











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
Permalink
INTRODUCTION
During the last decades, several publications have used lactate as a marker of training adaptations and a predictor of performance (Hahn, Bourdon, & Tanner, 2000). However, the high variability associated with protocol procedures in different studies makes comparative analysis difficult since they differ in concepts, methodologies, and the interpretation of results (Faude, Kindermann, & Meyer, 2009).
In the control and evaluation of international rowers, it is common to use the discontinuous incremental protocol to determine the intensity equivalent to the anaerobic threshold, a physiological criterion commonly used in training control (Beneke, Leithãuser, & Hütler, 2001). The results obtained through the incremental protocol have been considered essential for the training load prescription and competition preparation (Nolte, 2005).
A method considered valid for determining the anaerobic threshold (AnT) is the lactate maximal steady-state test (MLSS) (Beneke, 2003; Billat, Sirvent, Py, Koralsztein, & Mercier, 2003; Urhausen, Weiler, & Kindermann, 1993). The MLSS aims to identify the intensity at which the lactate concentration does not increase by more than 1 mmol/L during the final 20 minutes of a continuous 30-minute test with constant load. However, despite being the most suitable for assessing an athlete's cardiorespiratory capacity in the aerobic domain, the test has the disadvantage of being very long. This characteristic imposes a high strain on the athlete, often causing changes in the training plan for several days. This limitation often leads to opting for incremental tests (continuous and discontinuous) to determine the intensity equivalent to AnT, either through different modulations of the lactate accumulation curve or from fixed lactate concentrations (Beneke, 2003). This option has the advantages of ease and economy in the implementation and can be carried out during any training period. The validity of some of the protocols has been contested by several authors (Faude et al., 2009; Foxdal, Sjodin, & Sjodin, 1996; Heck et al., 1985), mentioning, among other reasons, that the duration of the step duration may influence the value found for the anaerobic threshold. The use of the 3 minutes steps in an incremental protocol has become common in the evaluations of rowing athletes (Beneke, 1995), but it is also applied in other sports, such as runners and cyclists (Faude et al., 2009). In some cases, the intensity performing at 4 mmol/L during protocol could be underestimated compared to MLSS (Baldari & Guidetti, 2000).
In this sense, the relevance of defining a proper incremental protocol that indicates the anaerobic threshold intensity with higher precision arises. Thus, this study proposes to evaluate which step duration in an incremental protocol (3 minutes, 5 minutes or 7 minutes) allows for identifying the intensity equivalent to the 4mmol/L of lactate accumulation (AnT4), which is the most strongly with the intensity of the maximal lactate steady preparation state (MLSS).
METHOD
Subjects
Ten elite Portuguese rowers volunteered for this study, aged between 19 and 32 years (25.1± 4.82 years), with a height of 177.5± 5.50 cm and 69.8± 2.74 kg of body mass. All athletes belong to the senior lightweight category, having extensive experience in the sport (10± 4.99 years of practice), representing the national team in World Championships (n= 8) and Olympic Games (n= 2). All participants were informed in advance of the study's objectives and gave their voluntary written consent. The scientific board approved the study of the Faculty of Sport of the University of Porto (FADEUP) following the Helsinki Declaration and the Oviedo Convention.
Instruments
To determine the rowers’ body mass and height, a Tanita scale model InnerScan BCM (Tanita, Japan) was used with a precision of 0.1 kg and a graduated stadiometer with an accuracy of 1 mm. Skinfolds were measured using a calliper (Lange) with a 10 g/mm2 pressure. All evaluation rowing protocols were performed on the Concept2 Model PM3 ergometer (Concept2, England) adjusted to a drag factor of 130 (Nolte, 2005), a value that simulates the vessel's resistance in the water considering the rower's body mass. Heart rate recording was performed at 5 seconds intervals using an RS800cx heart rate monitor (Polar Electro, Finland).
