











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
Introduction
Coronavirus disease 2019 (COVID-19) is a multisystemic disease caused by the severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2), and it is considered the greatest threat to global health in the last years.
The COVID-19 pandemic led to the implementation of different control and prevention measures, such as outdoor activity restrictions, social distancing, and the closedown of government institutions, including public schools1. Despite their undeniable effectiveness in preventing the spread of infection, such measures have been associated with the deterioration of multiple health indicators.1
The lockdown has certainly had a strong impact on children and adolescents. Social distancing, the impossibility to be physically active at school or to spend time with other people gave a huge incentive to social inequality and health problems, including mental and eating disorders.1,2 In particular, the consequences were greater for individuals with increased risk for several health conditions, such as overweight or obese children.3
Obesity is considered a complex and multifactorial chronic disease, to which various genetic and epigenetic, environmental, and biopsychosocial factors contribute. According to World Health Organization (WHO), it is estimated that approximately 340 million children and adolescents aged 5-19 years old were overweight or obese in 20164. The prevalence of obesity-related comorbidities has been rising in parallel to the increasing prevalence of paediatric obesity.5,6) Furthermore, a strong stability was found between the occurrence of childhood obesity and its persistence in adulthood. The change in the food consumption patterns of children and their families, the selection of fast, processed, and high-calorie foods, associated with a growing sedentary lifestyle, have been identified as determining factors for obesity and overweight. Therefore, obesity is one of the most prevalent preventable diseases.4,5
The Covid-19 pandemic, with all the previously mentioned limitations, has been increasingly associated with the worsening of risk factors for obesity and potentially associated consequences.3 It has changed children’s eating and physical activity behaviours, exacerbating the risk factors for weight gain.7 On the other hand, the negative impact on the mental health of a young and particularly vulnerable population may have potentiated the deregulation of eating patterns and binge-eating behaviors.2
The aim of this study was to evaluate the impact on the treatment of obesity and the expression of comorbidities during the first lockdown.
Material and methods
Study Overview
Retrospective cohort study of overweight and obese children aged 6-18 years, followed in a reference outpatient clinic of paediatric obesity, since 2018. The exclusion criteria were genetic and endocrinological causes of obesity, diagnosis of chronic diseases and chronic therapies.
Family risk factors for obesity, anthropometric data [Body Mass Index (BMI) and BMI z-score], and some of the comorbidities associated with obesity (insulin resistance, dyslipidemia, hyperuricemia, impaired hepatic function, vitamin D deficiency) were evaluated.
The results presented refer to the period of six months to one year, before the first registered COVID-19 case in Portugal, and a similar period after the pandemic.
The study was conducted through the consultation of clinical processes, using a protocol previously elaborated, being always assured of the participants’ anonymity and confidentiality of all data.
Definitions
BMI z-score was classified based on WHO recommendations (BMI z-score > 1.0 ≤ 2.0: overweight; BMI z-score > 2.0: obese).8
The lipid profile was assessed after at least 12 hours of fasting and classified according to reference values of the National Cholesterol Education Program and American Heart Association. There were considered pathological values > 200 mg/dl for total cholesterol, < 40 mg/dl for HDL, > 130 mg/dl for LDL, > 100 mg/dl (0- 9 years old) and > 130 mg/dl (10-19 years old) for triglyceride.9
The prevalence of insulin resistance was estimated by applying the homeostasis model assessment for insulin resistance (HOMA-IR) and considered positive for values ≥ 3.43.10 For fasting insulinemia, we considered pathological values > 15 μIU/ml.11
Regarding fasting glycemia, fasting glucose intolerance was defined for values between 100-125mg/dL and diabetes if glycemia was > 126 mg/dL.12
For transaminases values, there were considered pathological level of alanine aminotransferase (ALT) > 26 U/L for female and > 35 U/L for male, and aspartate aminotransferase (AST) > 27 U/L for female and > 32 U/L for male.13
The reference values of uric acid levels change with age and between the sex (In male, between 5-10 years old > 4.1 mg/dl, 10-12 years old > 4.4 mg/dl, 12-15 years old > 5.6 mg/dl, 15-18 years old > 6.2 mg/dl; In females between 10-15 years old > 4.5 mg/dl and 15-18 years old > 4 mg/dl).14
In relation to vitamin D, values are considered insufficient < 20 mg/L.15
Statistical Analysis
The software SPSS version 20.0® (IBM Corp., Armonk, NY, USA) was used for the construction of databases and data analysis.
