











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
Permalink
INTRODUCTION
In sports, injury prevention is a primary concern for teams and clubs’ technical committees and health departments, not only because of the damage caused by the athlete’s distance itself but also because of the high costs arising from the underlying treatments (Neves et al., 2016; Viegas et al., 2020). Considering this point of view, especially in high-performance sports activities, there is great interest in technical committees in facilitating and cheapening the process to identify possible future injuries of an athlete through the technology available today (Santos Bunn, 2020).
Thereunto, there are several direct or indirect indicators of the possibility of injury that can be used to monitor the health status and physical strain of athletes, such as measuring enzymes present in the bloodstream — lactate dehydrogenase (LDH), troponin I, myoglobin, and creatine kinase (CK-MM) — verification of maximum voluntary action, ultrasonography, tomography, surface electromyography, magnetic resonance, muscle biopsy, thermography, observation of subjective pain perception scale, also represented by delayed onset muscle soreness (DOMS), among others (Andrade Fernandes et al., 2017a).
The CK, in its muscular form, is an objective measure. However, it can only be accessed through the blood, not allowing for a precise locate the injured structure. In this sense, the combination of indicators that will enable objective and subjective measurements have been recommended, and several studies have pointed out the use of thermography for this purpose (Andrade Fernandes et al., 2017b; Júnior et al., 2021; Neves et al., 2015; Neves et al., 2016; Priego-Quesada et al., 2020).
In case of suspicion of musculoskeletal injury, imaging tests (ultrasound, tomography, surface electromyography, magnetic resonance imaging, among others) have been the main choice for confirming the diagnosis. However, they are costly methods to be maintained periodically, in addition to not being portable and emitting excessive ionising radiation, which is harmful to health. Therefore, a solution to promote the optimisation of this process is the use of thermography. It is a tool that obtains infrared images through cameras capable of measuring the surface temperature of the body’s skin, indicating an accelerated metabolic activity in some areas of the body, which may show the location of sites with a high chance of developing lesions (Andrade Fernandes et al., 2017a). The advantages are vast compared to other imaging techniques: safety, non-contact, non-invasive, painless, no ionising radiation, no side effects, no contraindications, and efficacy (Viegas et al., 2020). Researchers have, therefore, been successful in the combined use of physiological indicators to prevent injuries. If, on the one hand, high serum CK levels indicate the possibility of injury in any body area, thermography allows locating this area so that, consequently, a prevention protocol can be adopted (Andrade Fernandes et al., 2017b; Júnior et al., 2021; Kennedy et al., 2017; Neves et al., 2015; Neves et al., 2016; Priego-Quesada et al., 2020).
However, the literature doesn’t clarify whether the variation shown in skin temperature is associated with indirect blood markers of muscle damage, as some studies find an association (Andrade Fernandes et al., 2017a; Andrade Fernandes et al., 2017b; Júnior et al., 2021) and others do not (Bandeira et al., 2012; Kennedy et al., 2017). Knowing the magnitude of the associations between CK and thermography would support a more scientific, practical, and efficient application to prevent injuries in physically active subjects. In this sense, it can be questioned whether an eventual direct replacement of the CK assessment (invasive method) by the thermal image assessment (non-invasive method) would be possible? Or whether both should be used in a complementary way?
Thus, this study aimed to investigate the association between thermal variation identified by thermography and muscle CK values in healthy subjects from a systematic review with meta-analysis. A null hypothesis (h0) assumed that there was no association between thermal variation identified by thermography and muscle CK values.
METHODS
Protocol and registration
The protocol for this study was registered in the International Prospective Register for Systematic Reviews (PROSPERO) under number CRD42021262109.
Eligibility criteria
The PRISMA 2020 (Page et al., 2021) recommendations were followed in this systematic review with meta-analysis, and the PIRT (WHO, 2014) strategy was used to construct the research question and search for evidence. Therefore, diagnostic accuracy studies with the following characteristics were included: Participants/Patients (healthy subjects); Index Test (thermography); Reference Test (CK collection); Target Condition (having analyzed the results of the Index and Reference Test).
Regarding the researched reports, searches were carried out for scientific articles published in renowned journals and periodicals from 2000 to 2021 in English, Spanish and Portuguese, considering, therefore, that the use of thermography technology is of recent application in the sports world and there was a significant evolution in the quality of the cameras used. Furthermore, studies found in duplicate were removed, and articles involving animal tests were not listed.
Information sources
In June 2021, searches were performed in the SCOPUS, MEDLINE, and Web of Science databases in the Instituto Militar de Engenharia (IME) library. As for the articles not available for free in the download tools, the author was contacted via e-mail to request the sharing of the content, and additional studies were manually included based on the searched reference lists.
Search strategy
The search was performed in the SCOPUS, MEDLINE, and Web of Science databases using the English terms “thermography” and “creatine kinase (CK)”, with their respective variations shown in Table 1 below. The descriptors in question were obtained using the MeSH, and DeCS platform, as well as other synonymous terminologies found in the literature were added. In addition, Boolean operators (delimiters) were used to search the databases: “OR” for synonymous descriptors and “AND” for the association of different descriptors, as shown in Table 1 below.
