











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
Introduction
Secondary transport is increasingly common and necessary due to the lack of human or technical resources for the continuity of care at the healthcare center of origin; however, it may result in risks during care transfer. The need for secondary transport emerges as a result of the limited number of beds at specialized units, the inability to provide care from certain specialties, and the lack of complementary techniques for differential diagnosis (Eiding et al., 2019; Mueller et al., 2019; Kiss et al., 2017; Markakis et al., 2006). Secondary transfer involves risks both for the patient and for the care team performing the transfer, and careful risk-benefit analysis is needed to justify the transfer (Ordem dos Médicos (Colégio de Medicina Intensiva) & Sociedade Portuguesa de Cuidados Intensivos, 2023; Dabija et al., 2021; Ramgopal, 2020; Eiding et al., 2019; Markakis et al., 2006). Whatever method of transport is used, patient assessment instruments for secondary transport are needed to improve decision-making and the subsequent planning of the transfer (Markakis et al., 2006).
Decision-making regarding secondary transport has an impact on subsequent transport planning and execution in terms of the healthcare team and mode of transport to be assigned (Abdelmawla et al., 2021; Conde et al., 2021; Grass et al., 2020; Kiss et al., 2017). To promote successful transfers, these decisions must always be based on the best available scientific evidence, that is, with recourse to specific, validated instruments, and must always involve a careful assessment of the patient and potential complications that may occur en route (Abdelmawla et al., 2021; Grass et al., 2020). Decision-making and transport planning must be well structured and based on reliable assessment instruments, to put in place specialized teams of trained professionals for each type of transfer (Abdelmawla et al., 2021).
While some universally implemented instruments are available for evaluating clinical severity (Abdelmawla et al., 2021; Veldhuis et al., 2021; Grass et al., 2020), considerable disparities remain in the early identification of potentially high-risk patients. It is essential to optimize this assessment, as early detection of patients with severe conditions may result in the timely administration of life-saving interventions and care and, consequently, in successful transfers (Veldhuis et al., 2021). Given the difficulty of predicting which patients are likely to present deterioration during transport, and given the challenge of identifying high-risk patients, several instruments have been developed to predict high-risk illness (Abdelmawla et al., 2021; Veldhuis et al., 2021; Grass et al., 2020). However, the accuracy and applicability of risk stratification instruments must be evaluated in each type of population, as age and gender are also important factors to be considered (Veldhuis et al., 2021).
Therefore, secondary transport must be supported by a system providing for a series of structured processes with the active intervention of different elements of the healthcare system to provide rapid, effective action to ensure the quality and safety of care provision during transfer (Gabinete do Secretário de Estado Adjunto e da Saúde, 2016). Due to the specialization of care and the technical differentiation of care provision, it is important to promote the normalization of recommendations and best practices in secondary transport, aiming to achieve continuous quality improvement in patient transfers (Ordem dos Médicos (Colégio de Medicina Intensiva) & Sociedade Portuguesa de Cuidados Intensivos, 2023), hence the importance of studying this subject.
Secondary transport occurs due to the need to provide higher level care, or to carry out complementary diagnostic and/or therapeutic tests, which cannot be performed in the institution where the patient is located (Ordem dos Médicos (Colégio de Medicina Intensiva) & Sociedade Portuguesa de Cuidados Intensivos, 2023).
Secondary patient transfer between healthcare facilities is becoming increasingly frequent and represents a critical element of the healthcare system (Dabija et al., 2021; Ramgopal, 2020).
Risk stratification and the anticipation of potential complications are increasingly important in patient care during transportation (Ordem dos Médicos (Colégio de Medicina Intensiva) & Sociedade Portuguesa de Cuidados Intensivos, 2023; Grass et al., 2020; Ramgopal, 2020; Markakis et al., 2006). The risk assessment must be based on validated instruments for evaluating severity according to physiology and short-term health conditions (Grass et al., 2020).
