











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
INTRODUCTION
The increase in population ageing is a phenomenon observed worldwide, specifically in Brazil, the growth of the elderly population has been considered exponential, with the prospect of even greater growth (Wong & Carvalho, 2006). The reason for this fact has been directed to the extension of life expectancy. This constant growth is accompanied by social changes and a high prevalence of chronic diseases, contributing to reduced functional capacity (Chodzko-Zajko et al., 2009).
Linked to other factors, such as a sedentary lifestyle, ageing makes this population a risk group, requiring greater attention since they are naturally susceptible to diseases in general and functional damage (Bocalini et al., 2012). Thus, the regular practice of physical activity as well as the adoption of a healthy lifestyle, can provide considerable physiological adaptations, impacting muscle mass gains (Gai et al., 2010), reducing anxiety and depression (Souza et al., 2014), in addition to promoting positive responses in osteo-metabolic disorders (Bocalini et al., 2012).
Thus, strategies for improving, developing and implementing healthcare actions for the population, regardless of age group, have been disseminated. Senior centres, also commonly known as elderly centres, seniors’ clubs or community centres, offer a wide variety of programs and services. By offering opportunities for social interaction and friendship, senior centres have traditionally had a central role in easing loneliness, increasing social integration and reducing isolation (Bøen et al., 2010; Bøen et al., 2012; Rosenberg, 2015). Currently, the community centre also gained relevance as promoters of physical activity and successful ageing (Marhánková, 2014; Marquet et al., 2017; Marquet & Miralles-Guasch, 2015).
Among these strategies, that with the creation of the National Policy for the Elderly (Law nº 8.84 2/1994) regulated by decree nº 1.948/1996 and in the IV paragraph of the elderly care policy of the statute of the elderly (Law nº 8.842/ 1994) enabled numerous social assistance programs to promote better assistance to the elderly population, aiming to provide full assistance to the elderly. Studies (Beneditti & Petroski, 1999; Paulo et al., 2012; Tomicki et al., 2016) have often shown satisfactory results considering strategies offered in community centres for the elderly care in morphofunctional (Beneditti & Petroski, 1999), behavioural (Paulo et al., 2012) and psychological parameters.
Although the community centre has been considered an effective strategy to improve physical activity participation (Sarkisian et al., 2007; Porter et al., 2011), there is a lack of research devoted to measuring and objectively assessing the lifestyle and functional fitness gain from their visits to senior centres. Moreover, comparisons between the genders of elderly people attending these centres are still inconclusive. Therefore, the aim of the study was to evaluate and compare the lifestyle, depressive symptoms and functional aptitude of elderly men and women attending a community centre.
METHODS
The research was characterised as descriptive, exploratory, transversal and quantitative approach was carried out with 277 elderly people (197 women and 80 men) aged over 60 years who are physically independent and were recruited in a community centre and participated voluntarily in this study. The community centre serves approximately 800 elderly people in the region, being assisted in various activities, such as: water-based exercise, adapted volleyball, walking groups and various types of dance. They also have a literacy assistance service, computer rooms, and psychological support. In addition, the space also offers activities aimed at leisure, such as meetings scheduled for simple interaction between those interested.
After approval of the study by the Ethics and Research Committee of the Universidade Federal do Espírito Santo (nº: 4,131.396/2020), all elderly people attending—a community centre of Venda Nova do Imigrante (ES, Brazil) were invited to randomly participate in the study. All the elderly who participated in the project started the procedures only after providing a free and informed consent term signed according to the Declaration of Helsinki. The following exclusion criteria were adopted: recent hospitalisation, symptomatic cardiorespiratory disease, hypertension or uncontrolled metabolic syndrome, severe kidney or liver disease; cognitive impairment or progressive and debilitating conditions, obesity accentuated with incapacity for physical activity; recent bone fractures or any other medical contraindications for physical exercise.