Table 1. Literature search strategy#.
| [Thermography | [ Creatine Kinase, MM Form | |
|---|---|---|
| OR Temperature Mapping OR Mapping, Temperature OR Mappings, Temperature OR Temperature Mappings OR Thermal imaging * OR Thermal image * OR Infrared imaging * OR Infrared images * OR Skin temperature *] |
AND | OR Creatine Kinase, M OR Creatine Kinase, MM OR Creatine Kinase, Muscle OR Kinase, M Creatine OR Kinase, MM Creatine OR Kinase, Muscle Creatine OR M Creatine Kinase OR MM Creatine Kinase OR Muscle Creatine Kinase OR ADP Phosphocreatine Phosphotransferase OR ATP Creatine Phosphotransferase OR Creatine Phosphokinase OR Macro-Creatine Kinase] |
# The terms were removed from the DeCS/MeSH descriptor search tool, except those marked with an asterisk.
Selection process
The identification of the works was carried out by reading titles and abstracts that showed relationships of variation between skin temperature and the biochemical marker creatine kinase (CK). The number of files identified in each database was recorded, and files that weren’t related to the topic sought or marked as ineligible by automation tools, or presented in the form of duplicates, were removed.
The files selected in the initial identification were read in their entirety to carry out screening, eventually excluding articles with no specific relationship with the topic or that didn’t have versions in the chosen languages or weren’t available. The reports approved in this screening comprise the study scope of the systematic review. In turn, the studies that exclusively presented some type of statistical association with their respective correlation coefficient “r” specifically on the descriptors of the topic in question compose the studies retrieved for the meta-analysis. Scientific articles identified through other reliable sources were included in the scope of the work. The numerical values from the selection process were explained in a flowchart following the PRISMA 2020 recommendations (Page et al., 2021).
Data items and collection process
Three independent collaborators conducted the data collection process: two of them were responsible for the search and selection process of the separate primary studies (T.M.S and E.B.N). The other was responsible for the statistical elaboration of the meta-analysis (P.S.B). After completing the study selection process and eliminating duplicates, the first two reviewers compared the obtained results and proceeded according to the articles’ eligibility criteria and quality assessment. After that, all indicators (characteristics of the samples, the intervention methods used, the regions of interest (ROI) analyzed by thermal imaging, the results obtained, and the conclusions) were used to analyse the studies that make up the scope of work were spreadsheet. The third collaborator, in turn, compiled statistical data for the work based on articles that exclusively presented the modalities of statistical association with their respective Pearson and Spearman correlation coefficients and used the Statsdirect tool (version 3.0) to produce the meta-analysis result graphs.
Quality assessment of studies
At this stage, the assessment of the methodological quality of the included studies was performed using the QUADAS-2 (Whiting et al., 2006) method to assess the risk of bias and applicability concerns of each study based on four domains: patient selection, index test, reference test, and timing, enabling the verification of the impact of the results of each study and how they will influence the discussion and conclusion of the systematic review and meta-analysis. For the applicability concerns the domains “sample selection”, “test-index”, “reference standard” are the parameters evaluated.
Effect measures and synthesis methods
According to the meta-analysis, the indices and statistical correlation coefficients used to synthesize or present results were evaluated using the Hedge-Olkins Fixed Effects method. Thereunto, regions of interest and temporal flow of measurement were analyzed for each correlation coefficient. Data were analyzed according to combinations of study results and trends obtained in the meta-analysis, observing their respective consistency measures (I2, for example) (McNeish & Kelley, 2019).
RESULTS
The PRISMA flow diagram of the included studies is depicted in Figure 1 below. In Figure 1, it can be seen that 482 files were identified in the databases, and another one was obtained by manual search. After reading the titles and abstracts, 386 duplicates were excluded. Another 65 records marked as ineligible by automation tools (search filters) were removed from areas of knowledge and articles older than the year 2000. In addition, of the remaining 31 articles, another 15 were removed for not specifically addressing the topic sought and another four for not having a full version in English, leaving 13 reports evaluated as eligible to be included in the scope of study of the systematic review. Of the 13, only five had a correlation coefficient “r” referring to the topic and, therefore, were included in the meta-analysis.