This study aimed at mapping the scientific evidence on patient assessment instruments for secondary transport. Thus, the following research question emerged: What are the existing patient assessment instruments for secondary transport?
1. Methods
This scoping review used the “population, concept, context” framework set out by the Joanna Briggs Institute (JBI) (Peters et al., 2021). The study is reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) checklist (Page et al., 2021).
To gather all published and unpublished studies, the search strategy for the database followed the three-step process described by the JBI (Peters et al., 2021): population (critically ill patients), concept (assessment instruments), and context (secondary transport).
A protocol registration of scoping review was carried out in Open Science Framework, entitled “Patient assessment instruments for secondary transport: protocol for a scoping review”, with Registration DOI: 10.17605/OSF.IO/ATQPE, available in Internet Archive link: https://archive.org/details/osf-registrations-atqpe-v1.
This scoping review complies with the international research standards stipulated in the World Medical Association Declaration of Helsinki (2013). As a scoping review without the participation of human beings, it is exempt from the need for approval by an ethics committee.
An initial search was limited to the MEDLINE database (via PubMed) to identify the descriptors used to classify articles and to evaluate the search terms used through analysis of the words included in titles and abstracts. In the second stage, using the descriptors identified, a search was conducted on the following databases: MEDLINE (via PubMed), CINAHL Complete (via EBSCOhost), Cochrane, Scielo, and LILACS. In the third stage, the RCAAP, DART-Europe, and OpenGrey databases were searched to identify articles from the grey literature. The reference lists of the articles identified and relevant websites from this field of research were also considered.
Table 1 presents a detailed description of the process followed for the search strategy.
Table 1 Search strategy
| Strategy | Database | Results |
|---|---|---|
| (((Surveys[Title/Abstract] AND Questionnaires[Title/Abstract]) OR (Surveys and Questionnaires[MeSH Terms])) AND ((Risk Assessment[Title/Abstract]) OR (Risk Assessment[MeSH Terms]))) AND (((Transportation of Patients[Title/Abstract]) OR (Transportation of Patients[MeSH Terms])) OR ((Patient Transfer[Title/Abstract]) OR (Patient Transfer[MeSH Terms]))) | MEDLINE | 113 |
| (((TI Surveys and Questionnaires) OR (AB Surveys and Questionnaires) OR (MH Surveys and Questionnaires)) AND ((TI Risk Assessment) OR (AB Risk Assessment) OR (MH Risk Assessment))) AND (((TI Transportation of Patients) OR (AB Transportation of Patients) OR (MH Transportation of Patients)) OR ((TI Patient Transfer) OR (AB Patient Transfer) OR (MH Patient Transfer))) | CINAHL Complete | 4 |
| (((Surveys and Questionnaires): ti,ab,kw AND (Risk Assessment):ti,ab,kw) AND ((Transportation of Patients):ti,ab,kw OR (Patient Transfer):ti,ab,kw)) | Cochrane | 11 |
| (((Surveys and Questionnaires) AND (Risk Assessment)) AND ((Patient Transfer) OR (Transportation of Patients))) | Scielo | 0 |
| LILACS | 2 | |
| OpenGrey | 6 | |
| DART-Europe | 0 | |
| RCAAP | 17 |
Articles were selected according to the framework proposed by the JBI (Peters et al., 2021): population (critically ill patients), concept (assessment instruments), and context (secondary transport). Regarding aim and study design, the review included all qualitative and quantitative primary research articles, literature reviews, and grey literature articles. The review included studies written in Portuguese, Spanish, or English, with no limitations on the time of publication. Conference presentations, opinion articles, and abstracts were excluded from the analysis. The search was conducted between 14 March and 31 May 2022.