Parameters evaluated
Lifestyle assessment
Lifestyle assessment was performed using the fantastic lifestyle questionnaire validated for the Brazilian population by Rodriguez-Añez et al. (2008). The instrument takes into account behaviours presented by individuals in the last month and the results obtained after the association between lifestyle and health itself. The tool has 25 questions, divided into nine domains, which were presented above, which are: 1) family and friends; 2) physical activity; 3) nutrition; 4) cigarettes and drugs; 5) alcohol; 6) sleep, seat belt, stress and safe sex; 7) type of behaviour; 8) introspection; 9) work.
The 25 questions that comprised the body of the questionnaire were arranged on the Likert scale so that 23 of these have five possible alternatives as answers, and 2 are presented in dichotomous ways. In order for the questionnaire to be applied in a simple way and later more easily to have the answers tabulated, the alternatives were arranged in column format, and progressively, from left to right, the choices were related to a healthier lifestyle. After completing the questionnaire, the results were obtained through the sum of this score, where the column, when marked, represents 1 point, and the column farthest to the right represents a score of 5 points on the scale. After the sum of the 25 columns, a score was obtained, in which individuals were classified into 5 categories, which are: “Excellent” (85 to 100 points), “Very good” (70 to 84 points), “Good” (55 to 69 points), “Regular” (35 to 54 points) and “Needs improvement” (0 to 34 points).
The interpretation of the scale is the following: “Excellent” rating is established as people who have a lifestyle with great influences on health; “Very good” means they have a lifestyle that provides an adequate influence on health; “Good” means that the lifestyle provides many health benefits; “Regular” means that somehow the lifestyle provides some health benefit, however, health risks will also be present; “Needs improvement” represents the lowest score, which means that several changes will be needed, as this lifestyle has many risk factors for the individual.
Functional fitness
Functional aptitude was assessed by the protocol of functional autonomy of maturity of the Latin American development group (GDLAM) being proposed by Dantas and Vale (2004) and used by other studies of our group (Suzuki et al., 2018). The protocol consists of carrying out the following tests: walking 10 m (W10m), getting up from a sitting position (LPS), rising from the prone position (LPDV) and getting up from the chair and moving around the house (LCLC). All tests were performed in the order described above, in a single day, using a 3-minute break between them to allow for good recovery between tests. According to Dantas and Vale (2004), the GDLAM General Index was calculated with the results considering Equation 1:
The functional classification followed the recommendations suggested by Dantas and Vale (2004), being distributed in indicators such as low (+28.54 points), regular (28.54 to 25.25 points), good (25.24 to 22.18 points) and very good (–22.18 points).
Depression
After applying the socio-demographic questionnaire, the assessment of depressive symptoms was analysed using the geriatric depression scale proposed by Yesavage et al. (1982). The instrument consists of 15 items with dichotomous responses. The score varies between 0 and 15 points and aims to include the following points: less than 5 points meaning a normal individual or without depressive symptoms; above or equal to 5 points, individual with depressive symptoms. For this study, the cutoff point was used for the summed results that result in a score equal to or greater than five, as indicative of symptoms of depression and in cases where the value obtained is less than five, it is established that there is no evidence of symptoms of depression.
Statistical analysis
The variables in this study are qualitative-quantitative. The data underwent statistical treatment with a descriptive approach, using resources of absolute (n), relative (%) frequency for qualitative variables and measures of central tendency (mean) and dispersion (standard deviation) for quantitative variables. To compare the differences between the groups of women and men, the χ2 test was used for qualitative variables and the Student-t test for quantitative parameters. The effect size (ES) calculation and interpretation were based on the values established by Cohen: < 0.01= small effect; 0.06= moderate effect; and ≥ 0.14= large effect.
Analyses were performed using GraphPad Prism software (v. 6.01; GraphPad Software, USA) with a significance level of p < 0.05 with data presented as mean± standard deviation.
RESULTS
The general characteristics of the sample are presented in Table 1. A total of 277 elderly people participated in the study, 197 (71%) women and 80 (29%) men. Among them, 57.40% of the elderly were aged between 60 and 70 years, with 43.68% having the 4th grade in elementary school and 35.38% illiterate, and the vast majority being retired, with 89.17% of the general sample. Additionally, significant differences (x2; p= 0.0002) were found in age between women and men, however, no differences between them were found in scholarship (x2; p= 0.1202) and in occupation (x2; p= 0.1176).
