










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkPortuguese Journal of Nephrology & Hypertension
versão impressa ISSN 0872-0169
Port J Nephrol Hypert vol.34 no.2 Lisboa jun. 2020
https://doi.org/10.32932/pjnh.2020.07.073
REVIEW ARTICLE
Kidney-induced osteoporosis: a new entity with a novel therapeutic approach
Ana Beatriz de Oliveira Pereira1,João Miguel Machado Dória Frazão1,2,3,4
1 Faculty of Medicine of the University of Porto
2 Institute of Investigation and Innovation in Health, University of Porto, Portugal
3 INEB - National Institute of Biomedical Engineering, University of Porto, Portugal
4 Department of Nephrology, São João Hospital Center, Porto, Portugal
ABSTRACT
Over the past century, important scientific advances have been made regarding the complex pathophysiology of bone disease in renal patients. Bone disease in renal patients is included in a wider spectrum of disease, the CKD‑mineral bone disorders (CKD‑MBD).
Older patients with CKD can present with both age‑related osteoporosis and renal osteodystrophy. Clinicians are now challenged with the need to prevent fracture in these CKD patients, where the efficacy and safety of pharmacologic agents used for the general osteoporotic population have not been studied. Treatment of renal osteodystrophy has been focused on control of the parathyroid secretion with calcitriol, vitamin D analogs and calcimimetic agents. However, there is an increase in fractures with aging in patients with CKD, suggesting that these patients also have the fracture risk factors common to the general population, such as age. Pharmacologic agents, such as teriparatide, denosumab and romosozumab have been developed for osteoporosis treatment with a direct effect on bone cell activity, osteoblasts and osteoclasts. This article reviews the derangements in bone turnover, mineralization and volume in CKD‑MBD.
In addition, we will also discuss strategies to manage osteoporosis in CKD and the available data on the new pharmacological agents in CKD‑patients.
Keywords: chronic kidney disease‑mineral bone disease, denosumab, osteoporosis, renal osteodystrophy, romosozumab, teriparatide
INTRODUCTION
Since 1942, the term renal osteodystrophy (ROD) has been used to describe the bone disease resulting from chronic kidney disease (CKD) (1, 2). Over the past century, important scientific advances have been made regarding the complex pathophysiology of CKD‑mineral and bone disorders (CKD‑MBD).
In 2005, the entity CKD‑MBD was created in order to integrate not only the bone disease related to CKD, but also the laboratorial abnormalities in mineral metabolism biomarkers, and the vascular calcifications1. In consequence, ROD is a component of the syndrome CKD‑MBD, which is used broadly to also describe laboratory abnormalities of mineral metabolism and soft‑tissue calcifications (3, 4). CKD‑associated osteoporosis (OP) should be recognized as a component of CKD‑MBD, despite the poor understanding of the underlying pathophysiology, and better predictive scores are required to identify patients at high risk of bone loss and fracture. Clinicians are challenged with the need to prevent fracture in patients, where the efficacy and safety of pharmacologic agents has not yet been supported by solid scientific evidence4. Older patients with CKD‑MBD can present with both age‑related OP and renal osteodystrophy.
The distinction between these two entities is challenging without a bone biopsy.
For decades, treatment of renal osteodystrophy has been focused on control of the parathyroid hormone (PTH) secretion with calcitriol, vitamin D analogs and calcimimetic agents. However, there is an increase in fractures with aging in patients with CKD, suggesting that these patients also have the fracture risk factors common to the general population, such as age. New drugs have been developed for osteoporosis treatment with a direct effect on bone cell activity, osteoblasts and osteoclasts. Low turnover bone disease, a subtype of CKD‑MBD, could benefit from parathyroid hormone therapy, which is anabolic in OP. On the other hand, the monoclonal antibody against receptor activator of NF‑κB ligand (RANK‑L), denosumab, which inhibits osteoclast activity and proliferation, could be helpful in cases with high turnover bone. Romozumab, which inhibits osteoclasts and stimulates osteoblasts, is a monoclonal antibody inhibiting sclerostin that could provide anabolic and anti‑resorptive effects.
The emerging recognition that the bone metabolism is linked to the development of cardiovascular disease should prompt us to take into consideration the effects of the treatment of bone disease on the vasculature, as well as highlight the high burden of CKD‑MBD on mortality1. Also, the consideration of CKD‑MBD as a systemic spectrum should prepare us to face the extra‑bone effects of therapies targeting bone cells activity, mainly in the cardiovascular system. Therefore, new biological drugs could benefit patients with CKD‑MBD, with either OP or ROD, but cautious attention must still be paid to the extra‑bone effects3.
This article reviews the derangements in bone turnover, mineralization and volume in CKD‑MBD.
A brief review of the pathophysiology of CKD‑MBD is included. In addition, we will discuss management strategies targeting bone volume and the safety and efficacy in CKD patients of some pharmacologic agents currently used for the treatment of osteoporosis in the general population.