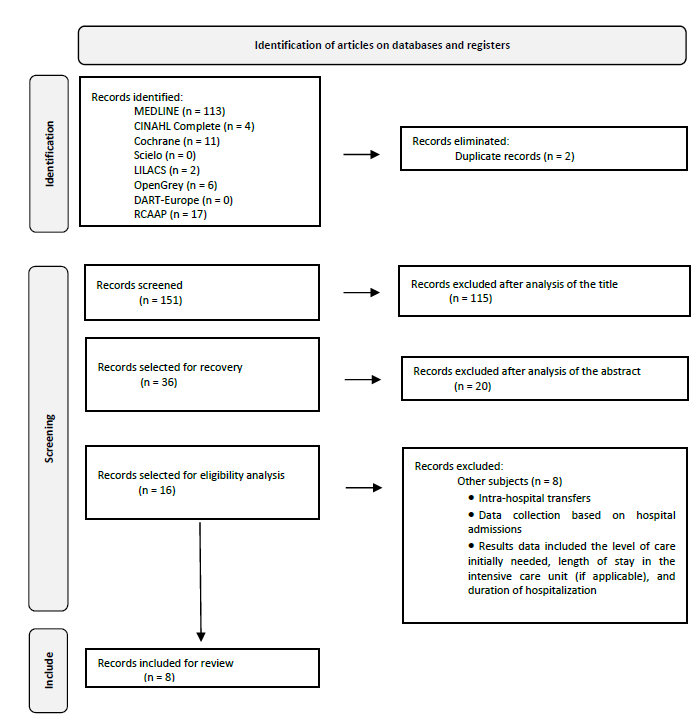
All the studies identified were organized using the EndNote® software. Duplicate articles were eliminated at this stage. Two independent reviewers (MR and LM) analyzed the titles and abstracts of the articles identified to assess their relevance. Two reviewers independently examined the full texts of the articles to establish whether they met the inclusion criteria. Disagreements were resolved by consensus, and recourse to a third reviewer was not necessary. All studies meeting the pre-established selection criteria were recovered in full text.
The PRISMA-ScR flow diagram shown in Figure 1 summarises the article selection process. No reliable, validated patient assessment instrument for secondary transport was identified. The diagram adapted for this scoping review presents the results of the 3 main stages: identification, screening, and inclusion. Of a total of 153 eligible studies, 8 articles focusing on patient assessment instruments for secondary transport were included in the review.
2. Results
According to the structure developed for this scoping review, the data extracted from the articles included for review are presented in line with the recommendations of the JBI manual (Peters et al., 2021), the research question, and the study objectives. The level of evidence was characterized according to the system proposed by the JBI (Peters et al., 2021); data extracted from the articles were organized by author(s), year, country, objective/purpose, sample, study design, results, and level of evidence (Table 2).
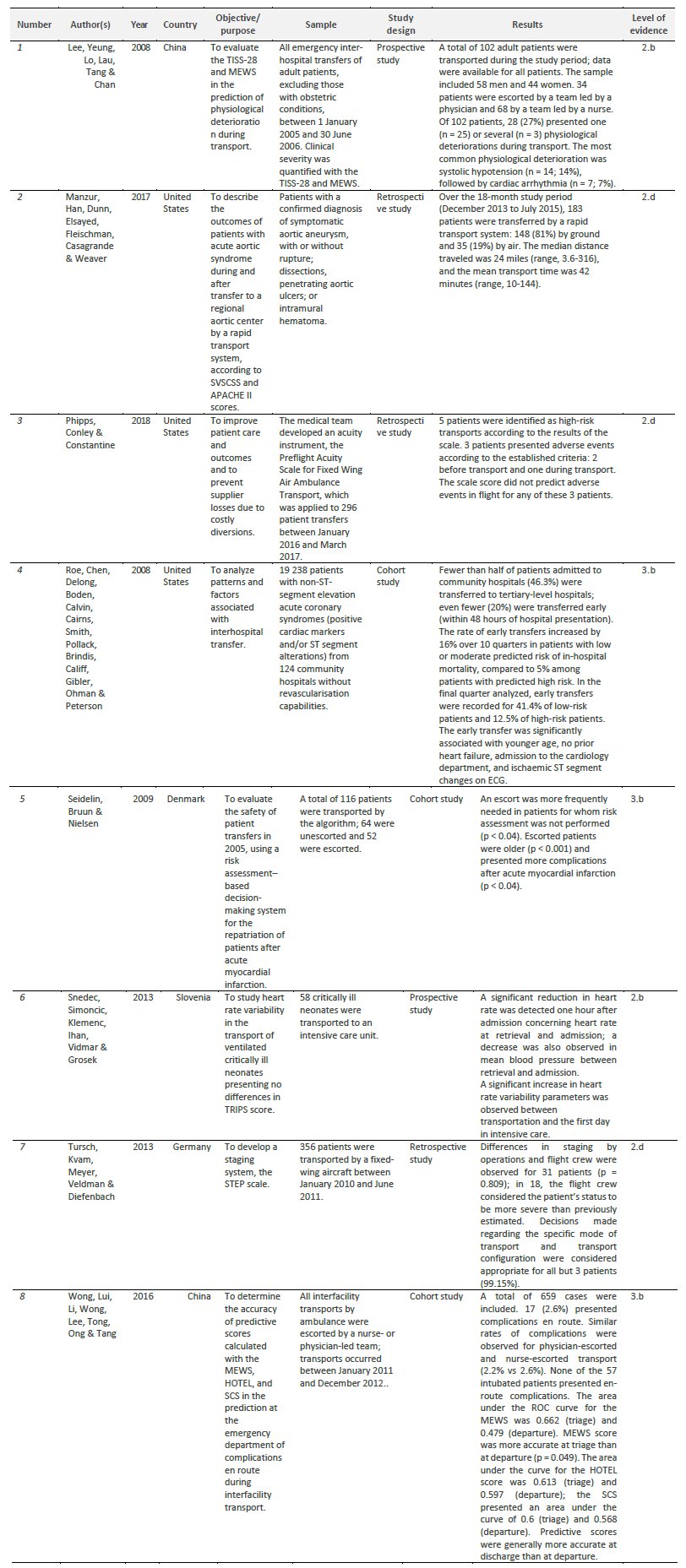