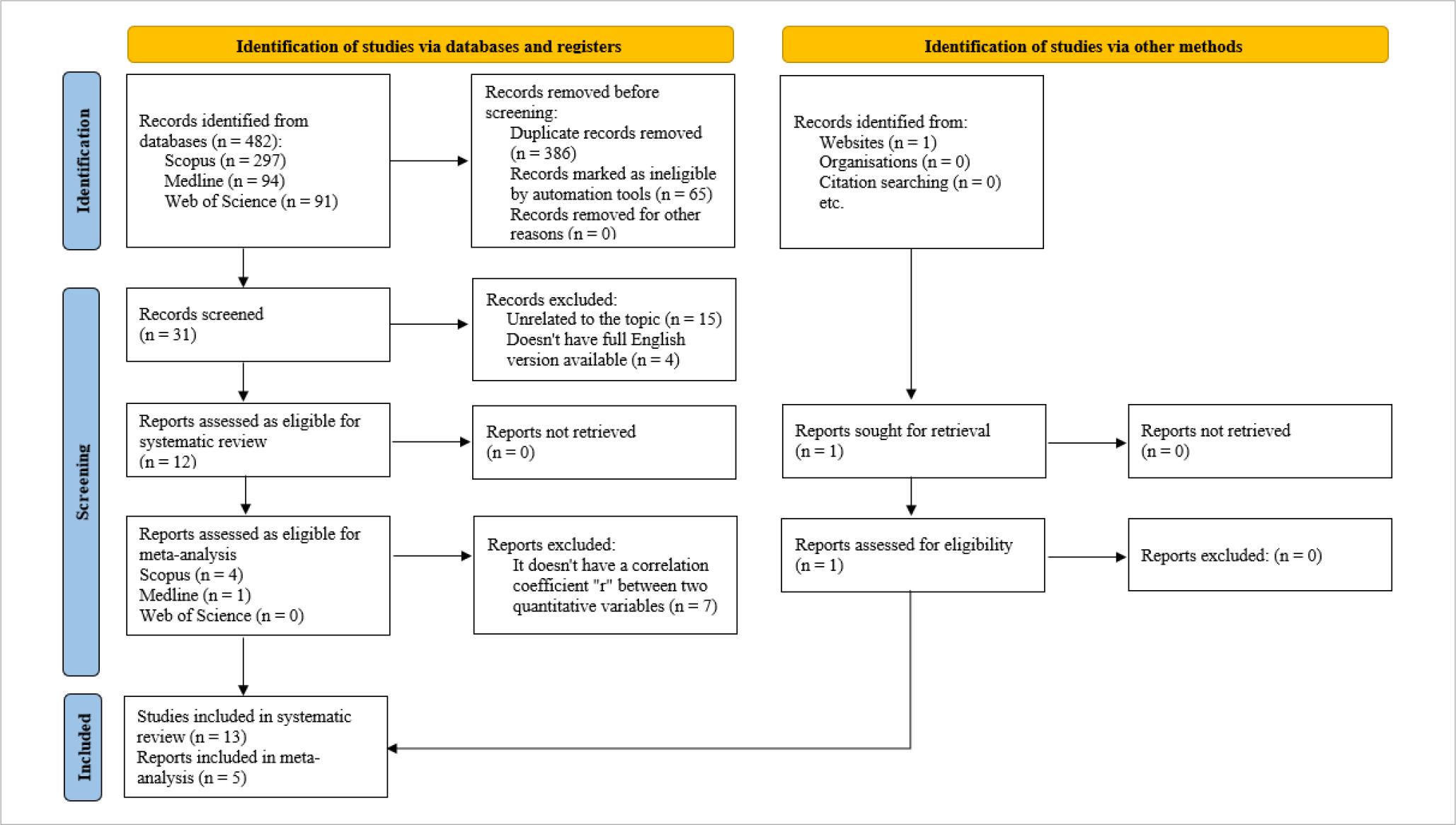
Figure 1. Flow diagram of the studies included in this systematic review with meta-analysis regarding the association between CK and thermography.
The characteristics of the 13 studies included in the systematic review are presented in Table 2, which details the characteristics of the samples, the intervention methods used, the regions of interest (ROI) analyzed by thermal imaging, the results obtained, and the conclusions.
Table 2. Association between thermography and CK: Systematic Review.
| Bibliographic Reference | Sample | Intervention Method | Region of Interest (ROI) analyzed by thermal imaging | Results | Conclusion |
|---|---|---|---|---|---|
| Júnior et al. (2021) |
Elite Male Football Players n= 20 age: 25.6± 4.0 |
An evaluation session was carried out before and another session after the competitive football season (16 weeks). In both sessions, blood collection was performed, evaluation of skin temperature asymmetry (Tsk) using infrared thermography (IRT) and evaluation of force asymmetry through the countermovement test (CMJ). | Anterior and posterior views of the lower limbs. | There were significant increases in Tsk (p < 0.03) and CK (p = 0.0001) even after a 3-day rest interval (no training). | CMJ testing can be combined with infrared thermography to monitor force asymmetry and help prevent muscle damage. |
| Carvalho et al.* (2021) |
Healthy male athletes from a professional football club n= 22 age: 27.7± 3.93 |
Athletes were followed in 19 national championship matches, with an interval of 7 days between matches. In each match, athletes used a GPS device to collect performance data. 48 hours after each match, each athlete’s perception of recovery, fatigue, and pain was documented, blood was collected for CK analysis, and infrared thermography was applied. | Anterior and posterior incidences of the lower limbs, which were divided into seven regions of interest (ROI), totalling 14 anterior ROIs and 14 posterior ROIs. | No correlation was observed between mean skin temperature and blood CK levels, pain level, perception of recovery, and perception of fatigue (r< 0.2, p> 0.05). | Infrared thermography didn’t correlate with CK level, pain, perceived fatigue or recovery, nor with performance variables within the field. |
| Barros et al. (2020) |
Healthy male athletes not using inappropriate ergogenic supplements and not in rapid weight loss programs n= 10 age: 22.50± 2.84 |
All athletes underwent three resistance training (RT) methods: traditional, tension and occlusion training. Torque peak, fatigue index, blood sample, thermal images and pain perception were measured immediately before and after the training session and 24 h and 48 h after. | Anterior and posterior views of the thighs. | Thermographic analysis revealed a reduction in skin temperature on both thighs after the tension (−9.37%) and vascular occlusion (−6.01%) methods. Only the vascular occlusion method showed an increase in CK (p< 0.001; ɳ2p= 1.08) and lactate dehydrogenase “LDH” (p< 0.001; ɳ2 p= 1.56). | An RT session with blood flow restriction (vascular occlusion method) increases plasma levels of CK and LDH, increases the subjective perception of muscle pain, and decreases peak muscle torque and skin temperature. |
| Pérez-Guarner et al.* (2019) |
Male and female amateur runners n= 11(M) n= 6 (F) age: 41± 6 |
Runners were measured 24 h and 48 h before and 24 h and 48 h after running a half marathon. The tests included obtaining blood markers, perception of pain and fatigue, skin temperature and jumping performance. | Anterior and posterior incidences divided into 10 zones (chest, anterior upper limbs, dorsal back and posterior upper limbs, abdominal, back and lumbar buttocks, anterior thigh, posterior thigh, etc.). | CK (p< 0.001 and effect size “ES”= 2.1) increased 24h after the half marathon. No increase in skin temperature was observed in tests after competition, and no regression model was able to predict physiological stress based on skin temperature. Only a bivariate correlation was observed between the 24-hour variation (pre – 24 h) of CK and the skin temperature of the posterior upper limb (p= 0.04; r= 0.5). | Monitoring basal skin temperatures doesn’t appear to be an adequate method to detect physiological stress after a half marathon. In line with the observed results, we recommend caution when interpreting peaks in basal skin temperature in field sports assessments. |
| Matta et al. (2019) |
Healthy male players from a Brazilian 1st division football club n= 10 Age: 25.3± 4.6 |