Lactatemia was obtained using the LactatePro blood lactate analyser (Arkray, Japan) with the respective lactate reactive strips. Capillary blood micro samples were collected in the earlobe (Dassonville et al., 1998) at a maximum interval of 45 seconds (Kass & Carpenter, 2009) immediately after each period of effort.
Procedures
All the athletes’ coaches were informed of the procedures and the importance of avoiding higher training loads 48 hours before the applied protocols, respecting the conditions for obtaining the best performance in the 2,000 m test, avoiding stressful efforts and favouring the maintenance of the usual routines in food and hydration. The interval between trials was at least 48h. During this period, athletes were asked to perform low-intensity recovery training sessions.
On the first day of testing, an anthropometric assessment was carried out. After 15 minutes of warm-up at low intensity, the athletes performed an “all-out” protocol of 2,000 m on a rowing ergometer. The intensity (power) and the maximal heart rate during the protocol were assessed.
The maximum power at stable lactate (MLSS) intensity was determined in the following sessions. The MLSS was determined according to the methodology adopted by Beneke (1995). The protocol defines the maximum constant intensity (power) where the lactate concentration does not increase by more than 1 mmol/L during the final 20 minutes of the 30 minutes of the continuous constant load test. Capillary blood samples were taken at the 10th, 15th, 20th, 25th and 30th minutes, and heart rate was recorded. The initial constant load was 60% of the power obtained in the maximum performance “all-out” 2,000 m, applying increments ≥ 2.5% during several moments (3 to 5 days) until the steady state was reached.
Finally, in the following sessions and respecting 48 hours of recovery, incremental protocols were performed to determine the power at the concentration of 4 mmol/L of lactate. Three incremental protocols were performed with different step durations, namely 3 minutes, 5 minutes and another step with 7 minutes, to determine the AnT intensity. All protocols were performed in random mode. The initial load was 60% of the power obtained in the maximum performance “all-out” 2,000 m, applying increments of 5% until the athletes reached above 6mmol/L of blood lactate. Through linear interpolation, the external mechanical power of the rowing and the heart rate corresponding to the anaerobic threshold was determined using a fixed concentration of 4 mmol/L of blood lactate.
Statistical analysis
Exploratory data analysis will be focused on descriptive statistics values, mean (M), standard deviation (SD), minimum (Min) and maximum (Max) values. In addition to the information produced by the standard deviation, the dispersion was appreciated by the coefficient of variation [(CV= SD/M)*100]. Friedman's ANOVA compared the three effort levels (W) simultaneously. The post hoc Bonferroni test was applied if statistically significant differences were found. The correlation was calculated using the Spearman-rho correlation coefficient with the magnitude of the correlation interpreted according to Pestana and Gageiro (2005). Data analysis was processed in the statistical software SPSS 19.0, and the adopted significance level was 5% (p≤ 0.05).
RESULTS
Table 1 shows the descriptive statistics values of the intensity at maximum lactate steady state (MLSS) and 4 mmol/L (AnT4) intensity when performing at the different incremental protocols. (step3min, step5min and step7min). By analysing the results, we can realise that the equivalent intensity with the concentration of 4 mmol/L was obtained through the protocol with 7 minutes steps (251.5± 35.72W) being the closest to the maximum lactate steady state of (246.5± 35.20W).
Table 1 External mechanical power (mean and standard deviation watts (W)) equivalent to maximum lactate steady state (MLSS) and intensity of 4mmol/L performing at the three different protocols (AnT4 step3min, AnT4 step5min and AnT4 step7min).
| MLSS | AnT4 step3min | AnT4 step5min | AnT4 step7min |
|---|---|---|---|
| 246.5± 35.20W | 277.3± 43.09W | 259.5± 41.30W | 251.5± 41.30W |
Figure 1 shows the correlations between the intensity values corresponding to the MLSS and the intensity values corresponding to 4 mmol/L (AnT4) obtained in the different incremental protocols.
