











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
COVID-19 prevention is possible, especially if all health recommendations are followed (National Department of Health in Mexico [SSA, by its acronym in Spanish], 2021). Preventive behaviors, such as social distancing and frequent handwashing, among others, depend greatly on people’s risk perception associated with the disease, and past experiences have shown that health policies’ success relies greatly on the accuracy of the people’s perception of risk (Cori et al., 2020; Dryhurst et al., 2020).
In health research, risk perception has commonly been assessed whilst exploring the individuals’ estimated likelihood of developing a disease or a medical condition. In this context, likelihood is usually expressed and measured through projected percentages or using verbal categories such as "probable" or "improbable", which compel the individuals to think of risk in a complex manner. In other words, using logical principles expressed in terms of quantities. This conception of risk perception suggests that people assess risk through a merely rational process (Dillard et al., 2012; Hay et al., 2014, 2016; Loewenstein, 2001). However, various authors have highlighted the central role feelings and emotions play in risk assessment, including decision-making and behavior (Loewenstein et al., 2001; Slovic et al., 2002). Anticipatory emotions, defined as those immediate visceral reactions (e.g. fear, anxiety or dread) experienced during the risk assessment process and uncertainty, may differ from the cognitive evaluation itself, exerting control over it and directly influencing behavior (Loewenstein, 2001). According to Hay et al. (2014, 2016), considering feelings involved in the process of risk assessment could stand for a much more integral and effective measure in explaining specific health-related behaviors.
Consequently, risk perception is a feeling-of-risk measure that reliably represents a “gut feeling”, which acts as a kind of intuition or personal heuristic people use to evaluate perceived health-related risks. These unpleasant feelings associated with risk, or intuition, in combination with risk appraisal, is called by Hay et al. (2005, 2014) Intuitive Risk Perception (IRP), which has been studied in the context of chronic diseases like cancer.
In addition, it has been proposed that the experience of anxiety and fear during risk assessment affects people's judgment and their perception of risk, thus increasing preventive behaviors in risky situations, including avoidance (Bechara et al., 1997; Lerner & Keltner, 2000; Maguire et al.., 2019). The assessment process in anxiety involves the presence of constant and elaborate worries, which define rumination, and comprise catastrophic imaging and intolerance of uncertainty as some of the central features of anxiety (Clark & Beck, 2010). Therefore, the construct of IRP could be closely linked to cognitive symptoms of anxiety, in particular chronic and excessive worry. Moreover, as stated by the cognitive approach, the impact of these cognitive processes could be reflected through somatic symptoms of anxiety (Kaltsas & Chrousos, 2007; Singh & Sahni, 2000). Taken as a whole, anxiety and worry could well have accompanied IRP during the COVID-19 outbreak.
Regarding risk perception and COVID-19, studies have focused on evaluating the influence sociodemographic factors, such as sex, age and educational level, have had on risk perception during the pandemic, showing it to be higher in women (Guzmán-Gonzalez et al., 2020; Zeballos-Rivas, et al., 2021), younger ones (Kim & Crimmins, 2020), and in those individuals with higher education (Ding et al., 2020). With respect to affect and emotions, it has been found that higher risk perception is associated with higher levels of negative emotions, such as anxiety, nervousness (Han et al., 2021), fear and worry; the last two have been shown to be good predictors of confinement behavior (Uribe-Alvarado et al., 2020). In the case of Mexico, it has been reported that the presence of worry related to the consequences of COVID-19, as well as the derived emotional effects, increased as the pandemic evolved (Lugo-González et al., 2021).
According to Han et al. (2021), it has become necessary to develop adequate instruments to have a more comprehensive measure of COVID-19 related risk perception.
IRP has proven to be a valid construct addressing chronic diseases in diverse populations within the US (Hay et al., 2014, 2016). It could also be employed, therefore, in understanding risk perception related to communicable diseases, such as COVID-19, considering that both represent a direct threat to physical health and life itself.
Additionally, in contrast with cancer, the current pandemic caused by COVID-19 represents a novel situation, a condition that tends to increase the general perception of risk associated with an event (Sjöberg, 2000). Thus, the purpose of the present study was to adapt and validate the COVID-19 Risk Belief Scale and evaluate Intuitive Risk Perception and its relation with somatic anxiety and worry in a group of Mexican adults during the COVID-19 outbreak in Mexico City.
