










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkPortuguese Journal of Nephrology & Hypertension
versão impressa ISSN 0872-0169
Port J Nephrol Hypert vol.34 no.2 Lisboa jun. 2020
https://doi.org/10.32932/pjnh.2020.07.077
CASE REPORT
Neutropenic enterocolitis (typhlitis) in a kidney transplant patient: A case report
Rita Valério Alves1, Luís Falcão2, Elsa Soares3, Milena Mendes4, Patrícia Cotovio5, Fernando Caeiro5, Inês Aires5, Cecília Silva5, Francisco Remédio5, Aníbal Ferreira5, Fernando Nolasco5
1 Nephrology department, Centro Hospitalar Médio Tejo - Torres Novas, Portugal
2 Nephrology department, Hospital Beatriz Ângelo, Portugal
3 Nephrology department, Centro Hospitalar de Setúbal, Portugal
4 Hepatobiliopancreatic and transplantation centre, Centro Hospitalar Universitário Lisboa Central, Portugal
5 Nephrology department, Centro Hospitalar Universitário Lisboa Central, Portugal
ABSTRACT
Typhlitis is a clinical entity rare in adults, reported in immunosuppressed patients. It is a life-threatening condition that occurs in neutropenic patients due to compromised integrity of the bowel wall and its exact pathogenesis is not completely understood. We report a 35-year-old man with a post deceased donor renal and pancreas transplantation status who presented fever and febrile neutropenia. Three days after admission he presented hematochezia with a hemoglobin drop. Colonoscopy revealed "ileum mucosa with multiforme ulcers" and since no other etiology was found, typhlitis was considered. He gradually improved with support treatment and was able to be managed non-operatively.
To our knowledge, there are only six other reports of typhlitis in kidney transplant recipients.
Key-words: Neutropenic enterocolitis, typhlitis, kidney transplant
INTRODUCTION
Neutropenic enterocolitis (NE), or typhlitis, is a clinical entity initially described in pediatric leukemic patients.1 Although it is uncommon in adults, it has been reported in people with hematologic malignancies, as well as other immunosuppressive causes, such as AIDS, therapy for solid tumors and organ transplants.1 NE is a rare life-threatening condition that occurs in neutropenic patients due to compromised integrity of the bowel wall.2
The exact pathogenesis of NE is not completely understood. The main elements in the disease onset appear to be intestinal mucosal injury together with neutropenia and the immunocompromised state of the afflicted patients and also the direct mucosal damage by cytotoxic drugs.1-3 The process has a predilection for the terminal ileum and cecum, but any segment of the bowel can be involved.4
NE is characterized by bowel wall edema, engorged vessels, disrupted mucosal surface and ulceration, which become susceptible to bacterial intramural invasion, translocation and hemorrhage and can rapidly progress to intestinal perforation, multisystem organ failure, and sepsis.2
The histopathological features are marked hemorrhagic necrosis, mucosal ulceration, extensive edema in the submucosa and laminal propria, marked congestion and even deep mural and transmural necrosis, significant infiltrative inflammation should be absent in NE due to the profound neutropenia.5
Patients present symptoms such as abdominal pain, fever, abdominal distention, nausea, vomiting, and diarrhea, with or without blood, with coexisting neutropenia in the at-risk patient population.4
NE should always be considered in the differential diagnosis of acute lower quadrant pain in immunosuppressed patients, since it has a nonspecific presentation that can mimic many other diagnoses.1,2
The management of these patients remains challenging: bowel rest, intravenous fluids and broad spectrum antibiotics with parenteral nutrition are the principles of the treatment.4,5 Surgical intervention is necessary only when complications such as hemorrhage or bowel perforation develop.5
CASE REPORT
A 35-year-old melanodermic man, diabetic type 1 from the age of 13, developed end-stage kidney disease and started renal substitution therapy in 2013. In May 2019, he underwent deceased donor kidney and pancreas transplantation. He was cytomegalovirus (CMV) antibody-positive, seronegative to human immunodeficiency virus (HIV), hepatitis B virus (HBV) and hepatitis C virus (HCV) and there were three human leucocyte antigen (HLA) mismatches. After the initial immunosuppression treatment with thymoglobulin (cumulative dose 970 mg - 12.1 mg/kg), he was placed on triple immunosuppression with prednisolone, mycophenolic acid and tacrolimus. The patient also received daily valganciclovir and trimethoprim-sulfamethoxazole prophylaxis. The patient was evaluated weekly at pos-transplantation consultation. The baseline kidney function was serum creatinine 1.4-1.6 mg/dL and serum urea 21-75 mg/dL. Tacrolimus levels at previous medical appointments were between 6 mg/dL and 7 mg/dL.
