










Services on Demand
Journal
Article
 Portuguese (pdf)
Portuguese (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkMedicina Interna
Print version ISSN 0872-671X
Medicina Interna vol.27 no.1 Lisboa Mar. 2020
https://doi.org/10.24950/O/185/19/1/2020
ARTIGOS ORIGINAIS / ORIGINAL ARTICLES
Etiologia, Tratamento e Prognóstico da Pericardite Aguda
Etiology, Treatment and Prognosis of Acute Pericarditis
João Fernandes Serodio1  https://orcid.org/0000-0002-9567-335X
https://orcid.org/0000-0002-9567-335X
Miguel Trindade1 https://orcid.org/0000-0001-6910-3807
Miguel Achega2 https://orcid.org/0000-0002-5500-0097
Daniel Faria3 https://orcid.org/0000-0003-3837-6786
Joana Maurício4 https://orcid.org/0000-0002-2049-8649
Frederico Batista1,5 https://orcid.org/0000-0002-6324-9300
Catarina Favas1,5 https://orcid.org/0000-0002-7472-7216
José Delgado Alves1,5,6 https://orcid.org/0000-0002-5216-4125
1Serviço de Medicina IV, Hospital Professor Doutor Fernando Fonseca, Amadora, Portugal
2Serviço de Medicina II, Hospital Professor Doutor Fernando Fonseca, Amadora, Portugal
3Serviço de Cardiologia, Hospital Professor Doutor Fernando Fonseca, Amadora, Portugal
4Serviço de Medicina III, Hospital Professor Doutor Fernando Fonseca, Amadora, Portugal
5Unidade de Doenças Imunomediadas Sistémicas, Hospital Professor Doutor Fernando Fonseca, Amadoera, Portugal
6Centro para o Estudo de Doenças Crónicas (CEDOC), Nova Medical School Lisbon, Lisboa, Portugal
Resumo:
Introdução: A pericardite aguda é uma síndrome frequente caracterizada pela inflamação do pericárdio e usualmente atribuído a etiologia viral/idiopática. Apesar dos avanços no tratamento, existe informação limitada em relação a etiologia e prognóstico. O objetivo do nosso trabalho foi identificar a prevalência de pericardite aguda com etiologia especifica e avaliar marcadores clínicos de prognóstico.
Material e Métodos: Estudo retrospetivo de doentes hospitalizados por pericardite aguda entre 2012-2016. A população foi caracterizada quanto a etiologia, apresentação clínica, tratamento e prognóstico. Para avaliação de prognóstico foram avaliadas recorrência de pericardite, pericardite constritiva e mortalidade global um ano após alta hospitalar.
Resultados: Foram incluídos 94 doentes com idade mediana 46 anos (IIQ 32-61), 65% eram do sexo masculino. A etiologia idiopática foi responsável por 68% dos casos. Etiologia especifica foi identificada em 32% dos doentes, sendo mais frequente doença autoimune (12%) e neoplasia (5%). A pericardite idiopática foi mais associada a miopericardite (p = 0,049), enquanto a etiologia específica se associou a derrame pericárdico (p = 0,001) e a tamponamento pericárdico (p = 0,027). A recorrência de pericardite ocorreu em 13% dos doentes. O tratamento com corticosteroides em doentes com etiologia definida não se associou com aumento de recorrência (p = 0,220). A mortalidade global a um ano foi de 9%. A etiologia definida de pericardite aguda revelou-se o único preditor independente de mortalidade na análise multivariada (OR 40,3; 95% CI 1,9 – 137,2; p = 0,016).
Conclusão: Cerca de um terço dos doentes hospitalizados por pericardite aguda têm uma causa específica identificável de pericardite e estes doentes apresentam risco aumentado de mortalidade.
Palavras-chave: Doença Aguda; Pericardite/diagnóstico; Pericardite/etiologia; Pericardite/tratamento; Prognóstico.
Abstract:
Introduction: Acute pericarditis is a common inflammatory condition of the pericardium usually assumed to be viral or idiopathic. Despite recent treatment improvements, information is scarce regarding etiology and prognosis. Our aim was to determine the incidence of pericarditis with a known etiology and assess clinical prognostic predictors.
Material and Methods: A clinical retrospective analysis of hospitalized patients with acute pericarditis was conducted from 2012 to 2016. Population was characterized according to etiology, clinical presentation, treatment and prognosis. Outcomes of interest, evaluated at one year after hospital discharge, were pericarditis recurrence, hospitalization, constriction and overall mortality.