DERANGEMENTS IN BONE TURNOVER, MINERALIZATION, AND VOLUME IN CKD PATIENTS: THE "TMV" CLASSIFICATION
Classical categories of renal osteodystrophy are high‑turnover bone (in the past, described as "osteitis fibrosa"), low‑turnover bone, osteomalacia and mixed uremic bone lesions. More recently, the "TMV" classification has been proposed, since there is an agreement that turnover (T), mineralization (M) and volume (V) are the most important aspects when describing the different bone histological categories. Each form of renal osteodystrophy could have high, normal or low bone volume.
Patients with hyperparathyroidism will typically have high turnover, normal mineralization, increased cancellous bone volume and decreased cortical bone volume1,5. Bone biopsy is the gold standard for determining the different types of ROD, since the available biochemical markers are not completely reliable3. Ott et al recognize that the "TMV" system includes the most important points, but suggest that it should also include aspects that are associated with bone strength, such as three‑dimensional trabecular structure, connectivity, degree of microdamage, collagen structure and cross‑linking, and the crystal size. According to this author, the goal for future generations will be to obtain all the important clinical information noninvasively1. Malluche HH et al performed a study with six hundred and thirty bone biopsies from adult CKD G5D patients evaluated by histomorphometry, using the "TMV" classification. The study showed racial differences, with white people revealing predominantly low turnover and the same proportion of low, normal or high cancellous bone volume. Black patients revealed predominantly normal or high turnover and a higher proportion of high cancellous bone volume. This study found a high prevalence of low cancellous bone volume. Vertebrae are essentially composed of cancellous bone, whereas long bones are mainly constituted by cortical bone. Therefore, low cancellous bone is associated with a higher risk for compression fractures of the spine, and cortical porosity with hip fractures. Patients with a low cancellous bone volume had thin cortices with normal cortical porosity, while patients with high cancellous bone volume had normal cortical thickness with high porosity, mostly due to hyperresorption. No apparent association between resorption parameters and low bone volume was found; thus hyperresorption does not contribute notably to low cancellous bone volume. Therefore, these authors concluded that it is improvable that antiresorptive agents improve low bone turnover, and so low bone volume.
Consequently, changes in present pharmacological management of the CKD‑MBD are necessary, since low bone volume and low bone turnover are a common subtype of the CKD‑MBD spectrum5.
KIDNEY‑INDUCED OSTEOPOROSIS: A NEW ENTITY IN THE CKD‑MBD SPECTRUM
Bone abnormalities are common complications of CKD, and they start early in the progress of CKD, usually with glomerular filtration rate below 90 mL/1.73 m2/min5. The incidence of fracture in patients with CKD G3 to G5D, and post‑transplant is two‑to 100‑fold higher, compared with age‑and sex‑matched individuals without CKD6. Studies have found that fracture rates in end‑stage renal disease (ESRD) are similar to the fracture incidence rate of non‑uremic individuals who are 10‑20 years old7,8. With aging, there is a physiological loss of nephrons, and subsequently a decrease in glomerular filtration rate (GFR). Furthermore, aging‑related vascular and renal disease may exacerbate the reduction in GFR3,9. Currently, we know that aging patients with CKD can present simultaneously with OP and ROD. This is a concern since the population will continue to age and there will be more overlapping of age‑linked and postmenopausal causes of bone loss with CKD‑specific causes of bone loss. The World Health
Organization defines OP as a T‑score ≤‑2.5, given by dual‑energy X‑ray absorptiometry (DXA). The National Institutes of Health defines OP as a skeletal disorder characterized by compromised bone strength predisposing to a higher risk of fracture. Bone strength reflects the integration of two main features: bone quantity and bone quality. Bone quantity is assessed by DXA, and bone quality is related to intrinsic biomechanical properties, such as remodelling defects, collagen crosslinking, and mineralization properties. In treatment studies, the improvement of bone mineral density (BMD) was small compared with fracture risk reduction, indicating that OP is more that only low BMD. This explains why fractures occur in patients with a T‑score non‑diagnostic of OP10,11.
In the earliest stages of CKD, identifying and treating OP could be effective in preventing fractures and reducing the burden of morbidity and mortality12. Fibroblast growth factor 23 (FGF‑23) is a phosphate‑regulating hormone, predominantly expressed in osteocytes, involved in the regulation of phosphate, vitamin D and parathyroid hormone13.
