











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
INTRODUCTION
Shoulder pain is a symptom that affects between 40 and 90% of competitive swimmers. Therefore, it characterises a special syndrome called “swimmer’s shoulder” due to the repetition of the gesture performed in an amplitude higher than 90° (Rouard & Clarys, 1995; McMaster, 1999; Sein et al., 2010). The symptom affects most of the swimmers. It initially starts with mild discomfort that remains during and after training, which ends up affecting the athlete’s progress (McMaster, 1999; Sein et al., 2010).
Bak (2010) proposes taking a break as a first tactic, cutting back on training and using an ice pack only when pain occurs during swimming. Another important tool is the coach’s analysis and technical corrections of the specific movement in this sport during training. Shoulder girdle stabilisation exercises, for example, are recommended for injury prevention in swimming athletes.
Glenohumeral joint stability is directly related to the correct muscular activation of the rotator cuff (infraspinal, subscapular, supraspinatus, minor round), which is essential for mobilisation, especially in swimming (Perry et al., 1992) due to being part of the muscles that generate propulsion to perform the stroke (Lauer, Figueiredo, Vilas-Boas, Fernandes & Rouard, 2013). Different researchers highlight the importance of instability and imbalance of the glenohumeral and scapular muscles as a secondary impact factor for this tendon. Other factors demonstrated are overuse of the joint, overload, bone configuration, the hypovascularisation of the supraspinatus tendon, lower flexibility levels, inefficient swimming technique, coach errors, and level of training (Fernández, Aravena, Verdugo, Galaz & Rex, 2010).
Swimming training is also known to lead to muscle imbalances between the internal and external rotators of the shoulder (Batalha, Raimundo, Tomas-Carus, Barbosa & Silva, 2013). However, the activities that induce changes in the biomechanics of the shoulder and tissue injuries are not fully understood. Most of the research was carried out on swimmers already injured, and the results interfered with developing prevention programs (Tovin, 2006). Clearly, high-performance swimming athletes must complete a series of on-land exercises to avoid possible injuries. Different clinical examinations are described in the literature to help evaluate shoulder injuries (Gismervik, Drogset, Granviken, Rø & Leivseth, 2017). These exams tend to demonstrate certain types of symptoms and specific signs, which reinforce the diagnosis of the shoulder that presents some type of pain, rupture, and instability.
In young people, injuries are likely to occur around the age of 13 (Sein et al., 2010). Thereby, although little studied, evaluating and proposing preventive exercises for young swimmers is a relevant topic. This is important as it will allow athletes to stay longer in the sport and improve their performance. Preventive exercises, description of shoulder injuries and weaknesses of child swimmers are very important topics for research.
Thus, the reason for this study is based on some authors who recommend a muscle-strengthening program to keep the shoulder healthy and avoid fatigue and shoulder injuries (Bak, 2010; Tate et al., 2012). In addition, evaluations of muscle activation, such as through surface electromyography, can address the requirements of the main muscles involved (Hug, 2011). There is evidence in the literature applied to swimming (Martens, Figueiredo & Daly, 2015) but little information on muscle activation for child swimmers. Thus, the aim of this study is to assess the effectiveness of a 12-week intervention program on muscle pain and the evaluation of the MVC. It was hypothesised that pain levels would decrease and the electrical activity profile would differ after 12 weeks of intervention with rehabilitation exercises.
METHODS
Participants
Twelve competitive swimmers volunteered for this study (Table 1). Based on the results provided by the Pain Intensity Scale, The swimmers were separated into two groups: the shoulder pain group and the control group (without shoulder pain). The athletes swam approximately 30,000 m per week (6 times/week) during the week’s training sessions. The swimmers had at least 2 years of national and international competitive experience (competition experience mean was 2.8 ± 0.8 years) and trained normally during the data collection (6 ± 1 days) period (13 to 30 km of volume per week). The competitive swimmers were from Paysandú City and were aged between 10 and 12 years.