Results: A total of 94 patients were enrolled, median age 46 years (inter-quartile range 32-61), 65% were male. Idiopathic etiology was responsible for 68% of cases. A specific etiology was found in the remaining 32% of patients, being the most frequent autoimmune disease (12%) and malignancy (5%). Idiopathic pericarditis was associated with myopericarditis (p = 0.049) and a known etiology with pericardial effusion (p = 0.001) and cardiac tamponade (p = 0.027). Recurrence of pericarditis was found in 13% of patients. Corticosteroid treatment in patients with an identified etiology was not associated with an increase in recurrence (p = 0.220). Overall 1-year mortality was 9%. A defined etiology was the only independent predictor of mortality at multivariate analysis (OR 40.3; 95% CI 1.9 – 137.2; p = 0.016).
Conclusion: Up to one third of hospitalized patients with acute pericarditis have an identified cause of pericarditis and these patients are at increased risk of mortality.
Keywords: Acute Disease; Pericarditis/diagnosis; Pericarditis/etiology; Pericarditis/therapy; Prognosis.
Introduction
Acute pericarditis is the most common disease of the pericardium. Its incidence is estimated in 27 cases per 100 000 population per year in an urban European population1 and it is responsible for 0.1% of all hospital admissions.2 It affects mainly male patients aged between 16 and 65 years old.3 Although the clinical diagnosis of acute pericarditis may be relatively simple, the etiologic diagnosis is broad and varies according to multiple factors.3 Whereas in Sub-Saharan African countries tuberculosis is the most important cause of acute pericarditis, in developed countries most cases have been classified as presumably viral or idiopathic.4-8 However, in some cases, pericarditis may reflect an underlying systemic disease.4,8
The treatment of acute pericarditis is based on the use of non-steroid anti-inflammatory drugs (NSAIDs), colchicine and the treatment of the underlying cause.9-11 The rate of recurrence of pericarditis ranges from 15% - 40%.9 The overall prognosis is generally good, however few data concerning mortality and predictors of recurrence is available.3,8 The aim of our study was to assess the incidence of acute pericarditis with a known cause and to determine clinical parameters related to prognosis.
Material and Methods
A clinical retrospective observational study of patients identified between 2012 and 2016 in our Hospital was performed. All patients aged 18 years or older hospitalized with a clinical diagnosis of acute pericarditis according to available criteria were included.3,4,7 Accepted criteria were at least two of the following: typical chest pain, pericardial friction rubs, recent widespread ST segment elevation or PR depressions and new pericardial effusion. Patients not fulfilling diagnostic criteria for acute pericarditis and those with missing data concerning the etiology were excluded.
Data was analysed regarding demography, clinical presentation, etiology, treatment and prognosis. Clinical variables considered were the presence of myopericarditis, pericardial effusion and pericardial tamponade. A diagnosis of myopericarditis was considered whenever a patient with the clinical diagnosis of acute pericarditis had evidence of elevated troponin I.12 Presence of pericardial effusion was assessed by transthoracic echocardiography. Cardiac tamponade was clinically established on patients with clinical signs of elevated jugular pressure or pulsus paradoxus, hemodynamic instability (tachycardia or arterial hypotension) and echocardiographic evidence of large pericardial effusion (pericardial effusion of >20 mm with partial or total collapse of right heart chambers), without other cardiac diseases.12,13
Information considering etiology was derived from patients’ clinical records. There was no specific diagnostic protocol applied to all patients, so workup was individualized. Diagnostic strategy for viral etiology was not generally used as the list of probable virus is broad, serologic testing is not adequate and molecular diagnosis is expensive and time-consuming.12 For the purpose of this study, all patients with viral etiology or patients with no confirmed etiology, presumably viral, were classified as having idiopathic pericarditis. Blood tests included C-reactive protein (CRP), erythrocyte-sedimentation rate (ESR) and high-sensitive troponin I. Data regarding treatment included therapy performed during hospitalization and after discharge. Prognosis was evaluated at one year after hospital discharge; we looked at pericarditis recurrence, hospitalization for recurrence, constriction and overall mortality.