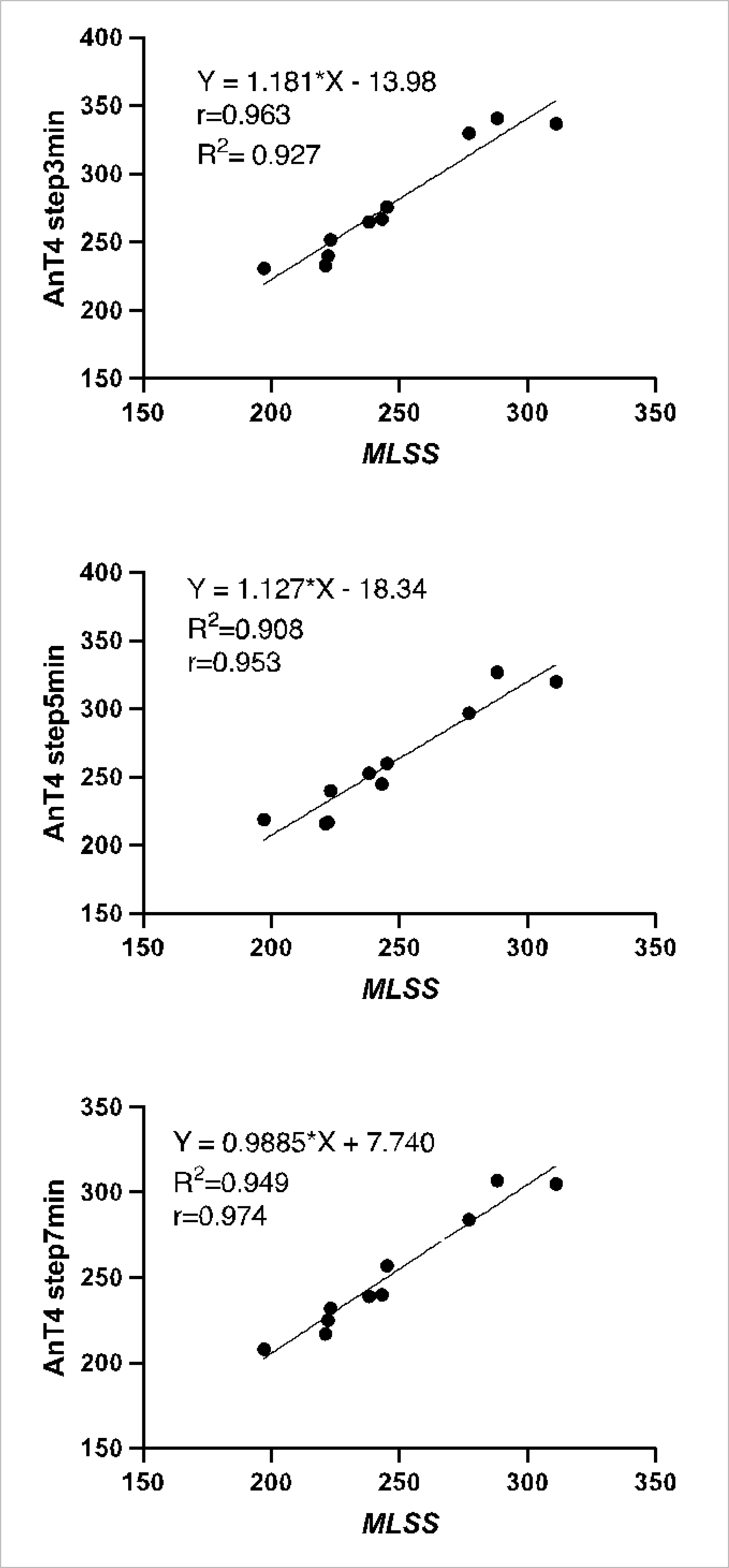
Figure 1 Correlations (r; R2) between maximum lactate steady state (MLSS) and intensity of 4mmol/L performing at different protocols (AnT4 step3min, AnT4 step5min and AnT4 step7min).
The correlation between MLSS and AnT4 calculated from the different duration step values is present in Figure 1, showing the high correlation values (r> 0.90; p< 0.001).