24 and 48 hours after a soccer match, GPS sensors were used to quantify the demand for game conditions among all participants, along with post-game measurements of serum CK, skin conductance and thermographic images of the lower limbs. | Anterior and posterior views of the lower limbs. Description of the ROI used: 5 cm above the upper edge of the patella to the line from the groin to the thigh; and for the leg, 5 cm below the lower edge of the patella to 10 cm above the lateral malleolus. | There was no significant difference (p> 0.05) in contralateral thermal symmetry in the lower limbs. However, both values (maximum and mean) of skin temperature showed a significant difference (p< 0.05) at rest when compared to 24h and 48h after the game. Furthermore, the serum CK level remained elevated for up to 48 h post-match compared to rest. | The results showed that 48 hours after the game is not enough for soccer players to fully recover. |
| Da Silva et al.* (2018) |
healthy untrained men n= 20 age: 24 |
Before, immediately after, and 48 h after a calf exercise protocol (multiple sets of plantar and ankle flexion for body elevation), blood samples were collected to determine CK and acetylcholinesterase activity. In addition, thermal images were recorded of the exercised muscles to determine skin temperature variation, and DMIT was quantified. | Anterior and posterior views of the legs. | There was an increase in CK activity 48 hours after exercise (p< 0.01). Skin temperature parameters didn’t correlate with creatine kinase responses (p> 0.05). | Changes in skin temperature are not correlated with the level of exercise-induced muscle damage estimated by CK activity in untrained individuals. |
| Drzazga et al. (2018) |
Two groups of elite male athletes. A group of cross-country skiers* and a group of elite endurance swimmers** n*= 6 n**= 4 age*: 23± 2.68 age**: 21.5± 2.08 |
At first, thermal images of the athletes’ bodies were recorded from the front and back, before, and about 1 to 2 minutes after performing a treadmill run until exhaustion. After two weeks, measurements were repeated after one hour of treadmill running. Functional (heart rate, oxygen consumption, workload) and biochemical (CK and LDH activities, lactate, and haemoglobin concentration) markers were also evaluated. | Anterior and posterior incidences of the body divided into 22 muscle zones (trapezius, pectoralis major, deltoid, serratus anterior, biceps brachii, latissimus dorsi, etc.). | Although there was great variability in the CK response among all subjects, the change in the activities of this augmenting enzyme was similar in each group, with no specific association with skin temperature. | Additional information about muscle work in different sports modalities can be useful in evaluating the efficiency of athletes. However, further investigation is needed to validate the results. |
| Andrade Fernandes et al.* (2017b) |
Under-20 athletes from the 1st Brazilian soccer division n= 10 age: 19± 1 |
Skin thermal responses obtained by IRT and CK concentration were evaluated in response to two soccer matches, with 3 days of recovery between each match. Measurements were taken 24 h before and after 24 h and 48 h after the first match. Then the data were measured again 24 h before and after 24 h and 48 h of the second match. | Anterior and posterior views of the lower limbs (thigh and leg). | Tsk and CK were moderately correlated in all analyzed ROI s, with greater correlation in the right leg anterior (r= 0.425) and left leg anterior (r= 0.428). | After obtaining lower limb Tsk as well as CK, there was a significant change in response to two consecutive matches separated by an interval of 3 days. In addition, an overall increase in these indices was obtained in the thighs and legs in the front and back. |
| Andrade Fernandes et al. (2017a) |
Right-handed defender, non-smoker athlete with no recent history of injury, member of a club from the 1st Brazilian football division n= 1 age: 27 |
24 hours before, 24 and 48 hours after an official soccer match, Tsk measurements with a thermal camera and blood CK concentrations were obtained using lancing devices. | Anterior and posterior views of the lower limbs (thigh and leg). | The results showed that CK values were 193 U/L 24 hours before, rising to 1.083 U/L 24 hours after the game and 414 U/L 48 hours after the game. Qualitative analysis of thermograms showed that entire lower limbs are much warmer 24 hours after the match, and certain areas such as right anterior thigh, left anterior leg, both anterior ankles and both posterior thighs have not fully recovered their initial Tsk 48 hours after the game. | Participation in a professional football match can lead to significant increases in Tsk values measured by 24-hour IRT. Thermography could help in the training control process as part of an injury prevention program in professional football clubs. |
| Bandeira et al.* (2014) |