Method
Participants
Data of 694 respondents was analyzed (77% women), with ages ranging between 18 and 74 years old ( X = 33.44 ± 13.47). All participants were living in Mexico City (600) and the Metropolitan area (94) when data was collected. Formal education was distributed as follows: 2.16% had completed elementary school and junior high, 31.7% high school, 45.24% university and 20.89% postgraduate school (masters and PhD). Regarding occupation, 44.5% were employed, and 42.8% were students, while the rest were distributed between self-employed (8.36%), unemployed (2.59%), working from home (2.02%), or retired (.72%).
Only 5.62% had previously been diagnosed with COVID-19, whilst 68.16% reported a family member or close friend being sick with COVID-19. Of the 694 participants, 84.58% reported consulting information related to COVID-19. Of these, 53.89% reported doing it frequently and only 21.47% reported almost never consulting information, whilst 1.15% reported never doing so. The most frequently consulted media were official websites (80.69%), electronic media (76.51%), social networks (68.01%), national healthcare department conferences (37.75%), radio (34.73%), daily government press conferences (26.95%), and printed media (25.5%).
Measures
COVID-19 risk belief scale. The Spanish version of the Cancer Risk Beliefs Scale (Hay et al., 2016) was adapted to explore intuitive risk perception specifically related to COVID-19, with all 25 items culturally adapted for the Mexican population. Although these diseases are different in nature, cancer and COVID-19 represent a threat to one’s integrity and life, and therefore the scale proposed by Hay et al. (2014) may be well suited for evaluating COVID-19-related risk. The scale explores both the cognitive and the emotional aspects of risk perception. According to Hay et al. (2014), this could be a better-suited measure to explain why people engage in health preserving behaviors, which is the case of COVID-19. Original dimensions of intuitive risk perception were considered for the validation process (Hay et al., 2014). These included: a) cognitive causation (CC), related to the belief that thinking about a given disease can actually cause it and, on the other hand, that minimizing such thoughts can avoid its occurrence, thus acting as a protective mechanism based on cognitive avoidance; b) negative affect in risk (NA), which refers to the unpleasant feelings, mainly fear, generated during the risk process; c) unpredictability (UN), related to a perceived uncertainty associated with the possibility of getting sick; d) preventability (PR) which evaluates beliefs regarding the degree of one’s perceived control over the development of a given disease; and e) defensive pessimism (DP), referring to negative consequences of being “too optimistic” about one’s ability to avoid the disease. Each item explores the participants’ level of agreement in risk related statements within the context of the COVID-19 pandemic and is coded in a four-option categorical scale (strongly disagree, disagree, agree, strongly agree).
Penn State Worry Questionnaire, PSWQ. This explores the cognitive dimension of anxiety through the presence and level of intrusion of worry in everyday life. All 16 items are coded in a five-point scale reflecting the frequency associated with each statement ranging from never to always (Meyer et al., 1990). The questionnaire has shown good internal consistency (α = 0.93) and test-re-test reliability (r = 0.92, p < .001). Scores range from 16 to 71 with a mean and standard deviation of 41.70+10.97 (Padros-Blazquez et al., 2018).
Beck Anxiety Inventory, BAI. BAI is a measure of somatic response associated with anxiety. It consists of 21 items coded in a four-point scale that reflects the intensity of the symptoms associated with each statement, ranging from Little or Nothing to Severe. The instrument has already been validated and standardized for the Mexican population, showing good internal consistency (α = 0.83) as well as test-retest reliability (r = 0.75). Furthermore, scores ranging from 0-21 for low anxiety, 22-35 for moderate anxiety, and >36 for severe anxiety have been established (Robles et al., 2001).
Procedure
Prior to scale administration, the Spanish version of the Risk Belief Scale, originally adapted in Haitian-Creole and Spanish-Speaking Populations in the US, was culturally adapted to the Mexican population and the context of the COVID-19 pandemic by two trained health psychologists who were native Spanish speakers. This ensured that each statement was clear and understandable for all people, regardless of educational background, whilst carefully keeping the original sense within the five factors.
Google Forms platform was used for an initial pilot with the inclusion of 38 undergraduate Psychology students from a public university in Mexico City. Their responses to the complete survey were tested, and potential problems with the instrumentation not attributable to the instrument itself were identified. Slight adjustments were made to the on-line version of the survey, which focused mainly on its visual appearance and enhancing the clarity of instructions.