Table 1 Characteristics of infant swimmers. They were divided in two groups: shoulder pain and control group.
| Shoulder Pain Group (6) | Control Group (6) | |
|---|---|---|
| Age (years) | 11.2± 1.1 | 11.2± .9 |
| Mass (kg) | 46.44± 7.82 | 39.76± 8.96 |
| Height (m) | 1.49± .09 | 1.47± .06 |
| Arm Span (m) | 1.50± .10 | 1.45± .04 |
| Male/Female | 1/5 | 1/5 |
This study was conducted in the first training cycle (6 weeks) of the training season. All swimmers were in the base training period and performed 30 training sessions before the protocols. Swimmers were informed of the benefits and risks of the investigation before signing an informed consent form approved by the institution to participate in the study. In addition, the swimmers’ parents or guardians provided written consent. The study was approved by the Ethics Committee of Universidad de la Republica Uruguay. All the procedures were in agreement with Helsinki’s declaration regarding research in humans.
Protocol
The evaluations were divided into three different times: pre, post and detraining. The first evaluation was conducted before the beginning of the intervention. The first evaluation test was composed of: i) measurement of anthropometric characteristics; ii) clinical examination (composed of five tests); iii) EMG evaluation (MVC — maximum voluntary contraction by 11 muscles). In the second and third evaluations, clinical examinations and EMG evaluations were performed.
The intervention with preventive exercises lasted 12 weeks and was performed twice a week for 50 min. In all sessions, the initial part consisted of mobilising the shoulder girdle and, in the end, stretching all the muscles involved in the movements.
The exercises consisted of muscle strengthening with elastic bands and scapular stability exercises. Periodisation was carried out (every two weeks) between exercise periods. The main variable that oscillated was the stability of the exercises, requiring greater control of the athletes’ shoulder girdle. All sessions and evaluations were conducted by a physical education teacher and a physiotherapist, which previously prepared for the exercises.
After the preventive exercises (12 weeks), the athletes were re-evaluated in five clinical examinations and in the EMG evaluation. At the end of the study, the athletes did not continue with the exercises, therefore, 12 weeks after the end of the preventive exercise sessions, the athletes were re-evaluated.
Measures
Clinical examination and pain intensity
Five clinical tests were performed: i) Hawkins-Kennedy for subacromial impingement and the supraspinatus (Hawkins & Kennedy, 1980); and four tests for determining the location of the rotator cuff lesion: ii) Lift-off test to evaluate the integrity of the subscapularis muscle (Hermans et al., 2013); iii) Jobe to evaluate the supraspinal muscle tendon (when positive it is an indicator of tendinitis and/or ruptures) (Chew, Pua, Chin, Clarke & Wong, 2010); iv) Patte’s test to evaluate the infraspinatus tendon (Leroux, Thomas, Bonnel & Blotman, 1995); v) palm-up test to evaluate long biceps bite (Gismervik et al., 2017; Leroux et al., 1995; Michener, Walsworth, Doukas & Murphy, 2009).
The Faces Pain Scale, a self-report instrument used to assess children’s pain intensity (Hicks, von Baeyer, Spafford, van Korlaar & Goodenough, 2001), was used. It was positioned in different places around the data collection areas, and the athletes were asked about the intensity of the pain before and after the tests (Figure 1). To participate in the group of controls, it was necessary not to feel pain in both shoulders (pain scale equal to zero). To participate in the group of athletes with pain, it was necessary to have pain in at least one of the shoulders. Based on these results, the athletes were divided into two groups: the shoulder pain group and the control group. The data were transcribed to a spreadsheet and presented with average and standard deviation.
EMG data
Electromyography data was collected through a Delsys® data acquisition system. The equipment has 16 channels with a sampling rate of 2000 Hz. Surface electrodes for each muscle evaluated were used: trapezius superiores (TS), trapezius inferiores (TI), rhomboideus major (Rm), infraspinatus (IS), teres major (ReM), latissimus dorsi (LD), serratus anterior (SA), pectoralis major (sternocostalis) (PM), deltoideus anterior (DA), biceps brachii (caput longum) (BB), triceps brachii (caput longum) (TB).