Male Rugby Athletes of a National-Level Professional Club n= 21 age: between 19 and 31 |
Blood samples were taken to assess the serum CK concentration and the acquisition of infrared images of the athletes to assess the skin temperature, both 48 h after a rugby training session and 48 h after a rugby match. | Anterior and posterior views of the body, individually analysing all the main muscles and their portions. | There was no correlation between the CK variation and the mean temperature variation of the selected muscle areas. However, in the group of athletes who presented CK elevation above 50% between the first and the second time of evaluation, the muscles of the left pectoralis and the left semitendinosus presented significant differences with values of p= 0.037 and p= 0.045, respectively. | It is concluded that thermography can be used as a support method for diagnosing muscle injury in athletes. |
| Bandeira et al. (2012) |
Male athletes of the Paraná Clube soccer team n= 18 age: between 15 and 17 |
First, a thermographic image of each athlete was captured before the start of the training session. After the training session, a blood sample was collected to verify the serum lactate level of each athlete. Subsequently, 24 hours after training, another blood collection was performed to check the serum CK level of each athlete. Another individual thermographic image was also acquired at this stage | Quadriceps femoris and specific analysis of the rectus femoris, adductor longus, vastus medialis muscles. | There was no statistically significant correlation between CK values 24 h post-training and temperature variation (24 h post-training – pre-training) in the muscles evaluated for the control group. There was a statistically significant difference in temperature (24 h post-training – pre-training) for the three muscles studied only in the experimental group. | The use of thermographic images, together with CK, is a possibility to determine the intensity and location of muscle injuries after training since the aforementioned biochemical marker cannot determine the anatomical location of the muscle injury. |
| Petrofsky et al. (2012) |
healthy individuals n= 20 age: between 20 and 40 |
Heat was applied for 8h immediately after an exhausting biceps exercise (4 sets of 25 repetitions with 35% of 1RM) or applied after 24 h or both. Self-reported pain perception and blood biomarkers were measured through blood collection before, immediately after and 3 h, 24 h, 48 and 72 h after the exercise session. | Incidences in 4 regions of the biceps brachii. | In all groups evaluated, there was an increase in skin temperature 24h after exercise. In the immediate heat group, CK increased within 48h. The biggest increase was in the 24h heat group, with the immediate plus 24h heat group falling in between. For the 24h heat group, CK increased to 3.280ng for 72 h. Didn’t indicate association. | When heat is applied immediately to the area of exercised muscle, there is a reduction in muscle pain and an apparent acceleration in the recovery process compared to not applying heat. |
| Petrofsky et al. (2011) |
healthy individuals n= 20 age: between 20 and 40 |
Heat was applied for 8h immediately after exhaustive biceps exercise. (25 repetitions until exhaustion with 35% of 1RM) or applied after 24 h or both. Self-reported pain perception and blood biomarkers were measured through blood collection before, immediately after and 3 h, 24 h, 48 and 72 h after the exercise session. |
Incidences in 4 regions of the biceps brachii. | Muscle temperature increased at 3 and 24 hours after exercise and decreased at 48 h. Mean CK was 120.2± 28.2 ng/ml pre-exercise, with no difference between groups (p> 0.05). Didn’t indicate association. |
The data suggest that heat applied immediately and/or 24 hours after exercise reduces muscle pain and accelerates the healing process. |
*Articles selected to compose the meta-analysis according to the eligibility criteria.
From the related samples, all studies selected healthy, non-injury professional athletes, with general ages ranging from 15 to 47 years, and from sports such as soccer, rugby, cross-country skiers, and endurance swimmers, except four studies that selected amateur runners (Pérez-Guarner et al., 2019), untrained men (Da Silva et al., 2018), and just healthy individuals (Petrofsky et al., 2011; Petrofsky et al., 2012). The selected ROI, in turn, were in short anterior and posterior chains of the lower limbs, except for three studies that included anterior and posterior views of the whole body (Drzazga et al., 2018; Pérez-Guarner et al., 2019; WHO, 2014) and two more that selected only the biceps (Petrofsky et al., 2011; Petrofsky et al., 2012) as the region of interest.