APACHE II: Acute Physiology and Chronic Health Evaluation II; ECG: electrocardiography; HOTEL: Hypotension, Low Oxygen Saturation, Low Temperature, Abnormal ECG, Loss of Independence score; MEWS: Modified Early Warning Score; SCS: Simple Clinical Score; ROC: receiver operating characteristic; STEP: Stratification of Aur Medical Transport by Expression of Symptoms in Patients; SVSCSS: Society for Vascular Surgery Comorbidity Severity Score; TISS- 28: Simplified Therapeutic Intervention Scoring System; TRIPS: Transport Risk Index of Physiologic Stability score.
A narrative analysis of the content was developed to provide a qualitative synthesis of the studies reviewed (Bardin, 2016). A thematic review of the content of the articles was conducted, identifying themes aligned with the study objective and the implications for future research, and evaluating policies and their implications.
The studies included for review were conducted in the United States (n = 3), China (n = 2), Denmark (n = 1), Germany (n = 1), and Slovenia (n = 1). The articles reviewed presented different study designs: 2 prospective studies, 3 retrospective studies, and 3 cohort studies.
Analysis of the results reported identified 9 assessment instruments: Simplified Therapeutic Intervention Scoring System (TISS-28); Modified Early Warning Score (MEWS); Society for Vascular Surgery Comorbidity Severity Score (SVSCSS); Acute Physiology and Chronic Health Evaluation II (APACHE II) score; Preflight Acuity Scale for Fixed Wing Air Ambulance Transport; Transport Risk Index of Physiologic Stability (TRIPS) score; Stratification of Air Medical Transport by Expression of Symptoms in Patients (STEP); Hypotension, Low Oxygen Saturation, Low Temperature, Abnormal ECG, Loss of Independence (HOTEL) score; Simple Clinical Score (SCS).