The final survey, comprising sociodemographic variables and the three psychometric scales, was launched through an open electronic link and disseminated via email and social media platforms containing an invitation to participate along with a careful description of the research aims and instructions for answering each scale. To address the ethical issues, procedures complied with the ethical norms in Mexico. The study was reviewed and approved by the research committee of the National Pedagogic University (UPN) in Mexico under registration number 23/2021.
Participation was voluntary and informed consent was obtained through initially asking: “Do you accept to participate in this research responding the survey?” If accepting, participants were asked to click on a yes or no box, after which they could complete the questionnaire; if refusing, the survey was automatically terminated. Anonymity and confidentiality were always guaranteed. All procedures were non-invasive, and no harm was induced because of participation in the study. Nevertheless, with the purpose of ensuring participants’ well-being, information relating to the minimal risks associated with mild discomfort was provided and options for addressing them were offered. These included the option to quit the study at any time and providing contact information pertaining to the research team in case any participant needed to discuss doubts and/or tackling any concerns. No person reported concerns of this kind. Of all approached participants, only one refused to complete the survey. Conflicting interests were considered and reviewed, and none emerged. Data was collected between November 11th and November 13th, 2020, and analyzed using the STATA statistical software package, version 14.1 (StataCorp, College Station, Texas). For analyses, duplicated questionnaires were identified and excluded, making a total of 2.1% from the original sample.
Analyses
To determining construct validity of the COVID-19 Risk Belief Scale, an initial confirmatory factor analysis (CFA) was performed based on the original model proposed by Hay et al. (2014). Alpha and omega coefficients of reliability were calculated for each dimension of the scale, and correlation matrices among items were carefully analyzed seeking to keep both coefficients between 0.7 and 0.9 in order to avoid redundancy or identify poor correlations. Items showing the highest and the lowest correlation indices were extracted from the instrument, as well as items that were negatively correlated with the rest. A second CFA was carried out after item selection considering the following parameters as good fit indices: non-significant values of X2 (Barrett, 2007), Root Mean Square Error of Approximation (RMSEA) values smaller than .06 (Hu & Bentler, 1999; Steiger & Lind, 1980); Comparative Fit Index (CFI) values ≥ 0.95 (Hu & Bentler, 1999; Pituch & Stevens, 2016); Tucker-Lewis coefficient (TLI) values above 0.9 (Pituch & Stevens, 2016) and Root Mean Square Residual (RMR) < .05 (Byrne, 1998; Diamantopoulos & Siguaw, 2000).
Additionally, reliability was tested through obtaining both alpha and omega coefficients for the total scale and each dimension of intuitive risk perception.
Skewness and kurtosis tests for normality were applied to each study variable and Spearman’s correlations between risk perception and cognitive and somatic anxiety were performed given the categorical nature of the scales. Association between IRP and sex and education were explored using Kruskal-Wallis, and correlation between IRP and age was also tested through Spearman’s rho. Descriptive data were finally obtained for Intuitive Risk Perception, as well as for cognitive and somatic anxiety.
Results
Confirmatory factor analysis including the original 25 items through five dimensions yielded unsatisfactory goodness-of-fit indices (X2 = 1565.9, df = 265, p < .001; RMSEA = 0.084, CI [0.080, 0.088]; CFI = 0.86; TLI = 0.85; SRMR = 0.08) and Alpha (CC = 0.93, NA = 0.91, UN = 0.73, PR = 0.47 y DP = 0.67) and omega coefficients (CC = 0.93, NA = 0.92, UN = 0.76, PR = 0.48) were then calculated and showed redundancy in cognitive causation and negative affect in risk. The omega coefficient for defensive pessimism could not be calculated given the number of items included in this dimension. The correlation matrices for each latent variable were then analyzed and items 3 (CC), 6 (CC) and 9 (NA) were extracted, since they showed r coefficients above .70 with the rest of the items in their dimension. Item 21 was also excluded from the final structure, as it negatively correlated with the rest of the items in its dimension. Items 17 (UN), 20 and 22 (PR) were also eliminated, since correlation coefficients with other items in the latent variable were close to zero. A second CFA including the remaining 18 items and the same factorial distribution showed adequate goodness-of-fit indices, except for the X2 (X2 = 426.8, df = 125, p < .001; RMSEA = 0.059, 90% CI [0.053, 0.065]; CFI = 0.95; TLI = 0.94; SRMR = 0.04). The final CFA is shown in Figure 1 and coefficients for each item of the final version are shown in Table 1.