The categorical variables are presented as frequencies and percentages. Continuous variables are presented with mean and standard deviation (or 95% confidence interval), or median and interquartile range (or Q1-Q3 interval) in cases where the normal distribution of the variable was not verified through the Kolmogorov-Smirnov and Shapiro-Wilk tests. Statistical inference of continuous variables was performed using independent t-tests or Wilcoxon and Mann-Whitney tests, while for categorical variables Chi-square or Fisher's exact test and McNemar test were used. A statistical significance level of 5% was considered for all statistical tests.
Results
The study included an initial sample of 221 children/adolescents, however 150 patients were excluded by loss of follow-up and/or the absence of biochemical parameters during the COVID-19 period. Therefore, it was considered a final sample of 71 children/adolescents, predominantly female (52.1%), with a median age of 10 (7;12) years (table 1). Almost 13% were overweight and 87.3% were obese. About half of participants (51.4%) had a family history of overweight or obesity (table 1).
Table 1 Characterization of the population at admission (1st evaluation)
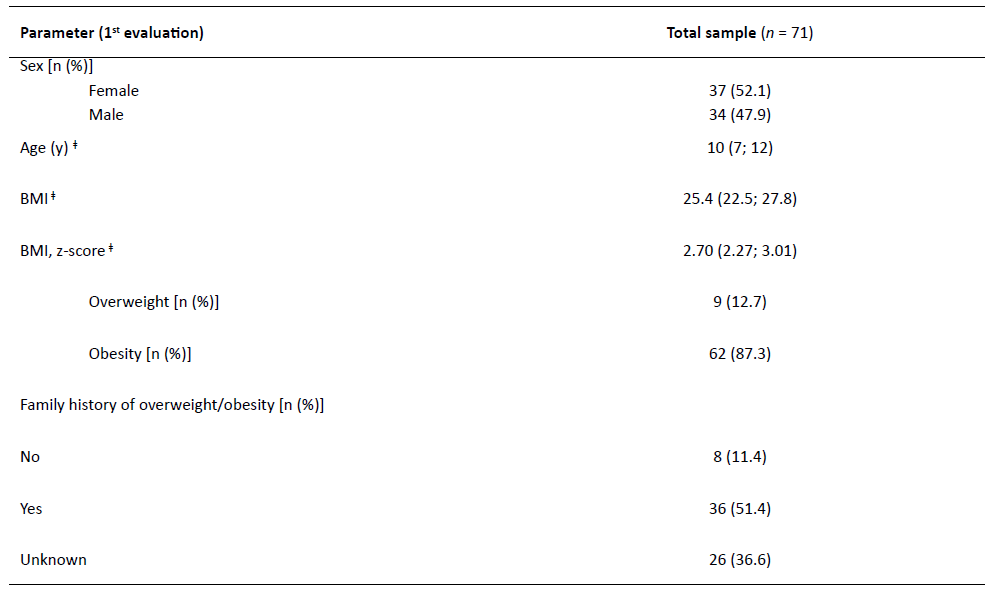
ǂ Data presented as Md (Q1;Q3); y, years, BMI, body mass index
The prevalence of obesity increased considering the evaluation before and after the COVID_19 pandemic (71.8% versus 76%, p=0.629), distinct of prevalence of overweight children who have suffered a decrease (28.2% versus 24%, p=0.629). Of the 51 initially obese patients, 7 (13.7%) had an improvement going into the overweight category. None of the children/adolescents during the study period presented a BMI normalization.
Although, the median of BMI, HOMA-IR values and the levels of insulin and AST slightly increased between the appointments before and after COVID [from 26.0 (23.0 - 28.0) to 26.8 (24.5 - 31.4), p<0.001; from 2.50 (1.40 - 3.60) to 2.90 (2.20 - 4.10), p=0.005; from 12.4 (7.38 -17.1) μIU/mL to 13.9 (10.0 - 19.2) μIU/mL, p=0.010 and from 22.0 (19.0 - 28.0) to 23.0 (16.0 - 26.0), p<0.001) respectively], no differences were observed for the remaining biochemical parameters (table 2).