Table 2 shows that the simultaneous comparison, by Friedman's ANOVA, between the three levels of AnT4 effort resulted in significant differences (χ2= 17.897; p< 0.001).
Table 2 Mean Rank and Friedman's ANOVA in simultaneous comparison between the three recording moments of intensity of 4mmol/L performing at different protocols (AnT4).
| Mean Rank | χ2 | p | |
|---|---|---|---|
| AnT4 step3min (W) | 3.00 | 17.897 | < 0.001 |
| AnT4 step5min (W) | 1.85 | ||
| AnT4 step7min (W) | 1.15 |
The posthoc analysis with Bonferroni adjustment showed significant differences between AnT4 step3min (W) versus AnT4 step5min (W) and AnT4 step3min (W) versus AnT4 step7min (W), with values of p= 0.005. In both cases, due to the higher mean rank of ANT4 step3min (W). It should be noted that there are no significant differences between AnT4 step5min (W) and AnT4 step7min (W), revealing the sample's homogeneity at these levels of effort.
The mean value of lactate production corresponding to MLSS was 3.7 mmol/L with a standard deviation of 0.82 mmol/L.
Table 3 shows the heart rate values equivalent to MLSS and intensity of 4 mmol/L performed at the three different protocols.
Table 3 Heart rate values (mean and standard deviation of beat per minute (bpm)) equivalent to maximum lactate steady state (MLSS) and intensity of 4mmol/L performing at the three different protocols (AnT4 step3min, AnT4 step5min and AnT4 step7min).
| MLSS | AnT4 step3min | AnT4 step5min | AnT4 step7min |
|---|---|---|---|
| 173.7± 7.50 bpm | 170.0± 5.68 bpm | 168.4± 5.06 bpm | 169.0± 5.89 bpm |
DISCUSSION
A strong and very significant correlation between all step duration and the MLSS was found. Our results showed that the intensity equivalent to 4 mmol/L obtained through the protocol with 7 minutes steps (251.5± 35.72W) is the closest to that determined through MLSS protocol (246.5± 35,20W), showing a difference of 5W that contrasts with the difference of 31W obtained in the 3 minutes steps protocol.
Determining the step duration in the incremental protocol that produces the closest intensity to the MLSS is extremely important to increase the precision in training prescription, namely in lightweight rowers. This importance is reinforced by several authors who refer to the maximal power, the anaerobic threshold and the lean mass as the physiological characteristics that distinguish competitors’ success and failure (Gayer, 1994; Shephard, 1998).
According to several authors (Beneke, Hutler, Von Duvillard, Sellens, & Leithauser, 2003; Urhausen et al., 1993), the more appropriate method for determining the AnT is the MLSS. However, despite being the most suitable for assessing an athlete's endurance capacity (Billat, 1996), the MLSS protocol requires a long application, which could cause perturbance in the athlete's preparation. The use of an incremental protocol to determine the AnT based on fixed lactate concentrations is common. These faster and more economical protocols can be performed in any training period without significantly changing the training periodisation.
In addition, a high correlation between AnT4 and MLSS was found in several studies, except for the one realised by Schuylenbergh, Eynde and Hespel (2004). The intensity of 4 mmol/L in incremental tests appears to be higher than in the MLSS test (Faude et al., 2009).
However, it is essential to point out that different methodologies were applied in these studies, particularly the value of load from step to step. Limited by those different methodologies used, it remains for us to analyse them individually. Heck et al. (1985) found a strong correlation (r= 0.98) between AnT4 and MLSS during running and cycling.
Additionally, they observed that the speed and power corresponding to AnT4 were superior to MLSS. However, it is essential to note that this difference in power only occurred when using incremental protocols with 3 minutes steps. However, when using 5 minutes steps, the differences were no longer observed (Heck et al., 1985). Analysing the comparative study of several scientific articles compiled by Faude et al. (2009), it is crucial to analyse the results obtained by Beneke (1995) due to the specificity of the sample since they are rowers. This author used 3 minutes steps to determine the AnT4, getting an average power of 32W higher than in the MLSS test. Similar to Beneke (1995), our results also show a difference of 31W between AnT4 and MLSS when using 3 minutes steps, showing an overestimated power AnT 4mmolL.
