











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
INTRODUCTION
For a good dynamic balance, the integrity structures of the body are necessary, such as bone, cartilage, ligaments and efficient performance of stabilising muscle structures. A deficit in some of these structures may generate a change in dynamic balance. In order to evaluate this balance, the literature has some functional tests such as the Timed Up and Go (TUG) and the Berg Balance Scale that are widely used for balance evaluation, besides the pressure platforms (Kim et al., 2011). Similarly, another widely used instrument is the Star Excursion Balance Test (SEBT), which measures the dynamic balance and quantifies muscle control deficits related to musculoskeletal diseases (Gribble, Hertel, & Plisky, 2012). More recently, the Octobalance® platform has been used to evaluate the dynamic balance of lower limbs. This instrument analyses five different movements of the lower limbs with single limb support to measure the maximum distance reached, resulting in values that qualify their balance (Gonzalo-Skok, Serna, Rhea, & Marín, 2015; 2017). These instruments are used in the general population without any comorbidity, and it is believed that some health conditions may generate changes in the dynamic balance by influencing body structures, such as knee osteoarthritis.
Osteoarthritis (OA) is a degenerative joint disorder with musculoskeletal implications. Its symptoms range from joint pain to crunching, oedema (Burgos-Vargas et al., 2014) and muscle weakness (Minshull & Gleeson, 2017). However, pain is considered the main limiting factor for this condition, directly affecting the activities of daily living (ADL), reducing the quality of life and generating biopsychosocial impacts (Coudeyre et al., 2016).
Considered the main cause of musculoskeletal disability in the world, OA has multifactorial aetiology that may be idiopathic or arise from traumas, congenital formations, postoperative, aseptic osteonecrosis, and metabolic, endocrine and postural disorders that generate direct impact between the joint degeneration and its synthesis (Loures, Góes, Labronici, Barretto, & Olej, 2016).
The knee joint, essential for weight support and balance maintenance, is the most commonly affected (Burgos-Vargas et al., 2014). Individuals with osteoarthritis have a higher proprioceptive loss when compared to people of the same age without the disease (Kim et al., 2011; Tamura et al., 2016), increasing the risk of falls and consequent morbidity (Kim et al., 2011; Takacs, Krowchuk, Goldsmith, & Hunt, 2017). Also, it is known that the deficit of muscle strength, especially of the quadriceps, causes important changes in the knee, contributing to the loss of functionality, in which the reduction of dynamic balance is within this functionality (Alnahdi, Zeni, & Snyder-Mackler, 2012).
Directed evaluations are necessary to receive clinically relevant information. Therefore, the Lower body test is highlighted, which is an adaptation of the SEBT with the insertion of a platform and a cart. However, the execution of this test with people with knee osteoarthritis is not feasible due to the difficulty of the total discharge of weight in a single member, as in the initial protocol. Those people with osteoarthritis have difficulty remaining in single limb support since overloading on only one joint can cause an increase in symptoms, especially pain (McAlindon et al., 2014). Also, because of the deficits of this population, adaptations are necessary so important clinical information is not neglected (Martins, Gonçalves, Mayer, & Schiviski, 2014; Kanko, et al., 2019).
These individuals have difficulty remaining in a single limb position due to all the joint wear and reduction of the strength of the supporting muscles. This deficit is a barrier to evaluating the dynamic balance, so a weight-bearing system was developed to partially reduce the body weight when doing the evaluated movements. Thus, this study hypothesises that the suggested adaptations, with the partial discharge of body weight with a suspension system, make the test feasible and with good reproducibility.
METHODS
This research is a cross-sectional study aimed at evaluating the reproducibility of the Lower Body Test (LBT) through the OctoBalance® (Check your Motion, Albacete, Spain) with partial reduction of body weight through a suspension system in individuals with knee Osteoarthritis.