Analysis was performed using STATA MP version 14 (StataCorp LLC®, Texas, USA). Categorical data was presented as counts and percentages and was analysed with chi-square test or the Fisher’s exact test, when the expected numbers are small (<5). Normality was tested with Kolmogorov-Smirnov test, showing that all continuous variables were skewed. The skewed distributions were described with medians and interquartile ranges (IQR) and were compared with the use of the Mann-Whitney. These tests were performed to compare clinical and laboratory features between patients with idiopathic pericarditis and those with defined etiology. In order to assess predictors of mortality, clinical, laboratory and treatment variables were selected for a logistic regression analysis, assessed by the estimated odds ratio (OR) with 95% confidence interval (CI). Firth logistic regression was applied whenever appropriate. Variables yielding p values of less than or equal to 0.10 in the bivariate analyses were entered into a multiple logistic regression model in which 1-year overall mortality was the outcome of interest. Two episodes of hospitalization for acute pericarditis from the same patient were treated as independent cases. The two-sided alpha level was set at 0.05.
Results
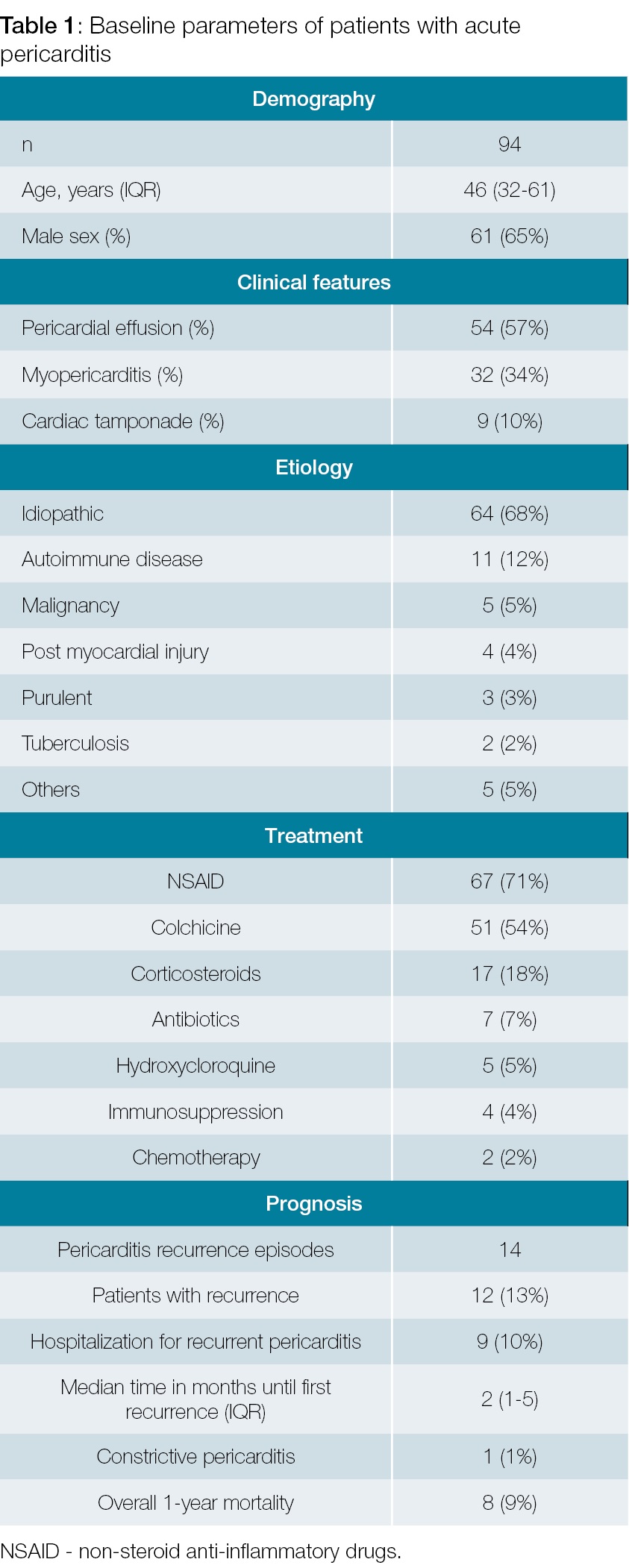
The population studied consisted of 94 patients with a median age of 46 years (32-61), 65% were male. Of all patients included, 57% had pericardial effusion, 34% had myopericarditis and 10% had cardiac tamponade (Table 1). Only one patient with myopericarditis had left ventricular systolic dysfunction on echocardiogram that completely resolved during follow-up. In our cohort, 68% of cases were idiopathic and 32% had an identified etiology. From these, the most frequent were autoimmune disease (12%), malignancy (5%) and post-myocardial injury syndrome (4%). Systemic lupus erythematosus was the most frequent autoimmune disease (6/11 patients), whereas lung cancer was the most frequent neoplasm (3/5 patients). In patients with autoimmune disease and malignancy, pericarditis was the first manifestation of disease in 18% and 80%, respectively. Six cases of pericarditis were attributed to bacterial infections: 2 patients had tuberculosis, 3 had purulent pericarditis (Staphylococcus aureus, Serratia marcescens and Salmonella enterica) and 1 had syphilis. All patients were HIV negative. Other uncommon causes like drug-induced pericarditis, uremic pericarditis and pulmonary embolism were found in 5% of patients.