The electrodes were placed on the muscle belly, parallel to the muscle fibres. All skin cleaning and abrasion care were performed. For the assessment of electromyographic activation, isometric MVC was performed for each of the 11 muscles, following the positioning suggested by Konrad (2005). EMG measurements were taken on the shoulder that presented pain. If the athlete had pain in both shoulders, the measurement was performed in the shoulder with the highest level of pain according to the pain scale. For the control group, the measurement was taken on the dominant side.
For the analysis, filtering and processing of the electromyographic signals were performed by a bandpass filter Butterworth, third order, with cut-off frequencies between 20 and 500 Hz. Then the calculation of the root mean square value (RMS) during three central seconds of the MVC contraction of each muscle (Winter, 2005) data are in millivolts (mV).
Statistical analysis
All values are expressed as mean ± standard deviation (SD). After assessing the normality and homoscedasticity, the researchers compared the anthropometric characteristics between groups by the unpaired t-test based on Kolmogorov-Smirnov, Levene tests and skewness values. Clinical examination and EMG data were compared with repeated-measures ANOVA. When suitable, multiple comparisons were made with Bonferroni correction. Alpha was established at 0.05, and all analyses were carried out using the Statistical Package for Social Sciences (SPSS 27.0, IBM, Armonk, NY, USA).
RESULTS
Table 2 shows the clinical examination results. The pain group presented lower pain intensity values in post intervention program. For most of the variables (Hawkin test right, Hawkin test left, Patte test left, Palm up test right, Palm up test left, Jobe test left, Gerber test right, Gerber test left), after the training program and until the detraining evaluation, the pain intensities presented higher values with statistical significance. Finally, some cases (Hawkin test right, Hawkin test left, Palm up test right and Gerber test right) had higher pain intensities in detraining compared to baseline. However, most tests showed lower values in detraining compared to baseline. After the intervention, the pain levels decreased significantly in five tests.
Table 2 Clinical examinations results.
| Pain group | Control group | |||
|---|---|---|---|---|
| Pre PE | Post PE | Detraining PE | Pre PE, Post PE, Detraining PE | |
| Hawkin test right | 1.17± .9 * | .15± .37 § | 1.26± .88 | _ |
| Hawkin test left | .71± .32 * † | .30± .75 § | 1.05 ± .55 | _ |
| Patte test right | .80± 1.03 | .76± 1.53 | .5± .75 | _ |
| Patte test left | 1.2± 1.10 * † | .15± .37 § | .85 ± .65 | _ |
| Palm up test right | .33± .94 * | .30± .75 | .65± .75 | _ |
| Palm up test left | .56± .87 * | .32± .55 | .70 ± .35 | _ |
| Jobe test right | .88± .93 * | .92± 1.03 | .85± .75 | _ |
| Jobe test left | 1.12± 1.03 * † | .34± .75 § | .85 ± .65 | _ |
| Gerber test right | .75± .55 | .31± .55 | .80± .85 | _ |
| Gerber test left | 1.05± .97 * † | .54± .37 § | .95± .70 | _ |
Right: referring to the right shoulder; Left: referring to the left shoulder. Infant athletes with shoulder pain, control group (without shoulder pain); Pre PE: clinical test pre preventive exercise; Post PE: clinical test post preventive exercise; Detraining PE: clinical test in detraining period. Control group: - - - no present pain (results);
*significant difference between Pre PE and Post PE;
†significant difference between Pre PE and detraining PE;
§significant difference between Post PE and detraining (P> 0.05).
In the comparison of muscle strength between groups, the control group presented higher values for TS, TI, Rm, IS, ReM, LD, SA, PM, DA, and TB., with a difference p< 0.05.
Figure 2 shows the EMG data for MVC for each evaluated muscle in the shoulder pain group in three evaluations: pre preventive exercises, post preventive exercise and detraining. The TS and TI presented lower activity in the post preventive training phase. The TI presented lower activation during training. Rm, IS presented higher activity in the post preventive training phase. ReM, SA presented higher activity in the post preventive training phase compared to the pre-training phase. PM presented greater electrical activity in the phase before preventive training compared to post and detraining. DA presented greater activation in the post-training phase when compared to pre- and detraining.