Table 2 BMI/BMI z-score and biochemical parameters before and after COVID-19 pandemics
| Parameter | Median (Q1;Q3) | p-value | |
|---|---|---|---|
| Before COVID | After COVID | ||
| BMI | 26.0 (23.0; 28.0) | 26.8 (24.5; 31.4) | <0.001 |
| BMI, z-score | 2.46 (1.94; 3.01) | 2.44 (1.98; 3.02) | 0.408 |
| TC (mg/dl) | 159.0 (140.0; 180.0) | 156.5 (136.8; 170.0) | 0.859 |
| HDL-c (mg/dl) | 45.0 (41.0; 52.0) | 45.0 (40.0; 54.0) | 0.698 |
| LDL-c (mg/dl) | 101.1 (81.0; 124.0) | 101.0 (83.5; 123.0) | 0.530 |
| TG (mg/dl) | 75.0 (60.0; 94.0) | 69.5 (54.8; 102.0) | 0.685 |
| AST (U/L) | 22.0 (19.0; 28.0) | 23.0 (16.0; 26.0) | <0.001 |
| ALT (U/L) | 21.0 (15.8; 27.0) | 20.0 (15.0; 27.8) | 0.940 |
| Glucose (mg/dl) | 87.0 (83.0; 91.0) | 87.0 (83.0; 92.0) | 0.138 |
| HOMA-IR | 2.50 (1.40; 3.60) | 2.90 (2.20; 4.10) | 0.005 |
| Uric acid (mg/dl) | 4.65 (3.98; 5.35) | 5.30 (4.40; 6.20) | 0.063 |
| Vitamin D (mg/L) | 19.0 (14.6; 24.3) | 20.1 (14.0; 24.5) | 0.160 |
| Insulin (μIU/mL) | 12.4 (7.38; 17.1) | 13.9 (10.0; 19.2) | 0.010 |
BMI, Body Mass Index; TC, Total Cholesterol; HDL-c, High-density lipoprotein cholesterol; LDL-c, Low-density lipoprotein cholesterol; TG, Triglycerides; AST, Aspartate aminotransferase; ALT, Alanine aminotransferase; HOMA-IR, homeostasis model assessment for insulin resistance
Discussion
While the lockdown strongly prevented the spread of COVID-19, the restrictions resulted in unexpected lifestyle changes which led to weight gain.16 Most of the schools switched to online interactive learning, resulting in more time spent indoors, limited physical activity, and more freedom in choosing diet.16
Alarmed by some studies that reported a deterioration in the quality of life in obese and overweight children, we focused our attention on understanding how the lockdown influenced the worsening of obesity and its comorbidity.17
In our study, the majority were obese and had a family history of overweight/obesity, allowing us to understand the importance of this factor, not only due to genetic reasons but also for common and similar eating patterns. Similar studies reported an increase in obesity and BMI between the appointments before and after the COVID-19 pandemic, showing a potential aggravation in children with overweight/obesity.16,18 Still, some studies show also showed aggravation of BMI z-score.18,19 There were no studies published that showed a reduction in BMI after the lookdown.
Considering the evolution of biochemical parameters, this study revealed that the values of HOMA-IR, AST, and insulin had a significant increase between the two moments, but not in pathological values. No differences were observed for the remaining parameters. Such findings show that confinement led to aggravation in the metabolic profile. In a similar study, there was an increase, without statistical significance, in levels of HOMA-IR and insulin, but with decreased in AST.19 On the other hand, in the study of Valenzise et al, all these markers have decreased, despite the absence of statistical significance.16
Concerning the comorbidities, the number of children/adolescents with levels of HDL, TG (above 10 years), aspartate aminotransferase (among males), HOMA-IR, and insulin within values associated with adverse health effects was higher after the COVID-19 pandemic. Despite that, there wasn’t a significant worsening of the comorbidities after the lockdown, like in other similar article.16 However, consequences in the future can’t be left out.
Our study has limitations due to the small sample analyzed. This possibly occurs due to the constraints caused by COVID-19 pandemics and fear of the virus, causing loss of follow-up (missing appointments and analytical studies). Furthermore, variables such as diet and exercise, that strongly influence the weight change in children, had not been investigated in this study. Beyond that, our study identified the increase of BMI under social distancing conditions and has long-term data spanning that show weight gaining trend. Therefore, childhood obesity deserves deeper attention due to the lockdown.
Conclusion
The COVID-19 pandemic had collateral effects beyond viral infection regarding children and adolescents with overweight and obesity: the lockdown and isolation led to an unfavorable environment for maintaining healthy lifestyle behaviors.
Although we do not yet have long post-confinement measurements of BMI, based on previous studies, we can speculate that excess weight gained during the lockdown may lead to long-term consequences, such as aggravation in comorbidities.20
So, identification of the lockdown-related problems is the first step in taking preventive measures. It is fundamental to support families in maintaining healthy habits, such as developing social programs, increasing physical activity, implementing policies to make healthy food and ingredients affordable to all households, and preparing children and adolescents to remain safe and active outdoors. In the impossibility of dissociating the obese child from their family context, which is often potentiating, the approach should address their entire environment and cohabitants.
In sum, our study revealed that during the COVID-19 pandemic, there was a worsening in the magnitude of obesity. However, there were no significant repercussions on its comorbidity, which does not allow to exclude any long-term consequences.

