











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
Permalink
INTRODUCTION
Healthcare carbon footprint was responsible for 4.8% of Portugal’s emissions in 2019. Globally, the average emissions per capita for healthcare activities was 0.28 tons CO2-equivalents (tCO2e) and in Portugal it was 0.35 tCO2e.1
The “green nephrology” and “eco or green dialysis” concepts were created to draw attention to the nephrology’s environmental impact and to promote attitudes that minimize its ecological footprint.2,3
Dialysis has a particularly significant carbon footprint (CFP), with chronic resource consumption and waste generation that is disproportionally high compared to other medical therapies. An Australian study has estimated a CFP for conventional hemodialysis (HD) at 10.2 tCO2e/patient/year - eight times the average healthcare footprint per capita in Australia (1.29 tCO2e/capita/year) and accounting for more than two-thirds the estimated Australian mean annual per capita CFP of 15.4 tCO2e.4,5 In the United Kingdom (UK), HD is estimated to be responsible for 3.8 tCO2e/patient/year, more than 7-fold the average per patient CFP in UK healthcare.5,6
The prevalence of end stage renal disease (ESRD) is increasing, and Portugal has one of the highest prevalence rates in the world.7
This topic has gained particular relevance, not only because nephrology has a significant environmental impact, but also environmental changes are associated with a higher rate of kidney diseases - people living with kidney disease are particularly vulnerable to the effects of climate changes - there is a bidirectional relationship between environment and nephrology.3,8
The aims of this study were to document Portuguese nephrologists’ current practice and attitudes towards environmental sustainability (ES) and expected barriers regarding new efforts on ES. Establishing the baseline ES attitude across Portuguese Nephrologists can guide future initiatives. It was also designed to support a clinical transformation toward a lower carbon kidney care by identifying fruitful áreas of attention. At the same time these surveys act as educational tools, impelling the responders to ponder on their attitudes.
METHODS
Based on a literature review conducted through PubMed, two surveys were developed: one for chief of nephrology departments (CD) and another for all nephrologists’ members of the Portuguese Society of Nephrology (SPN).
The questionnaire consisted of 18 (CD’s survey) and 24 (nephrologists’s survey) questions, mainly multiple-choice or Likert scale questions assessing: demographic data; value placed on ES and prior education on this topic; ES efforts and barriers; personal and departmental plans regarding ES; “mini quiz” questions regarding the environmental impact of nephrology in order to evaluate the knowledge of the responders. In the CD’s survey, questions related to the Units organization regarding sustainability and preparation for extreme weather conditions, were also included. A free-text box was also provided at the end of both surveys, and responders were invited to add information they considered to be relevant.
The survey was tested in advance using a convenience sample of three nephrology fellows and three staff nephrologists. Feedback indicated no significant changes were needed.
Twenty-nine adult public renal units were identified and a personalized email asking for participation was sent to the respective CD with a link to the survey. An invitation letter with a link to the survey was emailed by the SPN office, on behalf of the investigators, to all SPN members, including fellows. The surveys remained available for one month after the email had been sent. All responses were anonymous, and consent was implied by participation in the survey.
Data was collected and managed using forms.office.com®. Descriptive statistics were generated with STATA14® as proportions of responders. Given a potential study population of approximately 600 nephrologists and fellows (estimated number of SPN members), the minimum sample size required was estimated a priori to be 121 participants for a margin of error of 8% with a 95% confidence level.
RESULTS AND DISCUSSION
The number of responders was 153 (25.5% response rate, considering the estimated number of 600 SPN associates at the time), 17 were answers to the CD survey (corresponding to 58.6% of the renal units).
Among all responders: 11% (n=17) were CD; 23.5% (n=36) nephrologists with coordination roles (NCR), 39% (n=60) nephrologists and 26% (n=40) nephrology fellows (NF). Most responders worked in Units in the south region (49%, n=75), followed by the center 22.2% (n=34), north 24.2% (n=37) and Madeira or Azores islands 4.6% (n=7). Median age of responders was 34.5 years (IQR 30-51; minimum 25 and maximum 70).