Table 1. Socio-demographic characteristics of elderly.
| Parameters | Overal | Women | Men | p-value | |||
|---|---|---|---|---|---|---|---|
| F | % | F | % | F | % | ||
| Age (years) | |||||||
| 60 to 70 | 159 | 57.40 | 128 | 64.97 | 31 | 38.75 | 0.0002 |
| 71 to 80 | 100 | 36.10 | 62 | 31.47 | 38 | 47.50 | |
| 81 to 90 | 16 | 5.78 | 6 | 3.05 | 10 | 12.50 | |
| 91 and more | 2 | 0.72 | 1 | 0.51 | 1 | 1.25 | |
| Schoolarship | |||||||
| Up to 3years | 98 | 35.38 | 62 | 31.47 | 36 | 45.00 | 0.1202 |
| 4 years | 121 | 43.68 | 93 | 47.21 | 28 | 35.00 | |
| 9 years | 20 | 7.22 | 12 | 6.09 | 8 | 10.00 | |
| 11 years | 21 | 7.58 | 17 | 8.63 | 4 | 5.00 | |
| Graduate | 17 | 6.14 | 13 | 6.60 | 4 | 5.00 | |
| Ocupation | |||||||
| Employed | 6 | 2.17 | 4 | 2.03 | 2 | 2.50 | 0.1176 |
| unemployed | 11 | 3.97 | 10 | 5.08 | 1 | 1.25 | |
| Retired | 247 | 89.17 | 174 | 88.3 | 73 | 91.25 | |
| Early retired by medical reason | 7 | 2.53 | 3 | 1.52 | 4 | 5.00 | |
| Housewife | 6 | 2.17 | 6 | 3.05 | 0 | 0.00 | |
F: frequency.
As seen in Table 2, 57.40% of the elderly had a very good lifestyle, followed by 25% good and 17% excellent. Comparing the parameters as well as the classification of lifestyle between women and men, significant differences (p < 0.001) were found in the family, alcohol, behaviour and introspection domains of the lifestyle as well as in the classification of the lifestyle where a higher prevalence (p < 0.0001) was found.
Table 2. Life style parameters of elderly people.
| Parameters | Overall | Women | Men | MD [95%CI] | ES | p-value |
|---|---|---|---|---|---|---|
| Family and friends | 6.35± 1.80 | 6.13± 1.91 | 6.88± 1.38 | 0.75 [0.28 – 1.21] | 0.39 | 0.0016 |
| Physical activity | 5.00± 2.02 | 4.89± 2.04 | 5.25± 1.95 | 0.35 [–0.17 – 0.88] | 0.17 | 0.1878 |
| Nutrition | 8.65± 2.13 | 8.75± 2.09 | 8.40± 2.25 | 0.35 [–0.90 – 0.20] | 0.16 | 0.2157 |
| Cigarettes and drugs | 14.18± 1.38 | 14.25± 1.35 | 14.01± 1.45 | 0.24 [–0.60 – 0.11] | 0.1885 | |
| Alcohol | 11.73± 1.34 | 11.95± x.48 | 11.18± 2.30 | 0.77 [–1.11 – –0.43] | 0.17 | < 0.0001 |
| Sleep, seatbelts, stress, and safe sex | 14.61± 2.40 | 14.49± 2.33 | 14.90± 2.57 | 0.40 [–0.22 – 1.03] | 0.18 | 0.2024 |
| Type behavior | 4.55± 2.10 | 4.38± 2.16 | 4.97± 1.88 | 0.58 [0.03 – 1.14] | 0.27 | 0.0376 |
| Introspection | 8.58± 2.40 | 8.33± 2.44 | 9.20± 2.10 | 0.86 [0.24 – 1.48] | 0.35 | 0.0006 |
| Work and satisfaction with profession | 3.56± 0.73 | 3.58± 0.75 | 3.53± 0.67 | 0.07 [–0.26 – 0.11] | 0.06 | 0.4327 |
| Total score | 76.91± 7.49 | 76.50± 7.49 | 77.91± 7.44 | 1.41[–0.54 – 3.36] | 0.18 | 0.1561 |
| Classification | F (%) | F (%) | F (%) | |||
| Excellent | 48 (17.33) | 24 (12.18) | 24 (30.00) | < 0.0001 | ||
| Very good | 159 (57.40) | 138 (70.05) | 21 (26.25) | |||
| Good | 68 (24.55) | 34 (17.26) | 34 (42.50) | |||
| Regular | 2 (0.72) | 1 (0.51) | 1 (1.25) | |||
| Needs improvement | 0 (0) | 0 (0) | 0 (0) |
Values expressed in mean± SD; MD [95%CI]: mean difference [95% confidential interval]; ES: effect size; F: frequency.