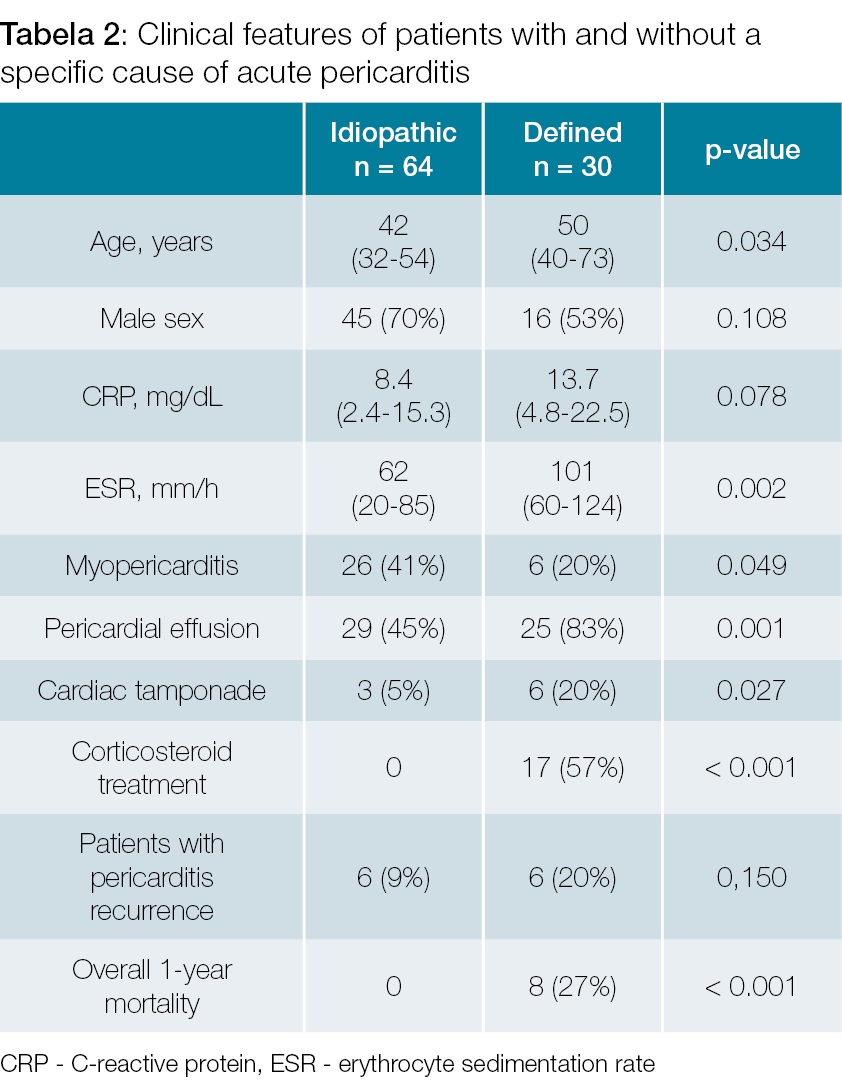
Patients with a known etiology (Table 2) were older (p = 0.034), had more frequently pericardial effusion (p = 0.001), cardiac tamponade (p = 0.027) and presented with increased ESR values at admission (p = 0.002). Myopericarditis was more frequent among patients with idiopathic pericarditis (26 out of 32 patients, p = 0.049). Among 9 patients with cardiac tamponade, only 3 had idiopathic pericarditis. The remaining 6 patients had recognized etiology, notably post-myocardial injury (2), purulent pericarditis, tuberculosis, neoplasia, pulmonary embolism and drug-induced pericarditis.