Table 1 shows β coefficients and confidence intervals for all 18 items, as well as the α coefficients of each latent variable.
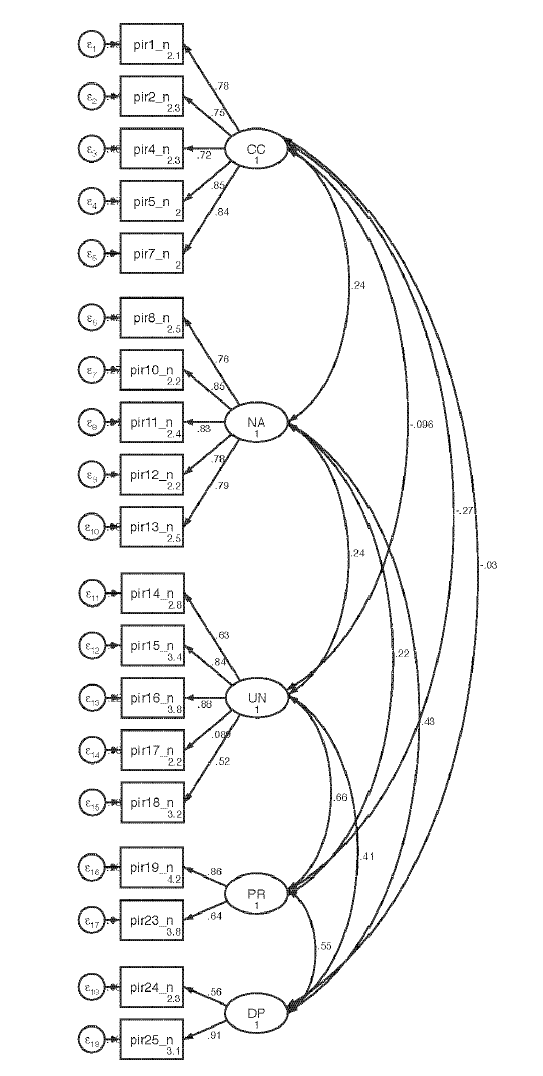
Table 1 β coefficients for the final 18-item scale and α and ( coefficients for each latent variable.
| Item | β | 95% CI | Cronbach α | McDonald’s ( |
| 1 | 0.78 | [0.75, 0.82] | ||
| 2 | 0.75 | [0.71, 0.79] | CC | CC |
| 4 | 0.72 | [0.68, 0.76] | 0.89 | 0.89 |
| 5 | 0.85 | [0.83, 0.88] | ||
| 7 | 0.84 | [0.81, 0.87] | ||
| 8 | 0.76 | [0.72, 0.79] | ||
| 10 | 0.85 | [0.83, 0.88] | NA | NA |
| 11 | 0.83 | [0.80, 0.86] | 0.90 | 0.90 |
| 12 | 0.78 | [0.74, 0.81] | ||
| 13 | 0.79 | [0.76, 0.82] | ||
| 14 | 0.63 | [0.58, 0.68] | ||
| 15 | 0.84 | [0.81, 0.87] | UN | UN |
| 16 | 0.88 | [0.85, 0.91] | 0.80 | 0.82 |
| 18 | 0.52 | [0.46, 0.58] | ||
| 19 | 0.86 | [0.81, 0.91] | PR | |
| 23 | 0.64 | [0.58, 0.69] | 0.71 | |
| 24 | 0.56 | [0.49, 0.63] | DP | |
| 25 | 0.91 | [0.84, 0.99] | 0.67 | |
| Total scale coefficients | ||||
| 0.82 | 0.71 | |||
Note: CC = Cognitive Causation, NA = Negative Affect, UN = Unpredictability, PR = Preventability, DP = Defensive Pessimism. Omega (() coefficients for PR and DP could not be calculated given the number of items included.
Table 2 shows standardized covariance coefficients between latent variables highlighting significant and moderate values: defensive pessimism with negative affect, unpredictability and preventability, and unpredictability with preventability.
