations are also higher than those of European countries such as Portugal (5.3%),8 Spain (15.5%),50 or Germany (17.0%),47 although not presenting such expressive differences as with the Asian populations.
Regarding the maxillary molars, the MB2 canal’s identification and clinical management are a great challenge for practitioners, and missing it may lead to unsuccessful endodontic treatments.2,51The present study identified a wide range of MB2 canal prevalence for both maxillary first (between 37.1%25 and 88.5%31) and second molars (between 21.8%26 and 83.4%31).
Generally, there is a tendency for lower percentages of MB2 canals in maxillary second molars than in first molars,5,8,52,53but that condition was not markedly evident in the presente review. The proportion of MB2 canals in maxillary molars varies considerably in the worldwide populations,33,52maybe not only due to the method of assessment or the evaluator’s experience, but also the assessed population’s intrinsic characteristics, which could be influenced by factors such as anthropological origins or demographics. Higher percentages of MB2 root canals have also been noted in maxillary molars from males and younger patients,8 which corroborates a recente CBCT study from a Brazilian Northeast sub-population.26
Additionally, the three-rooted configuration of maxillary molars has been associated with higher percentages of MB2 root canals.33In the present review, the three-rooted morphologies in the Brazilian sub-populations ranged between 93.0% and 100% in first molars and between 69.0% and 94.6% in second molars, which is in agreement with studies from other geographic regions.5 Thus, this external characteristic might not interfere with the Brazilian intrinsic MB2 prevalence. The most prevalent Vertucci’s classifications observed in the maxillary first molars’s mesiobuccal root were Types I and II, followed by Type IV. The use of a dental operating microscope and ultrasonic tips are highly recommended to effectively address this high prevalent MB2 root canal, mainly in cases where its orifice opening in the pulp chamber floor is not evident.51,54
As for the mandibular molars in the Brazilian population, the two-rooted configuration with two root canals in the mesial root and a single canal in the distal root was the most common morphology in the present review. The most common root canal classifications in the mandibular first molar’s mesial roots
were Vertucci’s Types II and IV, with the root canal orifice openings generally perceptible in the pulp chamber floor. Caputo,24 who analyzed a Brazilian sub-population from Sao Paulo, reported a proportion of mesial canals ending in one single apical foramen as high as 54.0%. Not enough data is available regarding the root canal classification for the second molar’s mesial root to allow proper analysis. Compared to the mandibular first molars, the second molars showed a higher prevalence of single-rooted configurations, ranging between 7.0%27 and 9.7%,10 and three-rooted configurations, ranging from 0.8% 7 to 3.6%.10
Not much difference was noted between Brazilian sub-regions. The low proportion of mandibular molars presenting three roots contrasts with the Asian population results, with an extra distal root in 32.0% of the cases.48It should be pointed that, although no third root canal in mandibular molars’ mesial roots was documented in the present study, this configuration has been documented in ex-vivo studies with a Brazilian sample.55,56 Furthermore, clinicians should be aware of the high prevalence of a second root canal in the distal root of mandibular first molars, which may be as high as 23.4%.24
In the present systematic review, all studies that fulfilled the inclusion criteria were submitted to a critical appraisal regarding their methodology, using the JBI Critical Appraisal tool. Depending on the JBI positive answers, each study score could range from 0% to 100%. Although no study was excluded, independently of its quality assessment score, to avoid losing potentially relevant data, this methodology allowed understanding the possible RoB of each study and the global RoB panorama regarding the pooled studies’ design, methodology, and analysis. Considering that eight studies were classified with high RoB, four with moderate RoB, and five with low RoB with inconsistent results in some of the analyzed outcomes, the level of aggregate RoB of the pooled studies may be scored as medium with a varying level of consistency, while the strength of the evidence might be classified as moderate with satisfactory completeness.
One of the present review’s main strengths is the inclusion of only studies that evaluated patients in specific regions, approaching results to the clinical settings. Moreover, the main applicability of the review evidence is related to the awareness of the root and root canal morphology of the studied population and potential differences in their sub-populations, na approach that represents the best available efforts to collect epidemiological data regarding the tooth morphology of a multi-ethnic population on its sub-regional locations.
A limitation of many CBCT prevalence studies is making no effort to confirm the anthropological origins of the included patients. Thus, ethnical and regional features can be misinterpreted, mainly in heterogeneous countries such as Brazil,
Australia, or the United States. One limitation of the presente review is the absence of information from most of the country states and limited data from the ones that have been addressed, which consequently requires a careful extrapolation of the review results to the global population (external validity).
Another study limitation is the low level of evidence (Level 4a), which is related to the nature of a review focused on observational studies.
As a recommendation for future cross-sectional studies on tooth anatomy, study design checklists should be used to provide more reliable data with a reduced RoB. Additionally, considering that no information is currently available regarding possible morphological variations within regions of large countries, more studies are required in large-sized and multi-ethnic countries in order to understand if differences exist within its own sub-regional locations that might justify some inconsistency of the data.
Conclusions
In conclusion, the Brazilian sub-populations present consistente and inconsistent results regarding the prevalence of root and root canal configurations depending on the outcome being assessed. A higher prevalence of mandibular anterior teeth presenting two root canals was observed in the analyzed Brazilian sub-populations. Moreover, a high proportion of the two-rooted configuration and two main canals were reported in maxillary second premolars, while the MB2 canal presented similar ranges between maxillary first and second molars. Further studies on morphological tendencies on regional anatomic variations within Brazil are recommended.
Clinicians should be aware that possible morphologic variations might exist between sub-population of large-sized and multi-ethnic countries.