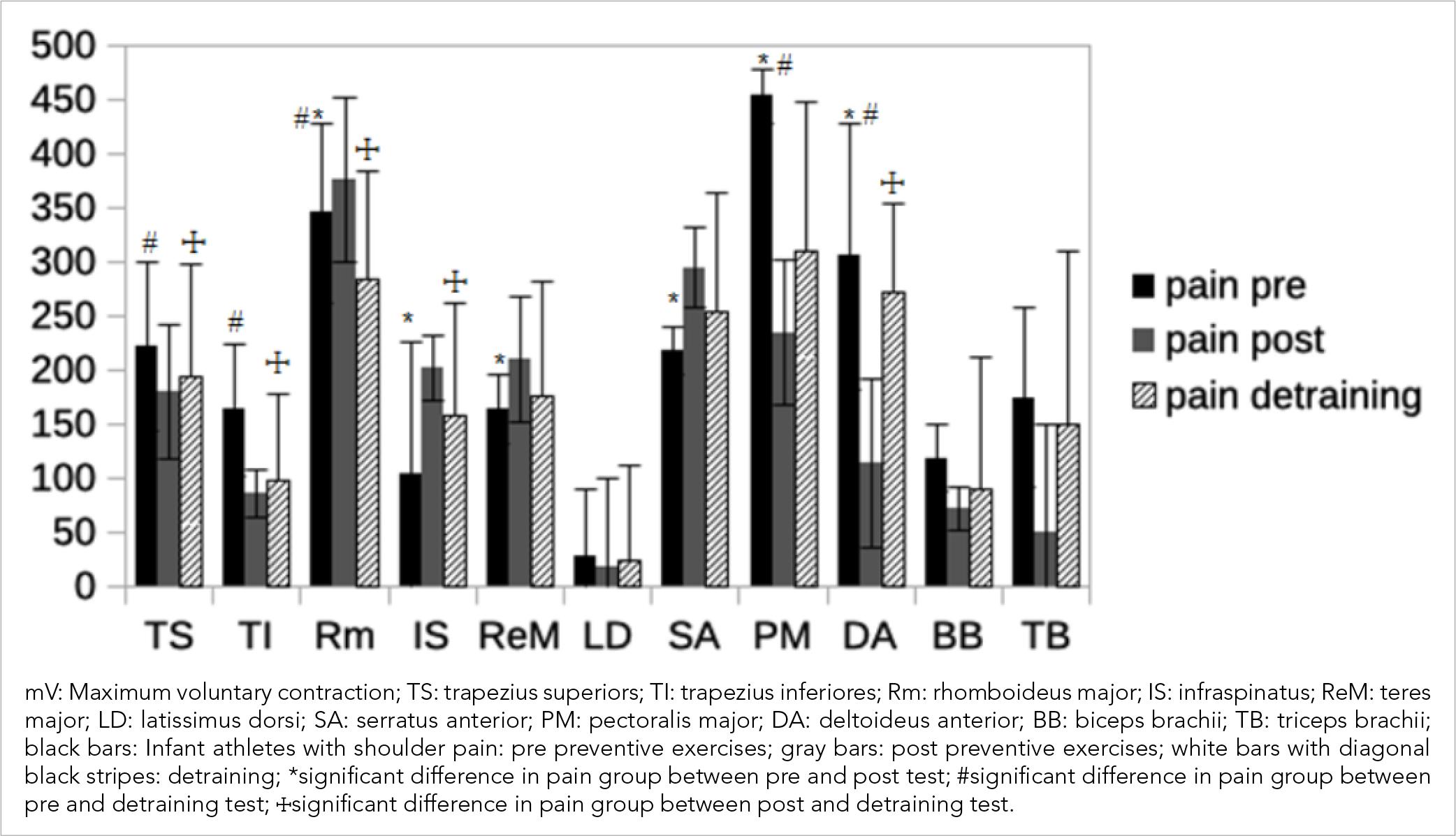
Figure 2. EMG data for MVC in the shoulder pain group in three evaluations: pre preventive exercises, post preventive exercise and detraining.