Table 2 Covariance coefficients between latent variables of the COVID-19 Risk Belief Scale.
| Latent Variables’ Covariance | Standardized cov | 95% CI |
| CC, NA | 0.24* | [0.16, 0.32] |
| CC, UN | -0.10 | [-0.18, -0.02] |
| CC, PR | -0.27* | [-0.35, -0.18] |
| CC, DP | -0.03 | [-0.12, 0.05] |
| NA, UN | 0.24* | [0.16, 0.32] |
| NA, PR | 0.22* | [0.13, 0.30] |
| NA, DP | 0.43* | [0.35, 0.51] |
| UN, PR | 0.66* | [0.60, 0.73] |
| UN, DP | 0.41* | [0.34, 0.49] |
| PR, DP | 0.55* | [0.48, 0.63] |
Note: CC = cognitive causation, NA = negative affect, UN = unpredictability, PR = preventability, DP = defensive pessimism. * p < .001.
The median score of global intuitive risk perception from all participants was 44 (P25= 39, P75 = 48; min = 18, max = 72), considering a scale ranging from a possible minimum of 18 and a maximum of 72 points. Table 3 shows the descriptive data for each dimension of the scale.
Table 3 Global scores on the five dimensions of the COVID-19 Risk Belief Scale (N = 694).
| Dimension | Median | (min - max) | Percentile 25,75 |
| Cognitive causation | 7 | (5 - 20) | 5, 10 |
| Negative affect | 11 | (5 - 20) | 9, 15 |
| Unpredictability | 12 | (4 - 16) | 11, 14 |
| Preventability | 7 | (2 - 8) | 6, 8 |
| Defensive pessimism | 5 | (2 - 8) | 4, 6 |
Note: CC = cognitive causation, NA = negative affect, UN = unpredictability, PR = preventability, DP = defensive pessimism. * p < .001.
The global score of the COVID-19 Risk Belief Scale for the Mexican population was correlated using Spearman’s correlation coefficients (N = 694) with those of the PSWQ (r = 0.32, p < 0.001) and BAI (r = 0.41, p < 0.001), given that none of the study variables distributed normally according to the skewness and kurtosis tests performed (p < .001).
When correlating the global scores of worry and somatic anxiety with each dimension of Intuitive Risk Perception, only associations between cognitive causation and PSWQ, and that between preventability and BAI scores appeared not statistically significant. The rest of the correlations were statistically significant, with the highest coefficients seen for negative affect and both dimensions of anxiety. Results are displayed in detail in Table 4.
Table 4 Spearman’s correlations between dimensions of IRP and cognitive and somatic anxiety.
| Variables | Spearman’s rho | |
| Cognitive Causation | Worry | 0.02 |
| Somatic anxiety | 0.11* | |
| Negative Affect | Worry | 0.39** |
| Somatic anxiety | 0.46** | |
| Unpredictability | Worry | 0.14** |
| Somatic anxiety | 0.18** | |
| Preventability | Worry | 0.12** |
| Somatic anxiety | 0.07 | |
| Defensive Pessimism | Worry | 0.16** |
| Somatic anxiety | 0.15** | |
Note: *p < .01, **p < .001
Median scores of PSWQ were 48 (P25 = 38, P75 = 60, min. = 19, max. = 80), whilst BAI showed a median of 10 (P25 = 4, P75 = 21; min. = 0, max. = 60).
To determine if the differences in intuitive risk perception were statistically significant across sex, a Mann Whitney test for unpaired samples was carried out, resulting in a significant higher perception of risk (p < .001) amongst women ( 𝑋 = 43.9, SD = 7.93) in contrast with men ( 𝑋 = 41.37, SD = 8.09, Rosenthal’s R = -0.12). Regarding education, a median test for k independent samples showed no significant differences between groups (X2 = 2.80, p = 0.59). Finally, Pearson correlation revealed a poor negative association between IRP and Age (r = -0.13, p < .001). This analysis was chosen since age was computed as a numeric variable and is supported by Spearman’s coefficient (rho = -0.15, p < .001), which means that perception of risk tends to decrease as age increases.
Discussion
The main purpose of this study was to evaluate the intuitive risk perception and its relation to somatic anxiety and worry in a group of Mexican individuals during the COVID-19 outbreak in Mexico City. This was done after confirming the validity and reliability of the COVID-19 Risk Belief Scale in its Spanish version for Mexican population. Data derived from the final CFA supported the five-factor structure originally proposed by Hay et al. (2014) for studying cancer-related risk perception in the US population; and showed that it could also be a valid measure for studying intuitive risk perception associated with the COVID-19 pandemic.