As shown in Table 3, significant differences (p< 0.001) were found in all tasks and in the classification of functional fitness between women and men. Variations of 52.43% and 13.51% among women and 38.46% and 33.33% among men in the classification between weak and very good, respectively. Although the lifestyle was considered very good, 45.29% of the elderly had a low level of functional fitness.
Table 3. Functional fitness of elderly people.
| Parameters | Overall | Women | Men | MD [95% CI | ES | p-value |
|---|---|---|---|---|---|---|
| W10m (sec) | 6.37± 1.94 | 6.51± 2.85 | 5.87± 2.08 | 0.63 [–1.14 – –0.13] | 0.22 | 0.0137 |
| LPS (sec) | 11.31± 3.29 | 11.58± 3.19 | 10.67± 3.47 | 0.90 [–1.77 – –0.04] | 0.28 | 0.0385 |
| LPDV (sec) | 4.29± 2.81 | 4.58± 3.12 | 3.61± 1.76 | 0.97 [–1.70 – –0.23] | 0.31 | 0.0095 |
| LCLC (sec) | 43.29± 11.53 | 44.40± 11.88 | 40.70± 13.65 | 3.69 [–6.98 – –0.43] | 0.31 | 0.0267 |
| GS (score) | 29.06± 8.09 | 29.92± 7.79 | 27.04± 0.8.48 | 2.87 [–4.97 – –0.76] | 0.36 | 0.0076 |
| Classification | F (%) | F (%) | F (%) | |||
| Very good | 51 (19.39) | 25 (13.51) | 26 (33.33) | 0.0030 | ||
| Good | 42 (15.97) | 31 (16.76) | 11 (14.10) | |||
| Regular | 43 (16.35) | 32 (17.30) | 11 (14.10) | |||
| Low | 127 (45.29) | 97 (52.43) | 30 (38.46) |
Values expressed in mean± SD. Walking 10 m (W10m), getting up from a sitting position (LPS), rising from the prone position (LPDV) and getting up from the chair and moving around the house (LCLC) and GDLAM score (GS); MD [95%CI]: mean difference [95% confidential interval]; ES: effect size; F: frequency.