Simplified Therapeutic Intervention Scoring System
The simplified TISS-28 was used to predict deterioration during interfacility transport. Clinical severity was quantified according to the TISS-28 score immediately before transportation. The transport team was selected according to the pre-transport TISS-28 score. The TISS-28 was selected as an assessment instrument because it exclusively represents the intensity of the intervention and serves only as an indirect measure of clinical severity. The instrument is simple to apply and can be used uniformly for all patients (Lee et al., 2008).
Modified Early Warning Score
The MEWS was used to predict complications during interfacility transport (Wong et al., 2016; Lee et al., 2008). The MEWS is a physiological scoring system that is appropriate for bedside application and requires no complex equipment (Lee et al., 2008). It can be used to assess various types of patients, as it enables quantification of patient risk, defined according to 5 variables: systolic blood pressure, heart rate, respiratory rate, temperature, and AVPU score (alert, reacting to verbal stimulus, reacting to pain, and unresponsive) (Wong et al., 2016; Lee et al., 2008).
Society for Vascular Surgery Comorbidity Severity Score
The SVSCSS was used to determine the severity of comorbidities. The components of the score include heart disease, lung disease, kidney dysfunction, hypertension, and age (Manzur et al., 2017).
Acute Physiology and Chronic Health Evaluation II score
The APACHE II score was used to evaluate physiological instability at the time of admission (Manzur et al., 2017).
Preflight Acuity Scale for Fixed Wing Air Ambulance Transport
This scale scores patients according to the conditions identified during preflight medical evaluation, initial patient assessment, demographic data, and associated factors. The system provides information for flight crews, enabling improvements in terms of staffing, modifications to existing protocols, and flight planning, to improve care provision and outcomes and prevent complications (Phipps et al., 2018).
Transport Risk Index of Physiologic Stability score
The TRIPS score was calculated at admission, according to 4 empirically weighted items: temperature, respiratory status, systolic blood pressure, and response to noxious stimuli (Snedec et al., 2013).
Stratification of Air Medical Transport by Expression of Symptoms in Patients
The STEP is a staging system for different situations between operations staging and staging by the flight crew, and for assessment of the correlation between operations and actual transport acuity (Tursch et al., 2013).
Hypotension, Low Oxygen Saturation, Low Temperature, Abnormal ECG, Loss of Independence score
A study was conducted to determine the precision of the HOTEL score in predicting complications during interfacility transport. The variables scored are: systolic blood pressure < 100 mmHg, peripheral oxygen saturation < 90%, temperature < 35 °C, presence of electrocardiographic alterations, and level of dependence (Wong et al., 2016).
Simple Clinical Score
Researchers aimed to establish the accuracy of the SCS for predicting complications during interfacility transport. The variables collected are age, gender, systolic blood pressure, heart rate, temperature, respiratory rate, peripheral oxygen saturation, respiratory effort, electrocardiographic alterations, diabetes, coma, impaired level of consciousness, intoxication or overdose, new-onset stroke, and level of dependence (Wong et al., 2016).
Patients with non-ST segment elevation acute coronary syndrome
The variables found to be significantly associated with secondary transport were age, no prior heart failure, admission to the cardiology department, and ischaemic ST-segment electrocardiographic alterations (Roe et al., 2008).
Aeromedical transport after acute myocardial infarction
The variables identified were age and complications following acute myocardial infarction (Seidelin et al., 2009).
3. Discussion
The lack of scientific evidence on patient assessment instruments for secondary transport results from the lack of studies; transport decision-making and planning by healthcare professionals are hindered by the lack of validated, reliable patient assessment instruments that may be applied in all situations.
The studies reviewed were published in China (Wong et al., 2016; Lee et al., 2008), the United States (Phipps et al., 2018; Manzur et al., 2017; Roe et al., 2008), Denmark (Seidelin et al., 2009), Slovenia (Snedec et al., 2013), and Germany (Tursch et al., 2013). Except for Denmark and Slovenia, these countries have mixed public-private healthcare systems in which health insurance is needed to access healthcare. Health insurance does not cover access to transport services, which constitutes a limitation for comparison of the results between countries.