Global scores distribution in this sample showed a rather moderate risk perception associated with the COVID-19 pandemic. This was the case even when, at the moment of data collection, Mexico was experiencing high rates of morbidity and mortality, which were exponentially increasing day after day. These findings are supported by Uribe-Alvarado et al. (2020), who found that a high proportion of participants reported low or no concerns at all about either getting sick of COVID-19 or being able to receive medical care if needed.
In a more detailed analysis of the scale, the fact that cognitive causation represents the principal dimension explaining risk perception is supported by research literature, which defines this construct mainly as a cognitive process, consisting in the appraisal of a real or potential danger or threat (Cori et al., 2020). As stated by previous studies, this appraisal depends greatly on the presence and magnitude of diverse factors directly linked to a given threat, such as availability of information. In many cases, access to such information is determined by mass media exposure, which tends to increase risk perception as the frequency of media coverage increases (Sjöberg, 2000). This has also been observed in the case of disease-related information (Young et al., 2013). In this study, respondents exhibited mild to total disagreement with the fact that thoughts can cause the illness or, by contrast, that minimizing such thoughts could prevent it, taking responsibility away from thoughts on the chances of getting sick.
The tendency of the average scores on negative affect in this study showed that, even when there was evidence pointing to COVID-19 as a global health crisis, negatively affecting a great proportion of people worldwide (WHO, 2021) and specifically in Mexico (SSA, 2021), the majority of participants surveyed did not seem to exhibit high levels of fear or discomfort associated with the idea of getting sick. These results were somewhat unexpected, given the magnitude of the problem.
According to a study conducted in Mexico, emotions like fear can lead people’s decisions towards confinement and prevention of contagion (Uribe Alvarado et al., 2020). Therefore, it would be expected to find higher responses of fear among the community. Nevertheless, in this case, the affective response associated with COVID-19 was rather moderate. One possible explanation for this is that participants in our study did not perceive themselves as vulnerable, which could in turn interfere with preventing behaviors. (Perez de Celis-Herrero & Cavazos-Arroyo, 2021).
In general, the unpredictability factor showed a response trend of uncertainty associated with the possibility of getting COVID-19, pointing to a marked difficulty in predicting its occurrence. Similar to Hay's finding on cancer (2014), part of the sample agreed that anyone can get COVID-19 no matter what they do.
The preventability factor, which comprises items 19 and 23, refers to the fact that COVID-19 can be prevented if specific health recommendations are followed, making it a controllable disease. The low correlation found in this sample between item 21 and the rest of the items of preventability dimension could be explained by the fact that participants did not consider following healthy lifestyles as protective factors to prevent COVID-19. This finding seems rather logical considering that COVID-19 contagion, unlike cancer, does not seem to depend greatly on the adoption of healthy habits or lifestyle.
According to our findings, people tend to think that COVID-19 contagion cannot be predicted. However, the common perception seems to be that its occurrence can be prevented through specific strategies, such as social distancing, using masks, reducing exposure by confinement, and handwashing. This is consistent with the findings of Lugo-González et al. (2021), who found a high perception of control to prevent contagion in their participants, which can be reflected through the above-cited strategies.
Regarding the defensive pessimism factor, participants agreed with statements about how risky being very optimistic over avoiding COVID-19 can turn out to be. The implications are that this type of belief can reduce people’s ability to estimate a real risk (Hay et al., 2014).
In this study, people exhibited a tendency to think that it was appropriate to commit to the idea of an increased probability of getting sick as a coping strategy. In accordance with these ideas, Young, et al. (2013) found that high media coverage associated with a given disease usually tends to increase unrealistic pessimism, which refers to the perception of a high probability of getting a disease regardless of its actual incidence or severity. It seems reasonable to consider that both concepts, unrealistic pessimism and defensive pessimism could be positively correlated. Here, it could lead individuals to reduce the frequency of behaviors aimed at preventing contagion. It would be useful to determine the impact of defensive pessimism as a specific prevention strategy.
Regarding the correlation between COVID-19 Risk Belief Scale and the BAI and PSWQ, global scores of all measures showed a modest positive association, which was slightly greater in magnitude with the BAI scores. This association between risk perception and both the somatic and cognitive components of anxiety was expected considering the nature of these three constructs.