Regarding the intervention methods, all studies performed infrared thermal imaging and blood collection, obtaining, respectively, the surface temperature of the skin in the ROI and the serum levels of CK and other biomarkers. Some studies also measured other variables such as countermovement jumping (Júnior et al., 2021; Pérez-Guarner et al., 2019), perception of recovery (Carvalho et al., 2021), perception of fatigue (Barros et al., 2020; Carvalho et al., 2021; Pérez-Guarner et al., 2019), perception of pain (Barros et al., 2020; Carvalho et al., 2021; Da Silva et al., 2018; Pérez-Guarner et al., 2019; Petrofsky et al., 2011; Petrofsky et al., 2012), functional markers (heart rate, the volume of maximum oxygen, etc.) (Drzazga et al., 2018) and peak torque (Barros et al., 2020). In addition, each author performed the assessments in different time frames. Regarding stimuli (sports matches, aerobic exercises, counter-resistance exercises, etc.), the authors performed the assessments as follows: 48 h before (Pérez-Guarner et al., 2019), 24 h before (Andrade Fernandes et al., 2017a; Andrade Fernandes et al., 2017b; Pérez-Guarner et al., 2019), immediately before (Bandeira et al., 2012; Barros et al., 2020; Da Silva et al., 2018; Drzazga et al., 2018; Júnior et al., 2021; Petrofsky et al., 2011; Petrofsky et al., 2012), immediately after (Bandeira et al., 2012; Da Silva et al., 2018; Júnior et al., 2021; Neves et al., 2016), 1 h after (Drzazga et al., 2018), 3 h after (Petrofsky et al., 2011; Petrofsky et al., 2012), 24 h after (Andrade Fernandes et al., 2017a; Andrade Fernandes et al., 2017b; Bandeira et al., 2012; Carvalho et al., 2021; Matta et al., 2019; Pérez-Guarner et al., 2019; Petrofsky et al., 2011; Petrofsky et al., 2012), 48 h after (Andrade Fernandes et al., 2017a; Andrade Fernandes et al., 2017b; Bandeira et al., 2012; Barros et al., 2020; Da Silva et al., 2018; Petrofsky et al., 2011; Petrofsky et al., 2012) and 72 h after (Petrofsky et al., 2011; Petrofsky et al., 2012).
Table 3 below shows the quality assessment of studies carried out with the QUADAS-2 tool (Whiting et al., 2006) by analysing the risk of bias and concerns about the applicability and external validity of the studies, classifying them as low risk (↓), non-risk evident (?) and high risk (↑).
Table 3. Results of the assessment of risks of bias and QUADAS-2 applicability of the studies included in the systematic review that associated CK with thermography.
| Bibliographic Reference | Risk of Bias | Applicability Concern | ||||||
|---|---|---|---|---|---|---|---|---|
| Patient Selection | Index Test | Reference Test | Timing | Patient Selection | Index Test | Reference Test | ||
| Júnior et al. (2021) | ↓ | ↓ | ↓ | ↓ | ↓ | ↓ | ↓ | |
| Carvalho et al.* (2021) | ↓ | ↓ | ↓ | ↓ | ↓ | ↓ | ↓ | |
| Barros et al. (2020) | ? | ↓ | ↓ | ↓ | ↓ | ↓ | ↓ | |
| Pérez-Guarner et al.*(2019) | ↓ | ↓ | ↓ | ↓ | ↓ | ↓ | ↓ | |
| Matta et al. (2019) | ? | ↓ | ↓ | ↓ | ↓ | ↓ | ↓ | |
| Da Silva et al.* (2018) | ↓ | ↓ | ↓ | ↓ | ↓ | ↓ | ↓ | |
| Drzazga et al. (2018) | ? | ↓ | ↓ | ↓ | ↓ | ↓ | ↓ | |
| Andrade Fernandes et al.* (2017b) | ? | ↓ | ↓ | ↓ | ↓ | ↓ | ↓ | |
| Andrade Fernandes et al. (2017a) | ↑ | ↓ | ↓ | ↓ | ↓ | ↓ | ↓ | |
| Bandeira et al. *(2014) | ↓ | ↓ | ↓ | ↓ | ↓ | ↓ | ↓ | |
| Bandeira et al. (2012) | ? | ↓ | ↓ | ↓ | ↓ | ↓ | ↓ | |
| Petrofsky et al. (2012) | ↓ | ↓ | ↓ | ↓ | ↓ | ↓ | ↓ | |
| Petrofsky et al. (2012) | ↓ | ↓ | ↓ | ↓ | ↓ | ↓ | ↓ | |
↓: Low risk; ↑: High risk; ?: Risk not evident; *Articles selected to compose the meta-analysis according to the eligibility criteria.
Considering the 13 studies reviewed, there is a general balance in obtaining results of CK increase along with skin temperature versus studies that didn’t observe any association between the measures. In other words, five studies (Andrade Fernandes et al., 2017a; Andrade Fernandes et al., 2017b; Júnior et al., 2021; Matta et al., 2019; Pérez-Guarner et al., 2019) found some association between the variables and eight studies (Andrade Fernandes et al., 2017b; Bandeira et al., 2012; Carvalho et al., 2021; Da Silva et al., 2018; Matta et al., 2019; Petrofsky et al., 2011; Petrofsky et al., 2012) didn’t find any type of association.