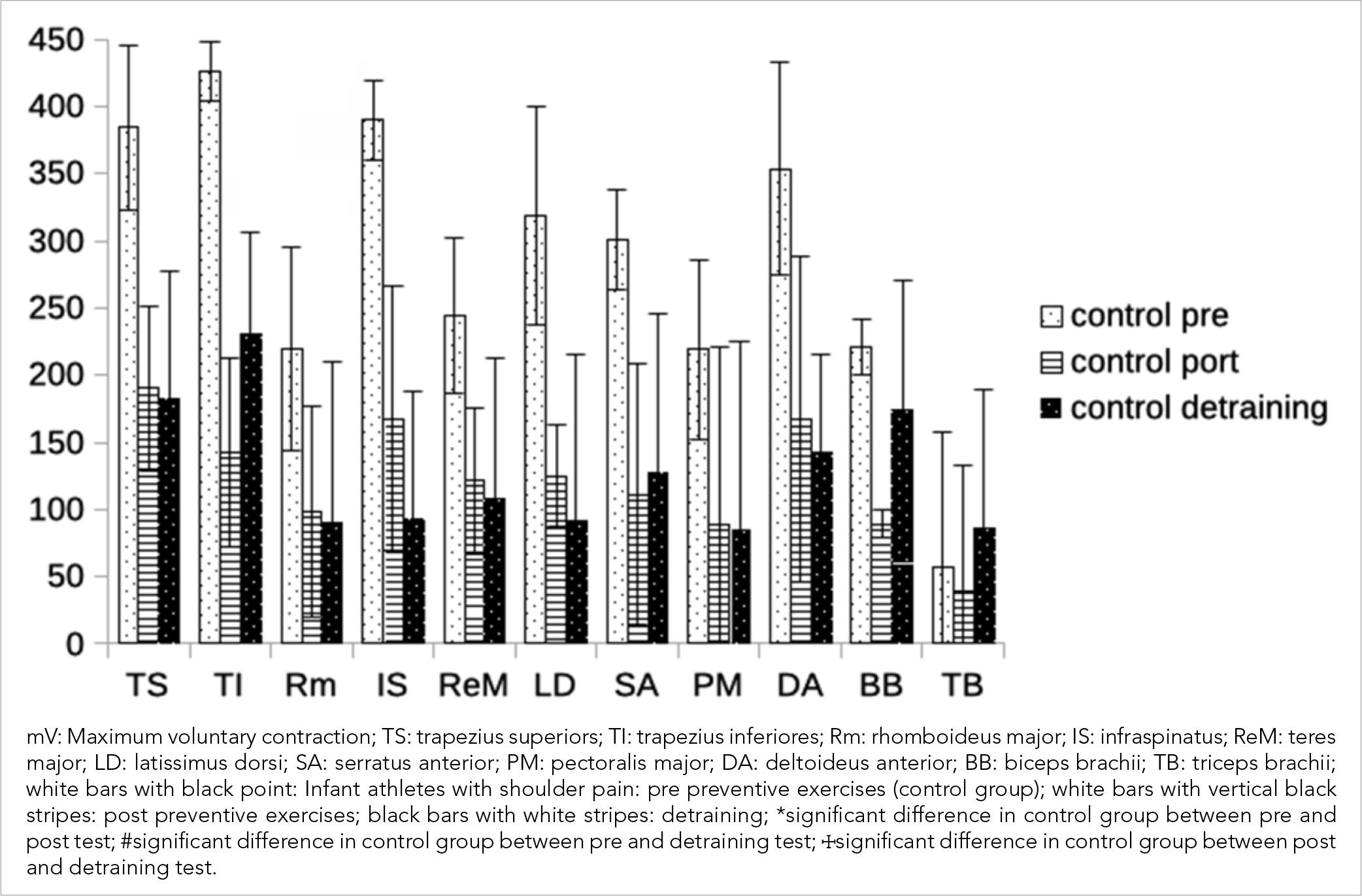
Figure 3 shows the EMG data for MVC in each evaluated muscle in the control group in three evaluations: pre preventive exercises, post preventive exercise and detraining. The TS and ReM presented greater activity in the pre-preventive training phase when compared to the post and detraining phases. TI presented higher values in the pre phase compared to the post and detraining phases. Rm, LD, SA, and DA presented higher activity in the pre phase compared to post preventive training. IS presented higher values of electrical activity in the pre phase compared to the post preventive training and also in relation to the post and detraining. BB presented lower values of electrical activity in the pre phase compared to post preventive training and also in relation to post and detraining. TB presented lower values in the post preventive training phase.