Sample
Thirty women with a previous diagnosis of knee osteoarthritis were selected. They were screened in an orthopaedic outpatient clinic and classified by x-ray between grades 2 and 4, according to Alback’s classification (Ahlbäck, 1968; Keyes, Carr, Miller, & Goodfelow, 1992).
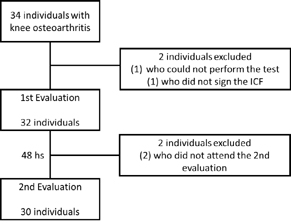
Female individuals aged between 30 and 80 years old, presenting their cognitive functions preserved and available for the evaluation days, were included in the study. Those women who did not agree with the ICF, with previous surgical procedures in the knee or a current indication, and were not able to carry out the evaluations were excluded from the study. The data collection only started after approval by the Ethics Committee in Research with Human Subjects (CEP) of the Universidade Federal de Sergipe (FUS). CAAE: 06219219.3.0000.5546.
Two days of testing were performed, with a 48-hour interval between them, to determine the reproducibility of the test with body weight reduction in individuals with knee osteoarthritis. Participants were also asked not to perform physical activities in the 24 hours before the sessions, so there was no influence of fatigue on the uptake of values (Cramer et al., 2017).
Procedures
The participants were characterised according to age, weight, height, body mass index (BMI, kg/m2), and the graduation of knee osteoarthritis, according to Alback.
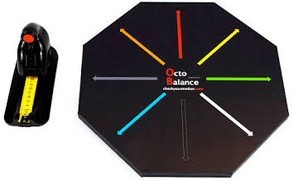
The Lower Body Test was performed using the OctoBalance® (Check your Motion, Albacete, Spain). It is a multidirectional dynamic balance evaluation instrument using coloured arrows to indicate the directions to be evaluated and a metric scale to verify the distance reached in each one (Figure 1). Also, the instrument enables to observe compensations or deviations during the movement since the magnets that connect the platform with the metric scale are sensitive to excessive displacements.
Following the protocol, the length of the lower limbs was measured before the test, with the patients in the orthostatic position, using a tape measure, following the reference of the anterosuperior iliac crest to the medial malleolus. The limb length was used to normalise the measurements of the OctoBalance® (Gonzalo-Skok et al., 2015; 2017).
Before the test, the patients were instructed on the evaluation process. Three measures were taken in each diagonal of familiarisation of the movements, respecting a rest of 30 seconds between them. Then, three more measurements were performed, and all these values were used as results.
The evaluation was performed in four diagonals for each member: 1) Anterior; 2) Medial; 3) Posteromedial; 4) Posterolateral. For the initial performance of the tests, a distance of 20 centimetres was adopted, being able to be reduced to 10 centimetres for those that presented more difficulties.
For greater fidelity, the evaluations were carried out by a single evaluator, and an assistant was responsible for writing the values in an evaluation form. Through the three replicates of each diagonal, the final values were calculated. The average of the values collected in each direction was divided by the length of the member corresponding to each side evaluated and finally multiplied by 100 (Equation 1).
Equation 1 shows the LBT representing the range value relative to the length of the evaluated lower limb, “r” is the range value for each repetition, and LL is the length of the lower limb.
Suspension system
The suspension system was created after previous attempts with no success to perform the test with this population due to their difficulties. This problem has suggested the creation of a suspension system.
This system has two pulleys fixed to the ceiling with a rope of support, with a distance of one meter between them. At one end of the rope, there is an adjustable vest to be worn by the patient, and at the other end, there is a weight with 10% of the body weight placed in the form of washers. Figure 2 shows the scheme used for the suspension system.