In the case of BAI, its association with IRP provides evidence to support the idea of an empirical relation between both responses. This relation could reflect the influence of affective processes over risk assessment, either in risk perception or in the anxiety response itself. This hypothesis finds additional support in the positive association found between global scores of cognitive and somatic anxiety and negative affect in risk, which was higher than that found between intuitive risk perception as a whole and both the BAI and PSWQ measures.
On the other hand, the association observed between risk perception and worry can be explained, since both constructs represent mainly cognitive processes, which rely on the assessment and anticipation of an imminent threat or danger. In addition to the evidence provided by Hay et al. (2014), relative to the advantage of using the Cancer Risk Belief Scale over traditional measures of risk perception in assessment, the moderate association found in the present study between the COVID-19 Risk Belief Scale and the BAI and PSWQ indicates minimal overlap among intuitive risk perception and anxiety response. This thus discloses additional evidence to empirically separate one concept from the other, even when both of them could be present in the face of a perceived threat.
Given that defensive pessimism showed the highest covariances with most of the other latent variables, it is possible that this factor modulates the changes observed in preventability, unpredictability, and negative affect. Regarding preventability, we could hypothesize that being overconfident about avoiding getting sick would imply a certain level of awareness, eliciting specific behaviors aimed at avoiding contagion, thus suggesting the idea that COVID-19 can be prevented. On the other hand, even when contagion can be prevented, our findings showed that people perceive the disease as an unpredictable event. Thus, it would be necessary for people to follow preventive measures consistently to avoid contagion, which would explain the high relation between defensive pessimism and unpredictability. Nonetheless, further information is needed to support the link between both defensive pessimism and unpredictability and preventive behaviors. Finally, the constant awareness derived from the possibility of being infected could explain the presence of constant fear or dread, comprising negative affect. However, this response remained moderate in our study, probably due to the idea that prevention depends greatly on specific actions taken and not on random factors; or even on the influence people’s ideas or thoughts have on the occurrence of certain events, as stated by cognitive causation.
Lastly, with respect to sociodemographic variables, our findings showed higher intuitive risk perception among women and younger people, which is in line with previous studies (Kim & Crimmins, 2020; Zeballos-Rivas, et al. 2021). Nevertheless, we did not find any significant difference in risk perception across educational level, which was probably due to heterogeneous groups.
While evaluating the results of this study, several limitations should be taken into consideration regarding data collection procedures. Firstly, most participants were women with at least a university degree, which could have biased the results. Despite these limitations, findings derived from previous studies seem to share these same selection biases (Guzmán-González et al., 2020; Lugo-González et al., 2021), which could indicate that women as well as individuals who have received higher education seem to be more willing to participate in these studies. Even so, the carrying out of randomized studies is recommended in the future. It would therefore be advisable to access greater national representation in subsequent studies, to discern how the general population actually behaves.
Online data collection procedures can pose some technical limitations, such as missing data due to duplicated or incomplete questionnaires. There can, moreover, be selection biases due the absence of electronic devices or a lack of access to the Internet for a great proportion of people in Mexico. Despite such circumstances, these procedures nonetheless presented a great advantage, especially when considering the current, critical global health situation, which has made personal collection data extremely difficult.
Conclusions
Our findings contribute to the understanding of how people evaluate risk within the context of a communicable disease caused by SARS-CoV-2. Differing from cancer in its causes and effects, such findings constitute evidence that favors Intuitive Risk Perception’s utility as a construct, which considers affective elements deemed as gut-feelings, not only for non-communicable diseases but also for communicable ones.
This study confirms the importance the affective component has within the risk assessment process through intuitive risk perception that, in contrast to categorical measures expressed in a probabilistic way, tends to confuse respondents, and consider risk perception only as a rational process.
Additional research on the subject within Mexican culture is clearly needed for developing explanatory perspectives aimed at establishing possible causal relations among intuitive risk perception and preventive behaviors. This is especially so in the context of the ongoing global pandemic. Hence, behavioral intervention programs and public policy designs aimed at counteracting the effects of people’s demeanor in the evolution of COVID-19 might benefit from such an approach.
Credit authorship contribution statement
Edgar Salinas-Rivera: Conceptualization, Investigation, Formal analysis, Methodology, Project administration, Writing - original draft. Héctor Velázquez-Jurado: Conceptualization, Investigation, Formal analysis, Writing - original draft. Carlos G. Castro: Formal analysis, Writing - original draft. Juan Manuel Rico-López: Formal analysis, Writing - review & editing.