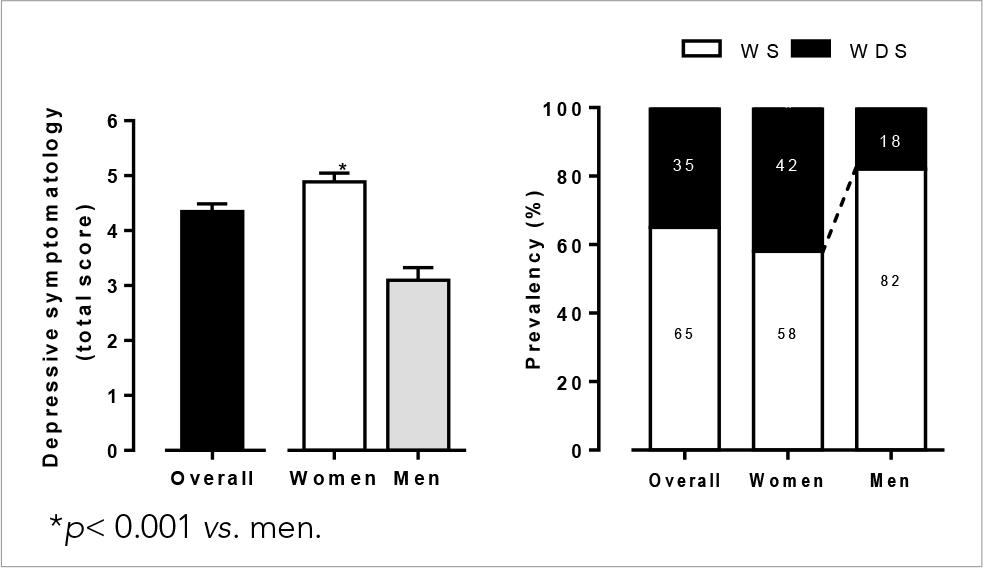
In Figure 1, it is possible to visualise the scores of depressive symptoms as well as the prevalence considering the presence or absence of symptoms. After analysing the scale, the mean total score of the elderly was 4.34± 2.60, reaching a prevalence of 35% of elderly people with depressive symptoms. Statistical differences (p< 0.001) were found after analysis by sex, with 42% of women presenting depressive symptoms with a mean score of 4.88± 2.66 points and 18% of men with 3.10± 2.04 points.
DISCUSSION
The aim results of the present study indicate that depressive symptoms were present in 35% of the elderly attending a community centre, however, the lifestyle analysis showed that 57.40% of the elderly had a very good classification followed by 24.55% as good, 17.33% as excellent and 0.72% as regular. With regard to functional fitness, 19.39% of the elderly had a score related to a very good level, 15.97% good, 16.35% fair and 45.29% weak. Studies dedicated to investigating the influence of socioeconomic indicators, demographics, lifestyle as well as level of physical fitness are important, mainly due to their association with health. So, with the accumulation of knowledge generated by the studies, it is possible to generate improvements in implementing healthcare strategies for the population, regardless of age.
In Brazil, based on the creation of the National Policy for the Elderly (Law No. 8.84 2/1994) regulated by Decree No. 1.948/1996 and the IV paragraph of the elderly care policy of the Statute for the Elderly (Law No. 8.842/1994) and programs of social assistance, strategies were disseminated in order to promote better care for the elderly population. In this context, in 2001, through the ordinance MPAS/SEAS No. 7, the creation of community centres for the elderly emerged in a regulated manner, with the aim of promoting interaction between the elderly, family and community.
Studies (Guimarães et al., 2020; Nóbrega et al., 2015) have already dedicated themselves to investigating the influence of these spaces in different perspectives of elderly care, emphasising problems associated with depression. Considering that depression is considered one of the major public health problems (Strawbridge et al., 2002), as it affects about 17% of the world population, understanding the possible indicators associated with the disease is considered essential for applications and interventions for the treatment and prevention of this disease. Currently, it is known that, although the disease can affect people at any stage of life, the elderly population is frequently affected by the disease, with variations between 15 and 30%, especially in institutionalised populations (Stella et al., 2002).
According to Pinton et al. (2006), among the classic factors identified in the depressive condition, it is possible to consider that three domains are primarily affected, namely: the affective domain, identified through crying, apathy and sadness; the cognitive domain, which manifests itself through feelings of worthlessness, lack of hope, guilt and finally the somatic domain, which is related to pain, lack of energy and sleep disorders. Considering the level of depressive symptoms, the prevalence (35%) of the present study was similar to that in other studies carried out by our group (Guimarães et al., 2020; Valadares et al., 2019) in a different city of the same region (which found a variation between 35 and 37% of depressive symptoms in the elderly). Similar data were also found in other Brazilian cities, with values corresponding to 30.6% (Nogueira et al., 2014). Many factors can influence these results, such as socioeconomic factors, retirement, decreased self-esteem, low education, low income, high drug consumption, reduced ability to perform daily activities, and loss of close people, such as spouse, children or friends. All these factors are considered triggering for the onset of depressive symptoms (Irigaray & Schneider, 2007).