How is Environmental Sustainability Perceived by Portuguese Nephrologists?
The median priority attributed to sustainability in a scale of 5 was 4 (IQR 3-5) and 70.2% gave at least 4 points. There was a significant difference in the priority attributed between categories: CD - 3 (IQR 3-4), NCR - 4 (IQR 4-5), nephrologists - 4 (IQR 3-5) e NF - 4 (IQR 3-5), p=0.049.
Only one department had formed an active green group or elected a green person (n=1, 5.9%), but 13 Units were currently undertaking at least one green project (n=13, 76.5%). These results show that the nephrology community gives value to this topic, which are in line with the EDTNA/ERCA Conference results where 72% considered mandatory to support the “Go Green in Dialysis” project.9
Education and Strategies to Increase Recycling and Sustainability
The median reported confidence level on sustainability (in a scale from 1 to 5) was 3 (IQR 3-4). Only 44% (60/136) agreed or strongly agreed (levels 4 and 5) that their level of knowledge about environmental impact of nephrology was sufficient to guide their practice.
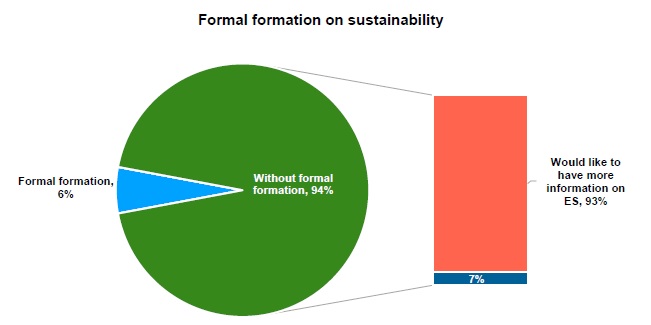
The median reported confidence of CD on sustainability was 5 (IQR 4-5, 94.12%) and they auto-evaluated their median knowledge degree in this field as 4 (IQR 4-5). Less than six percent of respondents (8/136, 5.9%) had received prior formal training on this topic, but more than 90% of responders indicated that they were likely to seek more information on the topic (119/128, 93.0%) (Fig. 1).
Respondents identified conference lectures on nephrology meetings, discussion of this topic within each Nephrology department and online e-modules as the preferred modes of training.
This survey showed that Portuguese nephrologists are very willing to receive more information and education on sustainability. The environmental impact of nephrology is rarely discussed at environmental conferences and medical conferences. The healthcare and/or nephrology ES impact and sustainability should also be added to the formal curriculum during fellowship training.
Waste Production and Resources Consumption
Measurement
The majority of departments (n=12, 70.6%) had never performed any kind of ES audit (e.g., regular measurement of energy and water collection of some data regarding resources consumption or waste production, only one collects both global and sectorial (hemodialysis) data for energy and water consumption and waste production.
Renal units should undertake waste audits (at routine intervals to monitor waste production and segregation) and measure water and energy consumption - all these measurements should be indexed per patient or per treatment, to be useful tool to guide the definition of goals, raise awareness and promote changes.
Recycling
Nearly all responders (130/136, 95.6%) either agreed or strongly agreed that they recycled at home, however only 99 (72.8%) recycle at least one type of waste at the hospital. The two most recycled items at hospitals were cardboard/paper and plastic.
In addition to the absolute weight reduction, the waste composition is also relevant to the management of waste. Triage of contaminated and non-contaminated (domestic) waste should be the cornerstone of hospital waste management - the appropriate triage avoids the “contamination” of potentially recyclable materials at the site of production.10
Effective waste segregation at source requires staff education and facilities, it is not necessarily time-consuming, but it does require attention and training, and should be regularly audited.10 Recycling bins for non-clinical packaging and plastic wastes should be available in visible places. Waste management has not only ecological advantages, but also a relevant economic impact, these hidden costs may allow significant savings with “zero costs” and no impact on quality of care.