In general, in compared studies, regardless of the duration of the steps, the AnT4 intensities overestimated the MLSS (Baldari & Guidetti, 2000). This result may be due to using a fixed concentration of 4mmol/L since studies compare different methods for determining AnT. The tests performed on cyclists (Cheng et al., 1992) and runners (Nicholson & Sleivert, 2001) should be highlighted, reporting that the intensities obtained using the fixed concentration method of 4mmol/L were higher compared to the remaining methods applied. Thus, overestimating the AnT. Given this situation, Figueira and Denadai (2004) suggested using a fixed concentration of 3.5 mmol/L of blood lactate as equivalent to AnT, justifying this choice due to the use of incremental protocols with steps of only 3 minutes to estimate the intensity of AnT correctly.
In summary, we can conclude that the literature is divergent both in conceptual aspects and in the methods for determining the AnT.
To define the incremental protocol with the most reasonable step, we compared the AnT4 intensity obtained through the three durations of steps and the MLSS. Analysing the results, referring to Bonferroni's posthoc, statistically, significant differences occur between AnT4 step3min (W) versus AnT4 step5min (W) (p= 0.005) and AnT4 step3min (W) versus AnT4 step7min (W), in both cases due to the higher mean rank of AnT4 step3min (W). It should be noted that there are no significant differences between AnT4 step5min (W) between AnT4 step7min (W), which shows the sample's homogeneity AnT these steps.
Focused on results, the protocol that uses 3 minutes steps does not represent the same lactic concentration obtained in the MLSS test, showing the difference of 31W obtained between the ANT4 and MLSS intensity. This conclusion contradicts many physiology laboratories that use protocols with durations between 3 and 5 minutes to test the AnT. These levels will even be considered adequate for measurements of ventilatory capacity and heart rate evolution. Still, according to Hahn et al. (2000), the duration will not be acceptable when the objective is to determine the intensity of the exercise corresponding to the AnT. Tests for determining lactate generally require longer steps than the ventilatory threshold tests, which could be partly explained by the differences between lactate in muscle and blood. Blood lactate is always lower than muscle lactate.
For this reason, when we use duration steps lower than 4 minutes, lactic muscle acidosis may be underestimated (Green, Hughson, Orr, & Ranney, 1983; Jacobs, 1986). Foster, Schrager and Snyder (1995) add that blood lactate may indicate intramuscular lactic acidosis. Still, a particular time is necessary for blood lactate to correspond to the maximum intramuscular lactate concentration because the diffusion of muscle-blood lactate is not immediate.
Our results do not show significant differences between the 5- and 7 minutes steps. However, if we compare the means, we can verify that the AnT4 obtained through the protocol with 7 minutes steps (251.5± 35,72W) is closest to the MLSS (246.5± 35.20W).
Several factors indicate the use of 7 minutes steps as being the most valid. Although the difference between the MLSS and the AnT with steps of 7 minutes is 5W and that of 5 minutes is only 9W, AnT the level of high competition, all details count, and this is a detail with great importance since minor physiological differences can correspond to major changes in training planning and control.
In the future, it would be relevant to test rowers on the field, evaluate the athlete on the boat, on the water or even as a team, and verify the impact of these conditions on the evaluation and determination of the aerobic competence of a rowing athlete.
CONCLUSIONS
In search of a more straightforward and less time-consuming test, we tried to determine which incremental protocol for anaerobic threshold (AnT) evaluation was best correlated with the maximum lactate steady state (MLSS). Our results allowed us to verify that the steps (step3min, step5min, and step7min) chosen to test the anaerobic threshold present a high correlation with the MLSS. However, due to the superior correlation with the MLSS, the proposal that emerges from this study defends the 7 minutes steps (step7min) as the most suitable for determining, through the AnT, the aerobic competence of a rowing athlete.