Another important component frequently investigated in the ageing process is functional fitness, mainly due to its association with an independent lifestyle. Blay et al. (1991) demonstrated that elderly women with poor health were associated with lower functional capacity as well as low social status. In our study, 45.39% of the elderly were classified as weak, with the same phenomenon found in men (52.43%) and women (38.46%). There is evidence that indicators of functional independence are associated with depressive symptoms, for example, Guimarães et al. (2020) and Branco et al. (2015) demonstrated a positive correlation between the scores of depressive symptoms and functional capacity, indicating that impairments in functional fitness can contribute for a higher incidence of depressive symptoms. Using the functional fitness indicator, the value presented in the present study (29± 8) was lower than that found by Guimarães et al. (2020), who presented 36.23± 28.75 of elderly people without depressive symptoms.
Branco et al. (2015) demonstrated that elderly people who present decreased exercise intensity, physical activity, and physical fitness tend to exhibit more depressive symptoms compared to those who remain active throughout life. Additionally, it is known that impairments in physical mobility can promote low self-esteem, decrease participation in the community and reduce the circle of social relationships that can naturally affect the increase in cognitive, behavioural and physical complications (physical fitness) that together intensify the ageing process.
Thus, the information presented collectively in the literature is consensual in considering that physical fitness directly affects functional capacity. In this sense, adopting a healthy lifestyle is considered decisive to promote improvements in the perception of quality of life and functional independence of the elderly (Ferreira et al., 2012). Valadares et al. (2019) demonstrated that lifestyle is an important parameter for the increase of depressive symptoms, with the group with depressive symptoms classified as having a good and regular level. In our study, the classification values of lifestyle varied between good and excellent, with the highest prevalence classified as very good (57.40%). In addition to considering the total lifestyle score, the values found in the present study (77± 8) were similar to those found by Valadares et al. (2019) in the group without depressive symptoms (79± 8).
The individual lifestyle indicators in our study were similar to the values found by Valadares et al. (2019) for elderly people without depressive symptoms. Indeed, there are studies showing that psychiatric disorders are associated with family problems such as lack of contact with family members (Teston et al., 2014), lack of physical activity (Moraes et al., 2007), high practice of physical activity and the predisposition to adopt healthy habits (Hua et al., 2015).
Considering the differences between men and women, our data agree with those by Gomes et al. (2007), showing that women tend to be more involved in community programs and more concerned with health than men. Additionally, it is worth mentioning that although sex differences were found in the lifestyle indicators, the classifications ranged from good and very good to excellent.
Therefore, the behaviours adopted by people can influence the quality of their ageing, namely healthy eating behaviour and involvement in personal, social, and physical activities that can positively influence physical function, mental function and also the individual’s engagement with life (Oliveira et al., 2007).
Although lifestyle was considered adequate, the indicators of functional fitness in the present study were considered low for both sexes. Thus, our findings are not in agreement with information available in the literature indicating that more active lifestyles are related to higher levels of functional fitness (Cardoso et al., 2008). Hypotactically, although the activities of the community centre are efficient in promoting positive behavioural changes, they were not sufficient to promote the improvement of physical fitness parameters (dose-response relationship).
Some limitations should be indicated in the present study and serve as guidelines for future studies, with emphasis on the non-assessment of the level of physical activity according to its type (physical activity at home, displacement, occupational, leisure and recreational physical activity). In addition, because the study proposes to investigate the lifestyle and its indicators, objective evaluation considering caloric intake, food choice, and distribution must also be accounted for in future studies. Finally, additional clinical and psychological assessments using multivariate analyses may also help to evaluate the influence of actions offered in community centres.
CONCLUSION
In conclusion, the results found in this research suggest that the elderly assisted in the community centre had low depressive symptoms and classification of lifestyle considered very good, yet with poor rated functional fitness. Additionally, the family and friends, alcohol, behaviour, and introspection parameters of lifestyle differ between women and men, with similar results in all functional parameters and depressive symptoms. Altogether, these results point to some possible applications, such as the activities of the community centre that were shown to be efficient in promoting positive behavioural and functional changes may be further optimised, aiming for increment in these parameters. Alternatively, other activities less prone to show positive changes may be less frequent.