DISCUSSION
The purpose of this study was to assess and compare the electrical activity of the shoulder muscles and the pain scale in child swimmers before and after specific muscle strengthening. This study demonstrated electromyographic activation in various muscles that contribute to swimming movement and shoulder girdle stability. The results show that the researchers’ hypothesis was accepted.
The first evaluations (muscular pre-strengthening) revealed differences in the average RMS value (mV) for the muscles: IS, ReM, LD, SA, and PM between the two groups (with and without pain). The group without pain showed greater electrical activation in most muscles, however, the group with pain presented higher electrical activation in the PM. According to the activity of the muscles involved in the movement of the shoulder girdle movement in swimming, the PM performs internal rotation and adduction of the arm (with the rib cage as a fixed point), this movement being the most harmful in the evaluated sports gesture. Activating the PM more than the other muscles (performing external rotation) results in a load that is too great for the stabilising muscles (rotator cuff) to bear, potentially resulting in injuries such as subacromial impingement syndrome and tendon rupture of these muscles (Batalha et al., 2013; Calais-Germain, 1999). As a result, the IS, ReM, and LD muscles, which allow stabilisation and prevent forward and backward displacement of the head of the humerus, act weakly, failing to perform their function of shoulder joint complex stabilisation. As the SA, when active, keeps the inner edge of the scapula close to the thorax, decreased or under activated muscle activation moves the scapula away from the thorax (with abduction and external belling of the scapula), causing overload to the acromioclavicular joint and scapulohumeral instability (Batalha et al., 2013).
Regarding post-muscular strengthening, significant differences in the average RMS value (mV) in the muscles TS, Ti, and Rm were found in both groups (with and without pain). The pain group had a significant difference in the average RMS value (mV) in the muscles Rm, IS, ReM, SA, PM, and DA before and after muscle strengthening. The serratus anterior is one of the most important shoulder girdle muscles in those who had Rm, IS, ReM, and SA more activated after specific muscle strengthening. Without it, the arm cannot be raised above the head because the trapezius does not produce enough superior rotation for complete abduction (Oliveira et al., 2007). If the trapezius (TS) and serratus anterior (SA) muscles are not activated properly, the scapula loses its most important stabilisers, and its position is determined primarily by the weight of the arm acting on the tip of the arm shoulder. When working with the upper limb in suspension, the upper trapezius (TS) is frequently overworked.
Because the middle adductor trapezius works in tandem with the (SA), (Abductor), these two muscles stabilise the shoulder blade in any upper-limb force action (Calais-Germain, 1999). This considers the fact that the SA was activated by others, resulting in its strengthening as a result of the specific training proposed. Furthermore, due to the repetition of movements in swimming, some of the muscles of the shoulder joint complex tend to weaken and must be strengthened to avoid injury. As there are muscles in the shoulder and waist scapular muscles that have greater electrical activation, this can result in an imbalance of forces acting on the shoulder joint complex. The Rm is in charge of scapula adduction and internal belling (Novotny et al., 2017).