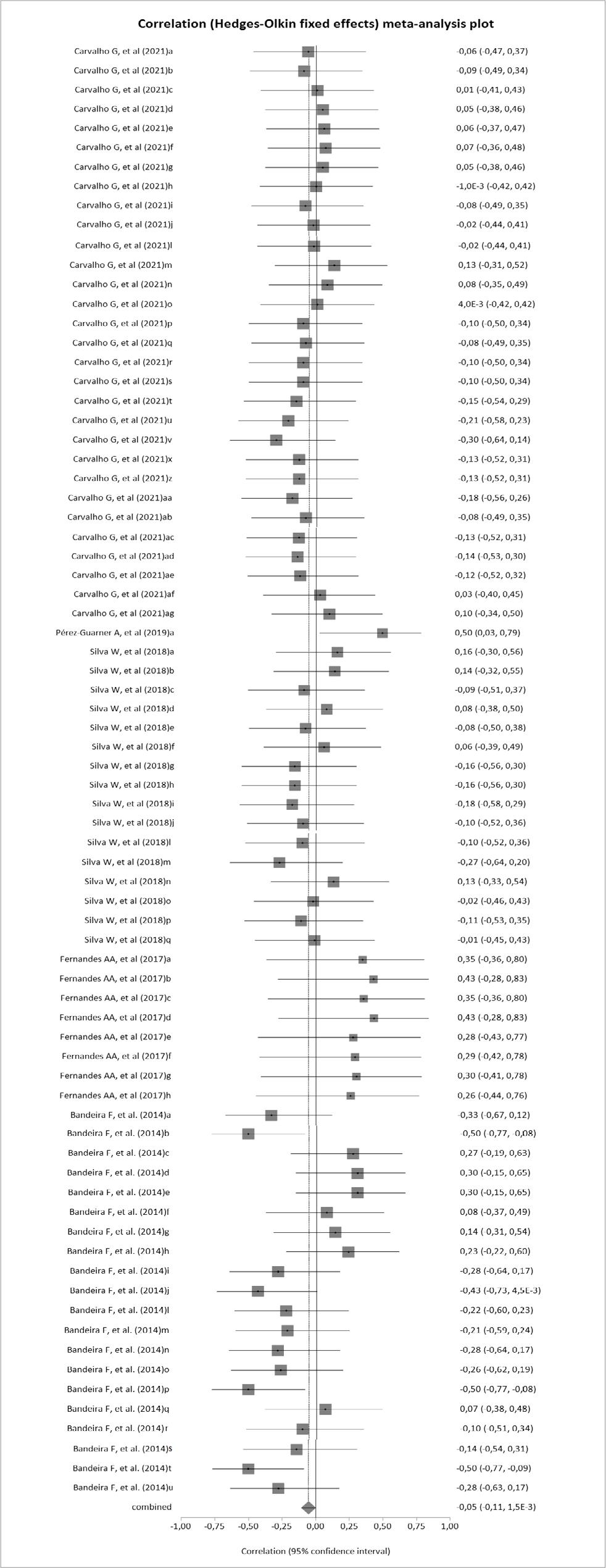
The result of the meta-analysis is shown in Figure 2 below. Each line of the graph, generated in the Stats Direct 3.0 tool, indicates the Pearson or Spearman correlation coefficient in each region of interest analyzed by thermal imaging in certain temporal sections evaluated by each author, with their respective p values inserted. In addition, the I2 statistic = 0% (95%CI 0% – 25.8%) was observed, indicating that there isn’t evidence of heterogeneity between studies. Thus, according to Figure 2, the correlation coefficient of the combined studies presented r= –0.05 (95%CI –0.11 – 0), with p-value= 0.0568, which indicates a result not significant for the association between CK and thermography.
DISCUSSION
The present study evaluated the statistical association between serum CK levels and skin temperature through a systematic review with meta-analysis. A total of 483 studies were retrieved from the databases, and 13 were selected for qualitative analysis, five of which were selected for quantitative analysis (Figure 1).
Most of the authors (Andrade Fernandes et al., 2017b; Bandeira et al., 2012; Da Silva et al., 2018; Matta et al., 2019) who claimed not to find associations didn’t present the corresponding statistical data. Furthermore, there was one author (Pérez-Guarner et al., 2019) who found an association is only one of the chosen ROIs and presented this only result, failing to present the non-association results obtained from the other ROIs. Some authors (Andrade Fernandes et al., 2017b; Barros et al., 2020; Drzazga et al., 2018; Júnior et al., 2021; Matta et al., 2019; Pérez-Guarner et al., 2019; Petrofsky et al., 2011; Petrofsky et al., 2012) presented general results, without providing the association in each chosen ROI.
Comparing the reviewed studies, the fact of obtaining a general balance between positive and negative results for the association between variables observed by the systematic review reinforces that there isn’t consensus in the literature and that, consequently, there isn’t a way to categorically state that there is any relationship between the variables. Da Silva et al. (2018), for example, observed that there was no association between the two variables after a muscle injury induction protocol; it can be said that in a real situation, with the analysis of training diaries and comparing with laboratory situations, it wasn’t possible to see an association between muscle damage biomarkers with increased skin temperature. However, it is worth noting that a good part of the studies, such as the one by Andrade Fernandes et al. (2017b) for example, found significant associations with the justification that strenuous exercise does generate micro muscle injuries that cause muscle CK to leak into the bloodstream, as well as lead to inflammatory processes that increase local temperature. However, studies recommend caution when interpreting the results, as well as reinforcing the idea of using thermography as a joint diagnostic support method, as Bandeira et al. (2014) recommends for example.