Water Conservation
Presently only three surveyed hospital HD units (17.6%) have installed systems to reuse the reverse osmosis (RO) reject water for use elsewhere (e.g., water gardens, toilets, etc.). In the same direction, only 25% and 19% of the facilities in an Australian11 and in a European12 survey, respectively, conserve RO reject water for reuse. We should note that our survey only evaluated hospital units, and our empiric data suggest that the proportion of reuse of RO rejected water in peripheral units can be higher (but not universal).
The RO rejected water is “purified” tap water that has never been in contact with the patient. It has already been filtered by the particles and carbon filters, to remove chlorine, chloramines and other potentially harmful substances. This water is commonly considered unfit for human intake due to a lack of chlorine and a mild increase in conductivity.13-16Although this water can be used for alternative purposes such as sanitation systems, laundry, street washing, gardening, etc. A structure to harnessing this water would require some initial investment, but would become profitable after a few years (in the UK up to 4 492 000 L of water and 10 558 GBP/year in one unit were saved) and should be a priority in new units.
A structure to harnessing this water would require some initial investment, but would become profitable after a few years (in the UK up to 4 492 000 L of water and 10 558 GBP/year in one unit were saved)17-19 and should be a priority in new units.16-20
On the same page the replacement of HD machines by more eficiente models and the implementation of more efficient water purification systems with lower proportion of reject water may lead to significant water savings.
Central dialysate delivery systems (CDS)
Only half of the hospital HD facilities had local on-line dialysate production (n=9, 53%). CDS with preparation of acid dialysate concentrate on-site can be effective in decreasing greenhouse gas emissions by reducing transportation of the concentrate canisters (distribution chain footprint), avoiding the disposal of any residual concentrate at the end of the session (standard fluid cartridges sizes, not adjusted to each patient/situation) and the use and disposal of plastic containers.
The “Green Excellence in Dialysis” - a joint EDTNA/ERCA initiative, a European multicentric study in 13 countries, found that only 29% of the surveyed units analyzed had on-line dialysate production.12 If the Unit does not have CDS, flexible bags should be chosen (they require less packing material and plastic) and their size should be adjusted to the amount of dialysate needed to each patient (avoiding waste).
The total annual savings from a CDS can reach, for a unit delivering 3000 L of dialysate per week (Central Manchester University Hospitals NHS Foundation Trust): 24,461 kWh of electricity; 428 064 L of water, reducing deliveries by 75% and saving £13 400 per year.21
Sustainability as a Criteria of the Procurement Process
Only two facilities (11.8%) declared that ES was considered in all procurement decisions, and 35.3% (n=6) admitted that it is seldom or never considered in the decision (median weight attributed by CD to sustainability as a criterion in products choice was only 3, IQR 2-4). In nephrology the environmental impact of a product or device is not regularly included as a selection criterion. The widespread incorporation of measurable sustainability criteria into procurement contracts will incentivize improvements and competition within the industry. The contribution of manufacturers of medical equipment toward a greener nephrology, is mandatory and a close relationship between industry and healthcare providers is crucial.22
The chosen criteria should be measurable in order to compare different options, for example: resource consumption in the product development and production processes (water, energy, etc.), waste production, recyclability of certain product components and reduction of the single use approach of medical devices. This analysis should also include the definition of the “full life-cycle” of a product (circular economy).13
Climate Change Preparedness
Emergency strategies were in place to cover interruptions to power supply in 12 units (70.6%) and to water supply in ten units (58.8%), and alternative plans in case of extreme weather conditions that preclude transportation services were only considered in three (17.6%).