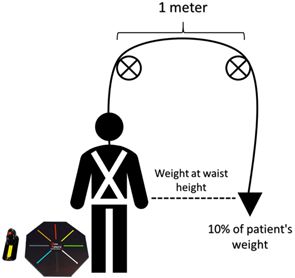
Initially, the patients remained in the orthostatic position. During the evaluation, they were instructed to leave their hands on their waist, so they did not interfere with the upper limbs. The evaluation was done with the movement of the lower limb contralateral to what was being evaluated, pushing the metric scale to the maximum distance reached. First, the right lower limb was evaluated, followed by the left one, with an interval of 1 minute between them. In this way, when the right lower limb was evaluated, it remained in contact with the platform, with support on the black arrow of OctoBalance® (OctoBalance, Check your Motion, Albacete, Spain), and the left limb performed the diagonal anterior movement (red arrow), medial movement (grey arrow), posteromedial movement (blue arrow) and posterolateral (white arrow).
The test was considered invalid when the patient did not obey the following recommendations: 1) do not push the platform abruptly; 2) maintain the balance during the test and be able to return to the initial position; 3) keep the movement rectilinear and diagonally, not loosening the movable platform; 4) keep the hand at waist height; 5) remain the heel of the evaluated limb always supported on the platform.
Statistical analysis
The SPSS software version 22.0 was used for the statistical tests. The data collected were expressed by the mean and standard deviation. The Shapiro-Wilk test was performed to verify normality. The student’s T-Test was performed to verify the possibility of a difference between the groups and to mischaracterize the reproducibility. As for reproducibility indicators, the interclass correlation index (ICI) was calculated using the calculation suggested by Koo and Li (2016). ICI values were considered small when presented up to 0.25, considered low when presented between 0.26 and 0.49, considered moderate between 0.50 and 0.69, considered high between 0.70 and 0.89 and considered very high above 0.90, according to a previous study (Jonson & Gross, 1997). The calculation of the Coefficient of Variation was performed according to the Wang, Olson, and Protas (2002) study with Equation 2:
For the calculation of the estimated standard error (EEE), Equation 3:
and the minimum detectable change (MDD) with 95% confidence interval by Equation 4:
Bland-Altman Graphs were used for visual verification of the agreement between the means. The value of p< 0.05 was adopted as statistical significance.
RESULTS
A total of 30 female individuals with a diagnosis of knee osteoarthritis (age= 59.7± 11.1 years old, body weight= 76.2± 15.2 kg, height= 1.6± 0.1 m and body mass index= 30.7± 6.6) participated in the research. The evaluations performed between the first and second day showed no statistical differences (p-value between 0.09 and 0.84), showing that the learning effect was contemplated previously.
The flowchart of the individuals is shown in Figure 3.
The reliability tests performed demonstrated a very high interclass correlation through the ICI and CV values with a low variation for all the evaluated movements. The EEE and MDD calculations showed positive responses for greater reliability. The values are shown in Table 1.
Table 1 Lower body test values.
| Movements | 1st day | 2nd day | 1st and 2nd day | ||||
|---|---|---|---|---|---|---|---|
| Mean± SD | Mean± SD | p | ICI | CV | EEE | MDD | |
| Anterior – R | 49.94± 4.6 | 47.64± 3.7 | 0.16 | 0.90 | 5.3% | 0.79 | 2.46 |
| Anterior – L | 48.71± 5.3 | 49.28± 5.6 | 0.09 | 0.97 | 5.3% | 0.28 | 1.47 |
| Medial – R | 51.48± 6.3 | 52.19± 6.1 | 0.25 | 0.93 | 6.0% | 0.82 | 2.51 |
| Medial – L | 51.42± 6.8 | 52.32± 6.9 | 0.11 | 0.96 | 5.4% | 0.55 | 2.06 |
| Posteromedial – R | 60.30± 7.6 | 61.10± 7.6 | 0.30 | 0.93 | 6.4% | 1.02 | 2.79 |
| Posteromedial – L | 60.97± 8.8 | 60.83± 9.1 | 0.84 | 0.96 | 5.8% | 0.71 | 2.33 |
| Posterolateral – R | 51.15± 9.7 | 52.05± 8.7 | 0.15 | 0.97 | 6.0% | 0.53 | 2.02 |
| Posterolateral – L | 50.68± 10.8 | 51.41± 10.6 | 0.09 | 0.99 | 4.2% | 0.21 | 1.28 |
R: right; L: left; SD: standard deviation; p: T-test, ICI: interclass correlation index; CV: coefficient of variation; EEE: estimative standard error; MDD: minimum difference detectable.