The last appointment prior to admission was 7 days before. At this time, the patient was receiving prednisolone 15 mg daily, tacrolimus (4 mg + 3.5 mg daily), mycophenolic acid (540 mg + 360 mg daily), valganciclovir 450 mg daily and trimethoprim-sulfamethoxazole 480 mg daily. The lab results presented hemoglobin 12.1 g/dL; leucocytes 5.58 x 109 /L (neutrophils 4.62 x 109 /L); serum creatinine 1.73 mg/dL; urea 68 mg/dL; pancreatic amylase 68 U/L; pancreatic lipase 125 U/L; PCR 1.2 mg/dL, tacrolimus (FK) 4.74 ng/mL and blood CMV PCR not detected.
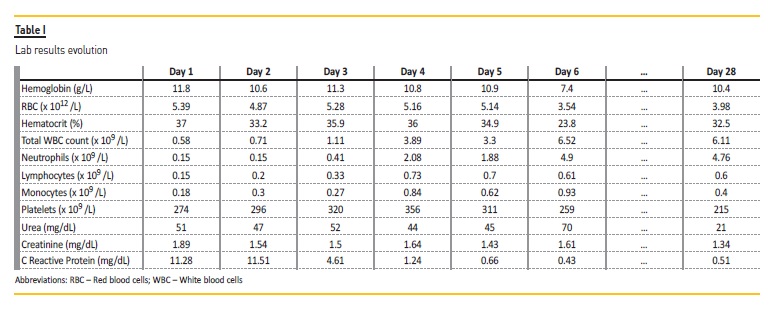
Two months post-transplant, the patient was hospitalized with a febrile neutropenia (leucocytes 0.58 x 109 /L; neutrophils 0.15 x 109/L), without changes in kidney and pancreatic function (pancreatic amylase 46 U/L; pancreatic lipase 60 U/L), an increased PCR and FK 4.74 ng/mL (Table 1).
His physical examination upon admission, including abdominal and genitourinary examinations, revealed fever (temperature 38.2 °C), well-healed transplant scars and a palpable, non-tender renal allograft.
Tacrolimus and prednisolone doses were adjusted, while mycophenolic acid, valganciclovir and trimethoprim-sulfamethoxazole were discontinued. Blood and urine cultures were obtained, and he was started on G-CSF filgrastim (360 mcg /day) and empiric meropenem (1g every 8-hours). 3 days after the admission the patient presented hematochezias.
Initially, hematochezias were auto-limited; however, his status progressed unfavorably, and a 4.0 g/dL hemoglobin drop (Table 1) was detected. The patient's status was unaltered after the blood transfusion and the lowest verified hemoglobin value was 5.7 g/dL.
In this context, he was admitted in the intensive care unit, where an endoscopy and a colonoscopy were performed and revealed "blood all over the colon", "colon and rectum without mucosa changes" and "ileum mucosa with multiforme ulcers of different sizes", of which biopsies were acquired. It was hypothesized that it was a cytomegalovirus ileitis and the patient started valganciclovir in treatment dose (900 mg every 12-hours).
At day 5, the patient had no fever, the leucocyte count was normal, and the blood and urine cultures were negative.
To exclude other possible ileitis etiologies, other tests were performed: stool culture was negative for common bacterial and parasitic pathogens, C. difficile toxin test was negative, mycobacterial blood cultures were negative, thorax computerized tomography (CT) excluded pulmonary tuberculosis and CMV PCR in blood was repeated (at admission it was negative). The abdominal CT did not identify an active hemorrhage or other pathologic changes. The mucosa biopsies were inconclusive ("Proximal intestine mucosa without changes and small ulcer fragment. Immuno-histochemistry study for CMV negative.
Ziehl-Neelsen bacillus negative. The changes are mild and unspecific."). It excluded CMV ileitis since CMV PCR in colonic mucosa was negative and Valganciclovir was decreased back to the prophylactic dose. The patient had several episodes of grossly bloody diarrhea during his hospitalization and required seven blood transfusions. However, he gradually improved and was able to be managed non-operatively. The last blood panel before discharge is presented in Table 1.