The studies included in this scoping review present a moderate level of evidence; further research is needed on the subject of patient assessment instruments for secondary transport due to the small number of studies, the countries in which the extant research was conducted, and the limited evidence currently available.
Nine instruments were identified in the review: TISS-28 (Lee et al., 2008); MEWS (Wong et al., 2016; Lee et al., 2008); SVSCSS (Manzur et al., 2017); APACHE II score (Manzur et al., 2017); Preflight Acuity Scale for Fixed Wing Air Ambulance Transport (Phipps et al., 2018); TRIPS score (Snedec et al., 2013); STEP (Tursch et al., 2013); HOTEL score (Wong et al., 2016); and SCS (Wong et al., 2016).
The studies included in the scoping review show that patient assessment instruments for secondary transport are not uniformly used in everyday practice. Thus, there is a need for a greater understanding of the available instruments, taking into account every aspect of the transfer process (Ramgopal, 2020).
The TISS-28 is not useful for pre-transport risk stratification as it does not inform as to whether the patient was inadequately overtreated. Thus, the intensity of care is affected by diagnosis and by the institutional setting, influencing the patient transport process. The TISS-28 showed poor performance in predicting physiological deterioration before secondary transport (Lee et al., 2008).
The MEWS was able to identify at-risk patients but is not an ideal instrument because it exclusively assesses variable physiological factors and simply collects the values recorded during the assessment. The fact that these variables are purely physiological would imply that the incidence of complications en route is influenced by physiological stability before secondary transport, alongside such other factors as case mix, anticipated deterioration, and the need for advanced-level care and specialized transport teams (Wong et al., 2016; Lee et al., 2008). Given the difficulty of predicting which patients will deteriorate and identifying high-risk patients, the MEWS was developed purely to predict critical events (Veldhuis et al., 2021).
The SVSCSS was able to predict the increase in system-related mortality and may be valuable for evaluating the appropriateness of patient transfer. This may assist healthcare professionals in determining the adequacy and the success of the transfer, reducing the rate of unnecessary secondary transports and subsequent futile therapy (Manzur et al., 2017).
The APACHE II score was a determinant of system-related mortality and is used at the time of patient admission (Manzur et al., 2017).
The Preflight Acuity Scale for Fixed Wing Air Ambulance Transport was not predictive of adverse events en route and is applied for the patients who would transfer by air ambulance. Assessment information was provided to flight crews, enabling improvements in terms of staffing, modification to existing protocols, and flight planning. Despite the failure to predict adverse events, it did offer information on relevant factors that may have prevented adverse events during secondary transport (Phipps et al., 2018).
The TRIPS score was found to be useful for evaluating the outcomes of secondary transport and is used at the time of patient admission (Snedec et al., 2013). No difference in transport success rates was observed between transfers with and without a physician escorting the patient (Abdelmawla et al., 2021). TRIPS score is associated with mortality and neurodevelopmental impairment, reflecting the degree of physiological instability, which may complement risk assessment (Grass et al., 2020).
The STEP is useful for evaluating the severity of illness/injury during the planning of long-distance secondary transport, informing decision-making regarding the mode and configuration of transport. Thus, it constitutes a pragmatic, effective tool for quality control and improving outcomes (Tursch et al., 2013).
The HOTEL score and SCS enable the prediction of mortality after patient assessment at admission, presenting acceptable precision and excellent discrimination (Wong et al., 2016).
Most patients with non-ST-segment elevation acute coronary syndromes admitted to centers without resources for revascularisation are not rapidly transferred to a different hospital (Roe et al., 2008).
Patients may be transferred in an aeromedical transport without a specialized team after acute myocardial infarction if the preflight risk stratification assessment indicates low risk (Seidelin et al., 2009).