Some studies performed collections 48 h before (Pérez-Guarner et al., 2019) and 24 h before (Andrade Fernandes et al., 2017b; Neves et al., 2015; Pérez-Guarner et al., 2019), as well as immediately before (Andrade Fernandes et al., 2017b; Bandeira et al., 2012; Barros et al., 2020; Da Silva et al., 2018; Drzazga et al., 2018; Júnior et al., 2021; Matta et al., 2019; Petrofsky et al., 2011; Petrofsky et al., 2012) and after (Bandeira et al., 2012; Barros et al., 2020; Da Silva et al., 2018; Júnior et al., 2021) and also 1 h after (Drzazga et al., 2018), 3 h after (Petrofsky et al., 2011; Petrofsky et al., 2012), 24 h after (Andrade Fernandes et al., 2017a; Andrade Fernandes et al., 2017b; Bandeira et al., 2012; Carvalho et al., 2021; Matta et al., 2019; Pérez-Guarner et al., 2019; Petrofsky et al., 2011; Petrofsky et al., 2012), 48 h after (Andrade Fernandes et al., 2017a; Andrade Fernandes et al., 2017b; Bandeira et al., 2012; Barros et al., 2020; Da Silva et al., 2018; Petrofsky et al., 2011; Petrofsky et al., 2012) and up to 72 h after (Petrofsky et al., 2011; Petrofsky et al., 2012), with each author choosing a period they deemed convenient for their intervention, causing divergences in the general comparison of studies. In addition, some authors (Bandeira et al., 2012; Barros et al., 2020; Drzazga et al., 2018; Júnior et al., 2021; Petrofsky et al., 2011; Petrofsky et al., 2012), despite having performed collections in different periods, presented statistical results of general association, while others presented results by period specifically (Andrade Fernandes et al., 2017b).
This difference in the time cut used by each author (1 h, 3 h, 24 h, 48 h, etc. after intervention) may impact the interpretation of the results since CK has its peak incidence in the bloodstream within 24 h after the stimulus, with cases in which it can increase or decrease within 72 hours (Bandeira et al., 2012). Thus, it is considered that this non-linearity of the biomarker and the fact that some blood collections were performed outside this time range after the stimulus may have affected the association between the observed CK level and skin temperature. However, heterogeneity wasn’t observed among the included studies.
The results showed that thermographic evaluation isn’t a recommended substitute for tests to detect the indirect biomarker CK in blood since no significant association was observed in the evaluation by meta-analysis (r= –0.05; p= 0.0568; 95%CI –0.11 – 0). In addition to the divergence in the design of the studies analyzed, this result can also be explained based on the physiology of each of these indicators. CK is a systemic biochemical indicator present in the bloodstream, and its values can be altered by damage to inner or outer muscles. On the other hand, although body temperature is also systemic, surface skin temperature (measured by thermography) is a local indicator (Fernández-Cuevas et al., 2015), reinforcing the lack of association.
In addition, skin temperature can be influenced at times due to inflammation or infection, fractures, oedema, etc. (Fernández-Cuevas et al., 2015). CK values, on the other hand, aren’t necessarily modified by these types of alterations, except when they result from a muscle injury (Bandeira et al., 2012). Another factor to be considered is that each individual may present different levels of this biomarker, and some individuals may reach this CK peak in the bloodstream within 72 hours (Bandeira et al., 2012).
Bandeira et al. (2012) already stated that thermography associated with the use of CK could be used as a complementary method for locating muscle injuries in athletes, suggesting, however, opting for visual inspection of thermal images. The results found in this meta-analysis reinforce the practical applicability of thermography, like the fact that no significant association was found between serum CK levels, as well as the association between thermographic assessment and the risk of injury (Santos Bunn et al., 2020), which reinforces the idea of using thermal imaging in sports as a complementary method to more invasive exams for the assessment of athletes and, mainly, in the diagnosis and prevention of injuries, because when there is an association between two methods, it isn’t necessary to use both, as from one of them it would be possible to estimate the other.
Thus, the main limitations of the evidence included in the review are related to the limited provision of statistical data, as well as the lack of magnitude and quantity of results. When comparing serum CK levels and thermography, there is a lack of presentation of correlation coefficients.
Limitations of this study can be mentioned: the scarcity of studies specifically looking for the association between serum CK levels and thermography, the diversity of different study designs, and, as mentioned in the previous paragraph, the lack of objective records of the relationship between serum CK levels and skin temperature.
To provide a perspective for future studies, we suggest the scientific community carry out further research seeking the association between serum CK levels and thermography in sports that have a low possibility of trauma due to contact between athletes since this can represent an intervening variable in the study impacting the interpretation of infrared images. Another suggestion is to search for this association in sports activities, whose primary motor muscles are superficial, such as cycling and hard running, making it easier and more accurate to identify, through thermal images, possible muscle damage that will also lead to an increase in CK.
CONCLUSION
Considering the parameters related to the use of thermography in this systematic review with meta-analysis, it can be concluded that there is no association between serum CK levels and thermography results. In clinical practice, it is recommended to use infrared thermal images in complement to the assessment of serum CK levels to assist in the determination of differential diagnoses of musculoskeletal injuries.