Before home discharge, after 28 days, the patient was submitted to another colonoscopy that showed ileum superficial ulcers in recovery and it was suggested by the Gastroenterologist that the final diagnosis was a neutropenic enterocolitis (typhlitis), since all other complementary diagnostic exams failed to provide an alternative diagnosis.
DISCUSSION
We found 6 reports of NE in kidney transplant patients: 4 in an 8-year review of NE in a surgical center6 and two published as case reports.
The first case report was from a patient with a biopsy-proven acute vascular rejection, treated with methylprednisolone pulses at day 19 post-transplant,7 and the second from a pediatric renal transplant patient with 9 months transplant and after three methylprednisolone pulses at month7,8. Both case reports refer to an increase of the immunosuppressive medication prior to the episode of NE; however, in our patient there were no changes in immunosuppressants prior to the admission and the tacrolimus level was not elevated.
A few risk factors that may have predisposed our patient to the development of NE were the treatment with an antimetabolite (mycophenolic acid) and treatment with other myelosuppressive medications such as prophylactic antibiotics and antivirals (9).
Although NE is most often associated with hematologic malignancy, other immunosuppressed and neutropenic patients without malignancy are at risk as well, as demonstrated in our case report.
Therefore, this is a diagnosis that should be considered in any neutropenic patient, including those who have recently undergone transplantation, with abdominal pain, fever, diarrhea, bloody stool, and appropriate radiographic findings of bowel thickening, dilation/distention, or pneumatosis.
Unfortunately, in our case, the abdominal CT performed did not show the typical bowel thickening and it was not possible to confirm which of the segments were affected.
Additionally, the biopsy fragments of the ileum mucosa were small, and the specific characteristics described in the articles were not found, but CMV infection was excluded.
The histologic examination is the gold standard for the diagnosis, but colonoscopy is relatively contraindicated in NE patients, as air insufflation may result in bowel perforation. This is an additional element at the attention of nephrologists.
This is an exclusion diagnosis and an extensive workup is necessary to rule out other possible causes. Nephrologists should remain vigilant for this condition in post-transplant patients.
References
1. Rodrigues FG, Dasilva G, Wexner SD. Neutropenic enterocolitis. World J Gastroenterol. 2017;23(1):42-7. [ Links ]
2. Tamburrini S, Setola FR, Belfiore MP, Saturnino PP, Della Casa MG, Sarti G, et al. Ultrasound diagnosis of typhlitis. J Ultrasound [Internet]. 2019;22(1):103-6. Available from: https://doi.org/10.1007/s40477-018-0333-2 [ Links ]
3. Satyanarayana G. Work-up for fever during neutropenia for both the stem cell transplant recipient and the hematologic malignancy patient. Infect Dis Clin North Am. 2019;33(2):381-97. [ Links ]
4. Bayasi M, Quiogue J. Noninfectious colitides. Clin Colon Rectal Surg. 2015;28(2):87-92. [ Links ]
5. Xia R, Zhang X. Neutropenic enterocolitis: A clinico-pathological review. World J Gastrointest Pathophysiol. 2019;5330(3):36-41. [ Links ]
6. Snydman DR, Nesher L, Rolston KVI. Neutropenic enterocolitis, a growing concern in the era of widespread use of aggressive chemotherapy. Clin Infect Dis. 2013;56(5):711-7. [ Links ]
7. Bueno Lledó J, Serralta Serra A, Hernandis Villalba J, Planells Roig M, Rodero Rodero D. Tiflitis aguda en el paciente inmunodeprimido: Nuestra experiencia en 8 años. Rev esp enferm dig.2003;95(1):30-9. [ Links ]
8. Frankel A, Barker F, Williams G, Benjamin I, Lechler R, Rees A. Neutropenic enterocolitis in a renal transplant patient. Transplantation. 1991;52(5):913-4. [ Links ]
9. Pelletier JH, Nagaraj S, Gbadegesin R, Wigfall D, McGann KA, Foreman J. Neutropenic enterocolitis (typhlitis) in a pediatric renal transplant patient. A case report and review of the literature. Pediatr Transplant. 2017;21(6):10-2. [ Links ]
Rita Valério Alves
Nephrology Department, Av. Dr. Xanana Gusmão, 45.
2350-754 Torres Novas. PORTUGAL
E-mail: anarita1990@gmail.com
Disclosure of potential conflicts of interest: none declared
Received for publication: Nov 19, 2019
Accepted in revised form: Jun 7, 2020


{kind=link}