In the population studied, 71% of patients were treated with non-steroid anti-inflammatory drugs and 54% with colchicine. Corticosteroids were used in 18% patients with refractory symptoms or systemic disease. There was no patient with idiopathic pericarditis receiving corticosteroid treatment (Table 2). Additional treatment was implemented for specific etiologies, such as antibiotics for bacterial pericarditis (7%), hydroxycloroquine in the case of systemic lupus erythematosus (5%) and immunosuppression or chemotherapy (respectively 4% and 2%). Combination of more than one pharmacologic treatment was frequent (52% of cases), with non-steroid anti-inflammatory drugs and colchicine being the most frequent combination (43% of cases). Nine (10%) patients required pericardiocentesis for the management of pericardial effusion.
At 12-month follow-up after discharge, 13% of patients had at least one episode of recurrence of pericarditis, and it motivated hospitalization in 10% of all patients. The median time until the first pericarditis recurrence was 2 months (1-5). One patient developed constrictive pericarditis and underwent pericardial surgery. Neither specific etiology nor any of the clinical parameters analysed were associated with a higher rate of recurrence. Of note, treatment with corticosteroids was not associated with pericarditis recurrence (p = 0.220).
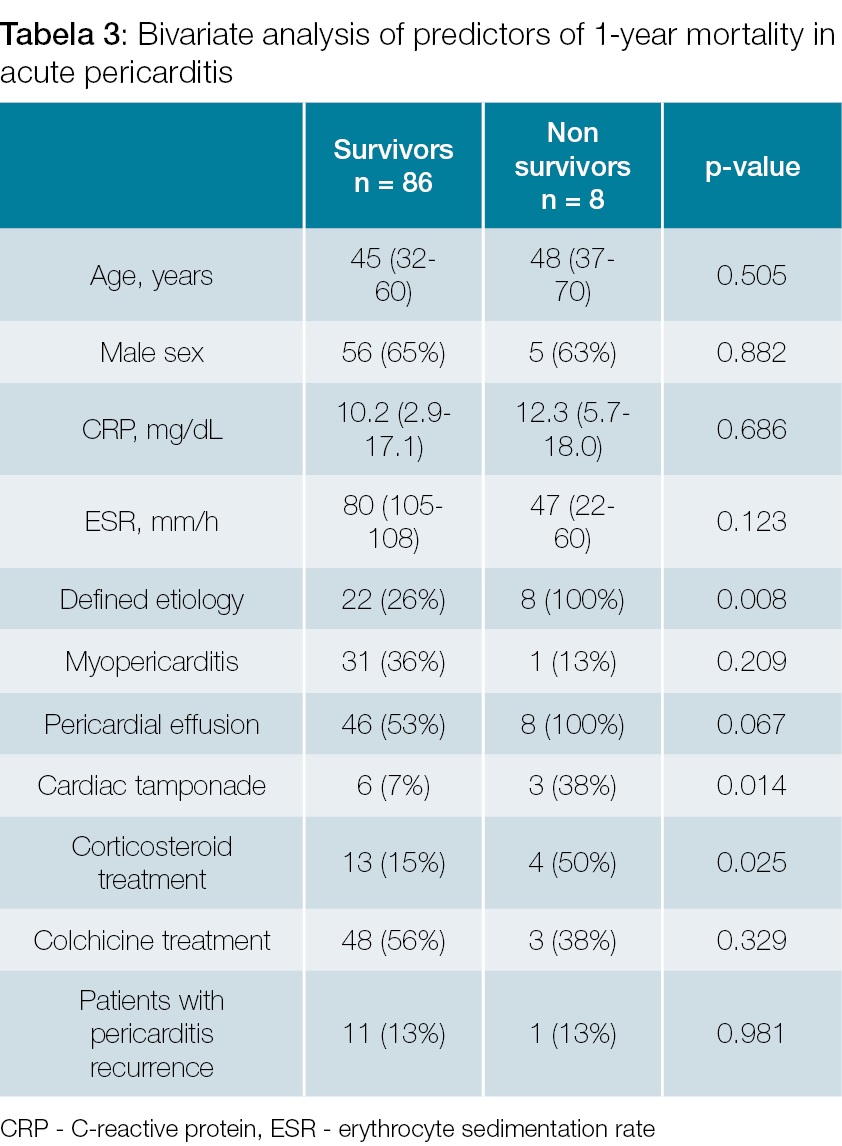
The one-year overall mortality for acute pericarditis was 9% (8 patients: 5 with malignancy, 2 with purulent pericarditis, one with post-myocardial injury). Predictors of pericarditis 1-year mortality at bivariate analysis are presented in Table 3. Multivariate model revealed that a defined etiology of pericarditis was the only independent predictor of mortality (OR 40.3; 95% CI 1.9 – 137.2; p = 0.016). Mortality was related with the underlying disease and not with pericarditis itself in a significant proportion of patients (5 out 8 patients). The etiology of pericarditis among non-survivors was neoplasia in 5 patients, purulent pericarditis in 2 and post-myocardial injury in one. Cardiac tamponade was managed at in-hospital care and was not a direct cause of death in our cohort.