Just two (11.8%) facilities had policies and emergency plans in place to address all the three dimensions (water, energy, and transportation interruptions). Similarly, the Australian survey found that climate changes adaptations are also not effectively adopted.11
The frequency of extreme weather events is predicted to increase in coming decades due to climate changes.19 However, this survey showed limited climate change preparation across Portugal public dialysis units.
General measures
Renal Units provided recycling bins for paper in 15 units (88.2%) and recycling bins for plastic in 13 (76.5%). All or almost all computers in these units had the standby mode on.
We found that printers in renal units are frequently set to print double-sided (64.7%, n=11/17); clinical records are exclusively (88.2%, n=15/17) or almost exclusively (11.8%, n=2/17) deployed on-line in most of the Units.
Light movement sensors for common facilities are installed only in three units (17.6%). Energy consumption may be further reduced by simple actions, such as turning lights and computers off at the end of daily activities or the use of low-energy lighting.
Only seven centres (41%) reported regular use of teleconferencing to replace staff meetings.
Barriers to Environmentally Sustainable Practice
The most reported barriers to sustainable practices were: inadequate information or education (124/136, 91%); lack of adequate facilities (128/136, 94%), concerns about security (infection control and contamination of waste with biologic fluids) (110/136, 81%) and legal norms and orientation (105/136, 77.2%). Some responders shared comments highlighting concerns about contamination of recyclable materials with biologic fluids.
Further training may overcome some of the unfounded concerns identified and give more confidence to change attitudes. As other countries, Portuguese legal regulations concerning medical waste management are ancient, inadequate and unsuitable to the current reality.
Staff Travel
The great majority of the responders travel to the hospital by private car, and only a very small minority (n=18, 13%) uses “no greenhouse emissions” modes of transportation (walking or bicycle) or shared modes of transportation (n=8, 6%).
“Mini Quiz”
1. Which kidney replacement therapy is more eco-friendly?
Responders ranked the different renal replacement therapies from higher to lower environmental impact to those with the lower:
- Home long nocturnal HD
- Automated peritoneal dialysis
- Continuous ambulatory peritoneal dialysis (CAPD)
- Kidney transplantation
There is limited data on the comparison of the overall ecologic burden between different kidney replacement modalities. Home HD (as peritoneal dialysis) allows to reduce the burden of home-centerhome transportation; however, home HD is often synonymous of more frequent and longer dialysis sessions. It was estimated that regarding transportation (in the UK thrice weekly ICHD has a CFP of 3.82 kg CO2e per patient per year, travel being responsible for 20% of the CFP),9 home-HD can save 0.73 to 0.96 tCO2e/patient/year, approximately 13% CO2e comparing to in center HD.23,24 These savings in the home HD are outweighed if the patient performs more than three treatments per week (more disposable HD sets are used) or longer treatments.24 The CFP of providing home HD varies with the regime: 4 times weekly (4 days, 4.5 hours), 4.3 tCO2e; 5 times weekly (5 days, 4 hours), 5.1 tCO2e; nocturnal (3 nightly, 7 hours), 3.9 tCO2e; and nocturnal (6 nightly, 7 hours), 7.2 tCO2e.24
Peritoneal dialysis might be perceived as more environment-friendly, because of its direct lower water and energy load needed (mainly for CAPD). This evaluation fails to account for the energy and water that is consumed to prepare peritoneal dialysis fluid or to the manufacturing of its plastic packages and the required transportation of solutions from the place of production, sometimes overseas, to the patients’ home (the point of care) - this information remains unknown (it is not published by producers).10,25 Thus, although its environmental impact has been poorly studied, it is likely also elevated. In short, all the current dialysis modalities are not environmentally sustainable.