The greatest activation was evidenced in the post-muscular strengthening in the pain group, which is important for generating scapular stabilisation and control and allowing the motor gesture of the sport with a lower risk of injury (Vanderstukken, Borms, Berckmans, Spanhove & Cools, 2020). In addition, there was an increase in the activity of the IS and ReM that participate in the rotator cuff and generate external rotation of the humerus, an important action due to the weakness commonly found in this muscle in swimmers, which can result in scapulohumeral joint injuries (Walker, Gabbe, Wajswelner, Blanch & Bennell, 2012; Ben Kibler, 1998). Along with SA, these muscles showed changes (higher mean RMS value in the CVM after muscle strengthening). Strengthening resulted in increased electrical activity of the rotator cuff muscles, which act as humeral mobilisers and develop action of the scapulohumeral joint active ligaments (Calais-Germain, 1999; Voight & Thomson, 2000).
Most muscles were less activated in the pain-free group, as well as the TB. The decrease in the average RMS value of the CVM in this group can be attributed to improved motor control following the training period (Beck et al., 2009). Physical exercise, such as those proposed in this study, can result in increased muscle activation efficiency and economy. Regarding the need to recruit motor fibre, choosing what is needed for exercise can reduce exhaustion and improve athletes’ functional performance (Abreu, 2019). To confirm these findings, different analyses and measurements of other movements (besides CVM) are necessary. Athletes without pain remained pain-free after muscle strengthening, which, along with decreased pain in the pain group, was a significant finding in this study. It is recommended a good specific muscular reinforcement of the stabilising muscles of the scapula, a correct position of the scapula, not allowing excessive abduction or external belling of the scapula so that athletes can continue training and remain with a greater chance of success in this sport, such as the children who participated in this study.
Other strategies used in the study included clinical examinations such as the “Hawkins” test that evaluates the impact, the “Lift-off test” that evaluates the Subscapularis muscle, the “Jobe” test that evaluates the supraspinal muscle, the “Patte’s” test that evaluates the infraspinatus, and the “Palm up test” that evaluates the long head of the biceps. Regarding the results obtained from the aforementioned tests, it was possible to collect data on the athletes who presented some type of pain and those who did not, as well as the intensity of pain before, during, and after the tests. Statistics that account for the differences between them were obtained: Patte’s (left shoulder), Hawkin (right-left shoulder), Palm up (right-left shoulder), Jobe (right-left), and Lift-off tests (left shoulder). The group that was in pain before the specific training had their pain decrease the same way after the proposed weeks of training, as shown in the post-test evaluations. It is necessary to propose a muscle strengthening plan for those muscles prone to weakness to keep them stable. It is also important to strengthen muscles that tend to be stronger or work harder on shoulder movements so they stay healthy (Oliveira et al., 2007).
In order to continue this research, the signals may be evaluated during a simulation of a land-based stroke with resistance from an elastic band. Following the analysis, the percentage in relation to CVM will be calculated. A limitation of this research was the reduction of training and intensity, as the children who complained of pain had an increase in the first weeks due to the lack of habitual adaptation to ground training. Otherwise, our expectations were met with success. Additionally, similar studies with more participants are strongly recommended.
CONCLUSIONS
Regarding the average RMS value (mV) in the muscles TS, TI, RM, IS, ReM, LD, SA, and PM, there was a difference between the two groups (with pain and without pain) in the pre and post muscle strengthening evaluations. The maintenance of resistance capacity, muscle strength and elasticity, and joint flexibility, in a way, protects the shoulder joint by maintaining its physical condition, allowing swimmers to correctly use the superior member without daily activities representing an overload to the joint.
The improvements obtained with muscle strengthening exercises were demonstrated in the Hawkin test, Palm up test, Jobe test, and Lift-off. The differences in the pre and post evaluations indicate that the intervention proposals were effective because there was a decrease in shoulder pain in the group with pain in Patte’s (left shoulder), Hawkin test (right-left shoulder), test Palm up (right-left shoulder), Jobe test (right-left), and Lift-off (right-left). It can be concluded that muscle strengthening work is highly recommended, as it improves the swimmer’s shoulder performance, reducing injuries and decreasing the intensity of the pain.