Discussion
In accordance with the literature,4-8 idiopathic pericarditis was the most prevalent etiology found in our study. About one-third of patients in our cohort had a specific systemic etiology, which is slightly higher than previous reports.7 Like in our study, most studies state autoimmune disease and malignancy as the two most prevalent causes for acute pericarditis.5-7 However, autoimmune disease was the etiology of pericarditis in a bigger proportion of patients (12%), than the average 3% - 7% reported in previous cohorts.7-12 Importantly, we found that acute pericarditis is the first manifestation of the disease in a considerable proportion of these patients. Post-myocardial injury syndrome was present in 4% of patients, somewhat lower than the 20% reported on the population of colchicine randomized trials.11 Nevertheless, the recruitment on these studies was based in cardiology and cardiac surgery departments, and some etiologies like tuberculosis were excluded from the trials, which may explain these differences.11 The frequency of tuberculosis remains as low as 2%, in accordance with the 1-3% reported in other European studies. This is in contrast with the prevalence of pericardial tuberculosis in African contrives, that represents about 70% of all cases.7,8 Notably, purulent pericarditis was found in 3% of our population, somewhat higher than the < 1% reported.7 Therefore, we believe it is important to look for the possibility of increasing incidence of purulent pericarditis during the following years considering the increasing prevalence of immunocompromised patients, mainly due to cancer and inflammatory diseases treatments. Although most cases are idiopathic, our data emphasize the diversity of the etiology of acute pericarditis, with some uncommon cases reflecting a systemic underlying condition like uremic pericarditis or xanthogranulomatous pyelonephritis.14 Therefore, an integrated approach should always be attempted whenever a defined etiology is suspected.
We also found that patients with idiopathic pericarditis differed in some important clinical features from pericarditis with specific cause. While myopericarditis was more frequent in idiopathic pericarditis, a specific cause was associated with older age, elevated ESR, pericardial effusion and cardiac tamponade. These results were similar to a prospective cohort from Imazio et al.13 Interestingly, tamponade was found almost only among patients with specific etiology (6 out of 9 patients). However, despite autoimmune disease being the most common specific etiology of pericarditis, no single patient with autoimmune disease developed cardiac tamponade.
The frequency of recurrence (13%) was low, when compared with the literature (15% - 40%9). Previous studies on recurrence of pericarditis were performed before clinical trials on colchicine, which is thought to halve the incidence of recurrences.10,11 Treatment with colchicine in a significant proportion of patients may explain the lower frequency in our population. No specific etiology was associated with the recurrence rate. Likewise, no clinical feature (pericardial effusion, myopericarditis, inflammatory markers) was found to be associated with an increased recurrence. So, mechanisms of recurrence may not be etiology associated and some data suggest that immune-mediated processes are involved in recurrent pericarditis, different from the mechanisms present in acute pericarditis.15 In our cohort, patients with a defined etiology who were treated with corticosteroids were not found to have an increase in recurrences. This is in contrast with some previous reports9,14 in which they were used in patients with idiopathic pericarditis at high doses. In our study, only patients with an identified cause were treated with corticosteroids (Table 2) at doses of 0.5-1.0 mg/kg. Therefore, our data suggest that at least in patients with a defined etiology, corticosteroid treatment is not associated with an increase in recurrence. Constrictive pericarditis occurred in very low numbers (one case of idiopathic pericarditis), not allowing making conclusions regarding this entity. This may reflect the low frequency of tuberculosis pericarditis in our cohort, as constriction is a recognizable complication among these patients.8
Besides the overall good prognosis, a known etiology of acute pericarditis was independently associated with an increased risk of mortality. The fact that patients with a specific etiology have increased mortality strengthens the need to better identify these patients. Increase in mortality in our study was mostly a result of malignancy and purulent pericarditis. Patients with cardiac tamponade also had significant mortality (3 out of 9 patients). However, tamponade did not reveal as a significant predictor of mortality on multivariate analysis. Most probably, this occurred because most cases of tamponade occurred in patients with specific causes (post-myocardial injury or cancer). Moreover, tamponade was not a direct cause of death among these patients, most importantly underlying disease explained worse prognosis.