The renal transplantation´s environmental impact was calculated as 90%-95% less than hemo- or peritoneal dialysis, being the most sustainable modality.26
2. Which areas have higher impact on the CFP of a nephrology department?
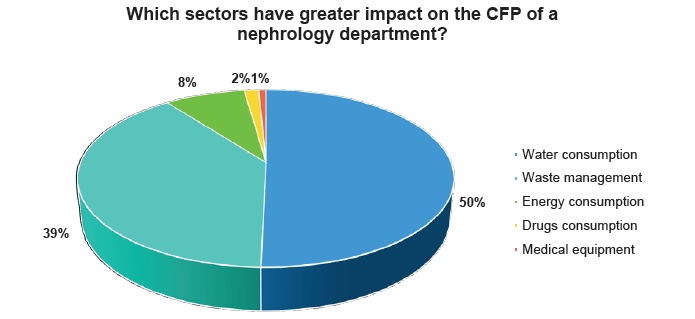
The water consumption (50% of the responders) followed by waste management (39% of the responders) were considered the main áreas responsible for the high CFP of nephrology (Fig. 2). Our results highlight that nephrologists are unaware of the areas responsible for a greater CFP, focusing their attention on the impact that is most visible.
Although only 2% of our responders attributed the highest footprint to drugs (Fig. 2), several studies have pointed that drugs may have the highest CFP (more than dialysis itself) in renal care activities.4,6,27
In the same direction, nephrologists are aware and concerned about the impact of water consumption on its CFP, however water consumption has low CFP. Nevertheless, water is a scarce source and needs to be used carefully. Some studies suggested that the largest water footprint is related to drug consumption even in HD patients. 27
Only one study was found evaluating the CFP of a comprehensive nephrology department, one that covers a population of 865 000. In this Unit the total GHG emissions distributed by functional departments were: 65.4% to the HD (225 patients) and peritoneal (54 patients) dialysis, 30.5% procurement, 27.4% to the inpatient ward (14 bed ward) and 5.7% to the outpatient department (7800 appointments per year). On the other hand, the distribution of the total CFP considering the activity areas was: 35% to the pharmaceutical subsector, 25% to the medical equipment, 15% to travel (HD represents 34% of overall travel emissions), 13% to facility energy and 8.7% to waste.6
3. Are strategies for improving environmental sustainability in nephrology units economically viable?
The great majority of the responders (n=111, 81.6%) recognized that implementation of more eco-friendly strategies in nephrology Units is associated with the need for an initial investment but longterm savings. To decision makers, the perceived additional costs to deliver more environmentally friendly care are often a barrier to the adoption of sustainable solutions. Many of the necessary changes to improve ES in nephrology will result in significant longer term cost savings and provide additional financial sustainability over time.5
Limitations:
Our survey has some potential limitations. First, a selection bias: although the surveys were sent to all nephrology department heads and nephrologists, the topic in analysis was clear at the survey’s title, selecting more environmentally concerned and more eco-friendly responders naturally more willing to be aware of environmental concerns and who have an eco-friendlier behavior. Second, the survey was sent only to hospital nephrology departments, leaving aside private HD clinics, where most patients are dialyzed. Several questions called for subjective responses, for instance, asking for an estimation of how comfortable they are with sustainability, rather than requiring objective measurements.
CONCLUSION
One of the most important barriers to a greener nephrology is the lack of awareness among nephrologists about the ecological burden of nephrology. Units need to measure their impact and define goals.
Portuguese nephrologists demand for educational programs on ES.
The surveys suggests that little attention is given to environmental impact in the procurement process in nephrology - it is urgent to embed sustainability criteria into this process.
To have a real impact, the contribution of all players (manufacturers, politicians, decision-makers, etc.) and at all levels (international, national, regional and local) is necessary.
The healthcare national authority should survey the nephrology and HD units about its ecological impact, environmental efficiency goals and results. New facilities must be built and organized with a more sustainable rationale in mind.
There are several and relevant opportunities to improve the Portuguese nephrology ES, with benefits on the healthcare quality and cost reduction. These surveys can be a starting point to implement
new strategies to reduce the ecologic impact of nephrology. In the coming decade we will probably not reach a thoroughly green nephrology, but we can have a greener nephrology.