Secondary transport has become increasingly necessary in recent years due to the differentiation of care and specialized techniques; however, transfers also involve several multiple risks (Eiding et al., 2019; Mueller et al., 2019; Kiss et al., 2017; Lee et al., 2008; Markakis et al., 2006). Anticipating potential clinical deterioration is essential to the safety of both the patient and the transfer team; therefore, it is crucial to conduct a risk assessment before transport (Dabija et al., 2021; Ramgopal, 2020; Eiding et al., 2019; Tursch et al., 2013; Lee et al., 2008). Secondary transport must be performed when the benefits to the patient outweigh the potential risks associated with the occurrence of complications during transfer. Thorough planning of the transfer is necessary to minimize any potential morbidity during transfer (Dabija et al., 2021; Eiding et al., 2019; Lee et al., 2008). Transport quality and outcomes are largely determined by decision-making and planning, taking into account the specialized human and technical resources available (Conde et al., 2021; Eiding et al., 2019; Phipps et al., 2018; Snedec et al., 2013; Tursch et al., 2013; Lee et al., 2008). No widely implemented standards or recommendations are available for the application or regulation of secondary transport, as no reliable, validated assessment can predict physiological deterioration during transfer. The assessments conducted before transport are currently subjective, resulting in variability in the composition of the team escorting the patient; more objective criteria are needed for the allocation of human and technical resources and the mode of transport (Ramgopal, 2020; Lee et al., 2008; Markakis et al., 2006). The assessment systems currently available may be generic or specific, and aim to quantify a variety of cases and predict outcomes (Lee et al., 2008).
Conclusion
In conclusion, no effective, validated instruments currently exist that guarantee precise patient assessment before secondary transfer, concerning the prediction of complications en route; such an instrument would enable the selection of the most appropriate mode of transport, transport team, and equipment.
Secondary patient transport has evolved in parallel to the development of the healthcare system and has assumed an increasingly important role in patient transfers as a whole. However, patient transfers involve numerous risks, instability, and potential complications. The decision to perform the transfer must be carefully considered, taking into account the best available evidence, the risk/benefit balance, and proper risk assessment.
These instruments are useful for patient assessment as they present informative variables that should be taken into consideration to prevent adverse events during transport. However, it is not yet possible to develop standardized recommendations and good practices based on a reliable, validated tool, as the existing instruments continue to present gaps that hinder proper risk assessment and stratification of all types of patients and conditions.
Nurses play a central role in the planning and execution of efficient transfers. In the context of secondary transport, nurses must seek to guarantee the continuation and quality of care provision.
It is important to evaluate the appropriateness of secondary transfer, considering the potential risks and benefits of transfer, based on associated factors related both to the patient and to the transfer itself.
The limitations of this study are related to the lack of evidence on normalized, validated, and reliable patient assessment instruments for secondary transport.
The majority of the studies included in the review were not conducted in Europe. As the studies reviewed present a moderate level of evidence, there is a need to conduct experimental studies analyzing the impact of patient assessment instruments on secondary transport, to develop a better instrument that may enable the standardization of care, based on recommendations leading to better practice.
Identifying issues related to patient assessment instruments for secondary transport enables a better understanding of the state of the art in this area and thus the development of projects attending to the actual needs of healthcare professionals in patient assessment before secondary transport.
Acknowledgements
The authors thank Jack Leyden for his help with the English translation of the manuscript.
Author contributions
Conceptualization, M.J.R., L.M., A.S.P. and T.A.; data curation, M.J.R. and L.M.; formal analysis, M.J.R. and L.M.; funding acquisition, M.J.R., L.M., A.S.P. and T.A.; investigation, M.J.R. and L.M.; methodology, M.J.R. and L.M.; project administration, M.J.R; resources, M.J.R., L.M., A.S.P and T.A.; software, M.J.R. and L.M.; supervision, M.J.R.; validation, M.J.R., L.M., A.S.P and T.A.; visualization, M.J.R., L.M., A.S.P. and T.A.; writing - original draft, M.J.R. and L.M.; writing - review & editing, M.J.R., L.M., A.S.P. and T.A.;