Mortality in patients with pericarditis was rarely addressed. Previous studies defined clinical predictors of pericarditis complications (tamponade, recurrence, constriction),13,16 however mortality was not evaluated. Zayas et al6 also found an association between specific etiology and unfavourable outcome. In a large Danish cohort, pericarditis patients were found to be at increased risk for cancer and patients with cancer and pericarditis had higher mortality.17 On the other hand, purulent pericarditis has also been associated with high mortality rates.18
Several limitations of our study should be considered. Firstly, it is a retrospective study on hospitalized patients. In fact, there is few data concerning the etiology of acute pericarditis in ambulatory patients. Secondly, it reflects a single centre experience. Furthermore, there was no etiologic diagnostic protocol. However, a diagnostic protocol does not seem to offer a significant advantage over a physician decision diagnosis.7
Furthermore, the small sample used in this study is another limitation to consider, particularly the small proportion of patients with defined etiology (30 patients). The outcome of interest on the prognostic analysis, 1-year after discharge overall mortality, was a relatively rare event (9% of patients). This may explain the wide and imprecise CI yielded by the multivariate logistic regression model for defined etiology as a predictor of mortality. Although this gives quite imprecise information regarding the risk of mortality for these patients, the results were quite significant and there were no deaths among patients with idiopathic pericarditis. That said, a defined etiology has prognostic implication and mortality might be related more with underling disease than the pericarditis itself. Nevertheless, pericarditis is the first presentation of the disease in a significant proportion of patients with underling cause. In order to overcome the above limitations, larger multicentric studies are needed. Besides, the inclusion of ambulatory patients would also be of interest.
In conclusion, most cases of acute pericarditis were idiopathic, but up to one third of patients hospitalized for acute pericarditis had a known etiology. Autoimmune disease and malignancy were the most frequent etiologies found. Patients with a known cause of pericarditis had higher rates of tamponade and an increased risk of mortality. Therefore, the identification of specific etiology for pericarditis has prognostic implications, which favours an integrated and individualized diagnostic approach to these patients.
REFERENCES
1. Imazio M, Cecchi E, Demichelis B, Chinaglia A, Ierna S, Demarie D, et al. Myopericarditis versus viral or idiopathic acute pericarditis. Heart. 2008, 94:498–501.
2. Sheith S, Wang DD, Kasapis C. Current and emerging strategies for the treatment of acute pericarditis: a systematic review. J Inflamm Res. 2010; 3:135 – 42. doi: 10.2147/JIR.S10268.
3. Imazio M. Contemporary management of acute pericarditis. Curr Opin Cardiol. 2012, 27:308-17. doi: 10.1097/HCO.0b013e3283524fbe. [ Links ]
4. Permanyer-Miralda G, Sagrista-Sauleda J, Soler-Soler J. Primary acute pericardial disease: a prospective series of 231 consecutive patients. Am J Cardiol. 1985; 56:623–30.
5. Ilan Y, Oren R, Ben-Chetrit E. Acute pericarditis: etiology, treatment and prognosis. A study of 115 patients. Jpn Heart J. 1991;32:315-21. [ Links ]
6. Zayas R, Anguita M, Torres F, Giménez D, Bergillos F, Ruiz M, et al. Incidence of specific etiology and role of methods for specific etiologic diagnosis of primary acute pericarditis. Am J Cardiol. 1995; 75:378–82.
7. Imazio M, Brucato A, DeRosa FG, Lestuzzi C, Bombana E, Scipione F, et al. Aetiological diagnosis in acute and recurrent pericarditis: when and how. J Cardiovasc Med. 2009, 10:217–30. doi: 10.2459/JCM.0b013e328322f9b1.
8. Mayosi BM. Contemporary trends in the epidemiology and management of cardiomyopathy and pericarditis in sub-Saharan Africa. Heart. 2007; 93:1176 – 83. doi: 10.1136/hrt.2007.127746.
9. Imazio M, Bobbio M, Cecchi E, Demarie D, Demichelis B, Pomari F, et al. Colchicine in addition to conventional therapy for acute pericarditis: results of theCOlchicine for acute PEricarditis (COPE) trial. Circulation. 2005; 112:2012–6.