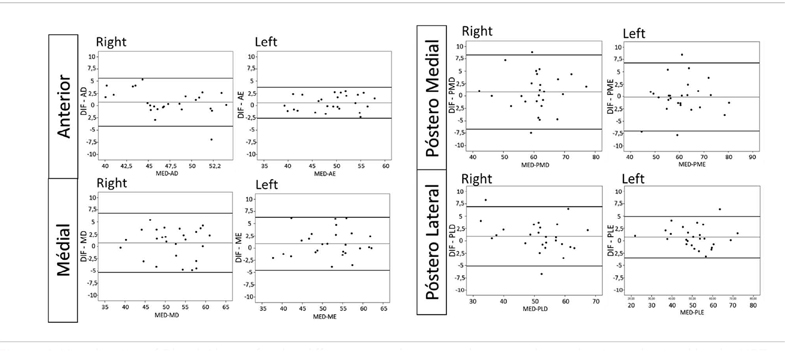
The Bland-Altman graphs showed agreement between the means, presented in Figure 4. A bias range close to zero and an acceptable agreement interval between the evaluations and practically all patients evaluated within the confidence limits were observed.
DISCUSSION
This study aimed to verify the reproducibility of the Lower Body Test performed with Octobalance®, for individuals with knee osteoarthritis. The main finding of this study was the confirmation of reproducibility with suggested adaptation, verified by high values of ICI, low CV, and good agreement, and Bland-Altman charts were considered satisfactory.
Reproducibility studies have proved sufficiently capable of demonstrating the efficacy of similar tests (Plisky et al., 2009; Murray, Salvatore, Powell, & Reed-Jones, 2014). There is variability between how many repetitions are necessary to obtain good results in the literature. Unlike Gribble, Tucker, and White (2007), who performed 3 replicates at one-week intervals, this study showed reliable results with only two replicates within a 48-hour interval between them, potentially being simpler and more agile in obtaining results (Gribble et al., 2007). Also, the study by Kanko et al. (2019) showed the same for the same population studied but with another balance test.
Performing only two repetitions can be explained through the adaptive neuromuscular process of the patients. Also, emotional factors such as fear may have been reduced, increasing safety and overcoming ability. During the reproducibility of the 6-minute walk test, several authors (Redelmeier, Bayoumi, Goldstein, & Guyatt, 1997; Rodrigues, Viegas, & Lima, 2002; Lacasse, Goldstein, Lasserson, & Martin, 2006) showed that it is possible to obtain good results with two tests, and there is no statistically significant difference between them through the learning process.
Another relevant factor was the characteristics of this sample, which had mostly individuals with high BMI. A recent study showed that being overweight is directly linked to a deficit of balance and, consequently, functionality, making it essential to adapt to this study. Also, senescence is directly related to the advancement of osteoarthritis and loss of function, as seen in the studies of Rebelatto, Calvo, Orejuela, and Portillo (2006) and Shane Anderson and Loeser (2010).
Among the analyses carried out, the values of the minimum detectable difference were highlighted that despite not generating reproducibility indicators, they demonstrated important data for clinical and labour practice (Haley & Fragala-Pinkham, 2006; Paço & Cruz, 2011). Therefore, through a reassessment with this instrument for individuals with knee osteoarthritis, satisfactory modifications will only be demonstrated with clinical improvements and values above the MDD.
CONCLUSIONS
It is reproducible to perform the Lower Body Test with the Octobalance® platform to evaluate the dynamic balance of lower limbs in women with knee osteoarthritis.
It was also possible to identify values of minimum detectable difference, values to be used as a form of prognosis and improvement of these individuals.