10. Imazio M, Bobbio M, Cecchi E, Demarie D, Pomari F, Moratti M, et al. Colchicine as first choice therapy for recurrent pericarditis: results of the CORE (COlchicine for REcurrent pericarditis) trial. Arch Intern Med. 2005; 165:1987–91.
11. Imazio M, Brucato A, Cemin R, Ferrua S, Maggiolini S, Beqaraj F, et al. A randomized controlled trial of colchicine for acute pericarditis. N Engl J Med 2013;369:1522-8. doi: 10.1056/NEJMoa1208536 [ Links ]
12. Imazio M, Spodik D, Bracato A, Trinchero R, Adler Y. Controversial issues in the management of pericardial diseases. Circulation. 2010; 121:916-28. doi: 10.1161/CIRCULATIONAHA.108.844753. [ Links ]
13. Imazio M, Cecchi E, Demichelis B, Ierna S, Demarie D, Ghisio A, et al. Indicators of poor prognosis of acute pericarditis. Circulation. 2007; 115:2739-44. [ Links ]
14. Caetano J, Fernandes das Neves M, Oliveira S, Delgado Alves J. Xanthogranulomatous pyelonephritis presenting as palmoplantar keratoderma BMJ Case Rep. 2014; 2014 doi:10.1136/bcr-2014-208511.
15. Caforio AL, Brucato A, Doria A, Brambilla G, Angelini A, Ghirardello A, et al. Anti-heart and anti-intercalated disk autoantibodies: evidence for autoimmunity in idiopathic recurrent acute pericarditis. Heart. 2010;96:779-84. doi: 10.1136/hrt.2009.187138. [ Links ]
16. Imazio M, Demichelis B, Parrini I, Giuggia M, Cecchi E, Gaschino G, et al. Day-hospital treatment of acute pericarditis. J Am Coll Cardiol. 2004 ;43:1042–6.
17. Søgaard KK, Farkas DK , Ehrenstein V, Bhaskaran K, Bøtker HE, Sørensen HT. Pericarditis as a marker of occult cancer and a prognostic factor for cancer mortality. Circulation. 2017; 136:996–1006. doi: 10.1161/CIRCULATIONAHA.116.024041.
18. Pankuweit S, Ristic AD, Seferovic PM, Maisch B. Bacterial pericarditis: diagnosis and management. Am J Cardiovasc Drugs. 2005; 5:103-12. [ Links ]
Acknowledgements
We kindly thank Dr. António Alho from Serviço de Medicina I, Hospital Prof. Doutor Fernando Fonseca (not current affiliation) for his contribution with the review of medical records and data collection.
Responsabilidades Éticas
Conflitos de Interesse: Os autores declaram a inexistência de conflitos de interesse na realização do presente trabalho.
Fontes de Financiamento: Não existiram fontes externas de financiamento para a realização deste artigo.
Confidencialidade dos Dados: Os autores declaram ter seguido os protocolos da sua instituição acerca da publicação dos dados de doentes.
Proteção de Pessoas e Animais: Os autores declaram que os procedimentos seguidos estavam de acordo com os regulamentos estabelecidos pelos responsáveis da Comissão de Investigação Clínica e Ética e de acordo com a Declaração de Helsínquia da Associação Médica Mundial.
Proveniência e Revisão por Pares: Não comissionado; revisão externa por pares.
Ethical Disclosures
Conflicts of interest: The authors have no conflicts of interest to declare.
Financing Support: This work has not received any contribution, grant or scholarship
Confidentiality of Data: The authors declare that they have followed the protocols of their work center on the publication of data from patients.
Protection of Human and Animal Subjects: The authors declare that the procedures followed were in accordance with the regulations of the relevant clinical research ethics committee and with those of the Code of Ethics of the World Medical Association (Declaration of Helsinki).
Provenance and Peer Review: Not commissioned; externally peer reviewed.
© Autor (es) (ou seu (s) empregador (es)) 2019. Reutilização permitida de acordo com CC BY-NC. Nenhuma reutilização comercial.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use.
Correspondence / Correspondência:
João Fernandes Serodio – jserodio@campus.ul.pt
Serviço de Medicina IV, Hospital Professor Doutor Fernando Fonseca, Amadora, Portugal
IC19, 2720-276 Amadora
Received / Recebido: 20/09/2019
Accepted / Aceite: 20/01/2020
Publicado / Published: 17 de Março de 2020


{kind=link}
{kind=link}
{kind=link}