Alterations in FGF‑23 and its co‑receptor, Klotho protein, seem to be the earliest metabolic disturbance of mineral metabolism detectable in CKD13. Therefore, in CKD, early increments in FGF‑23 could be useful in identifying the timing of adaptation of bone to CKD, and therefore the establishment of renal osteodystrophy. Additionally, in early phases of CKD, significant reductions in BMD, diagnostic of OP, could be useful in identifying CKD patients at increased risk of fracture and who could benefit from early therapy. New drugs established for the treatment of OP directly regulate the activity of bone cells, and experience has been accumulating on the potential role of these compounds in CKD patients with OP. In addition to human recombinant PTH peptide 1-34 (teriparatide) and bisphosphonates, the new human monoclonal antibodies, denosumab and romosozumab, should be the focus of nephrologists, since they have been shown to increase BMD and decrease fracture rates in OP. The mechanisms of these drugs will be discussed later.
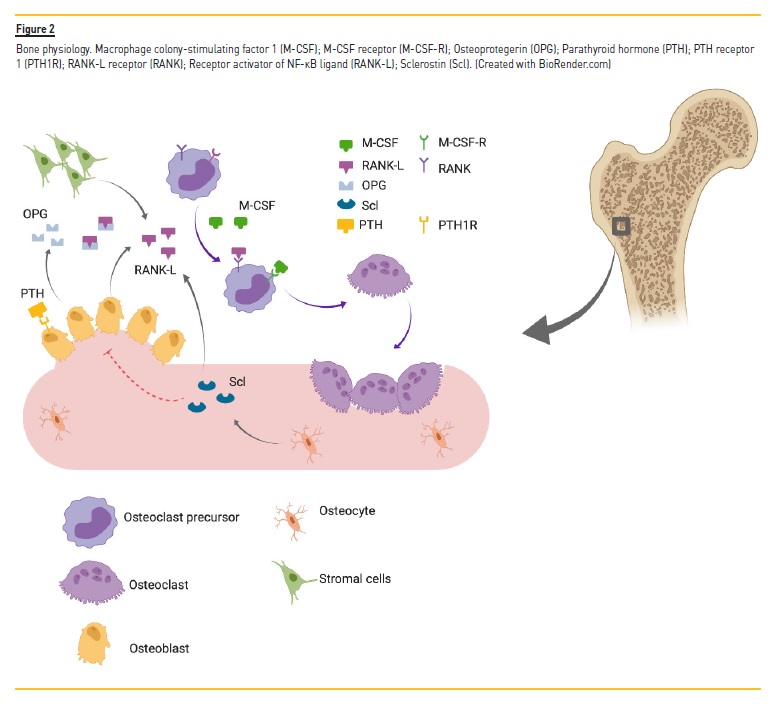
BONE PHYSIOLOGY AND CKD#8209;MBD
In terms of physiology, bone is continuously renewed through the coordinated process of bone resorption by osteoclasts and bone formation by osteoblasts (Figure 1). Hormones through paracrine and endocrine mechanisms rigorously regulate bone resorption and formation. Osteoclasts derive from the bone marrow macrophages, and express receptors for several cytokines, specifically the receptor activator of NF‑κB ligand (RANK‑L) and macrophage colony‑stimulating factor 1 (M‑CSF).
These cytokines are synthetized in the bone marrow by stromal cells and their derivative osteoblasts, and then bind to the respective receptors (RANK and M‑CSF‑R), promoting the differentiation of monocytes into mature osteoclasts14,15. Osteoblasts also synthetize osteoprotegerin (OPG), a high‑affinity inhibitor of RANK‑L, thus reducing RANK‑L/RANK ligation in osteoclasts precursor and pre‑osteoclasts16.
Osteocytes are also a key element in bone turnover regulation, since they synthetize sclerostin. Sclerostin is an anti‑anabolic protein that inhibits the Wnt pathway. The major role of this protein is to reduce osteoblastogenesis, promote osteoblast and osteocyte apoptosis17. Furthermore, sclerostin also stimulates osteoclastogenesis, by inducing RANK‑L synthesis. The RANK/RANK‑L/OPG axis and Wnt pathway are the major elements that are mainly responsible for the balance between bone resorption and bone formation, keeping the balance between bone resorption and bone formation bone remodelling. When both processes are unbalanced, pathologies arise. In OP, there is an imbalance towards bone resorption, which leads to loss of bone mass and consequently bone strength. In renal osteodystrophy, the pathophysiological mechanism is more complex, including changes in phosphate and calcium metabolism, as well as hormonal imbalances, involving vitamin D and parathyroid hormone3. PTH is typically increased in CKD, and induces maturation and activity of osteoblasts via the PTH receptor (PTH1R) present in these cells. Consequently, it leads to osteoclast activation, via RANK‑L formation. In turn, vitamin D synthesis is decreased in CKD. Vitamin D stimulates calcium resorption and osteoclast differentiation in bone, by a mechanism that involves a receptor on bone cells, vitamin D receptor (VDR). This mechanism is independent of the kidney and intestine. The different ROD subtypes are the result of the combination of several possible hormonal disorders that occur in CKD3.
MANAGEMENT OF KIDNEY‑INDUCED OSTEOPOROSIS: CHANGING PARADIGM
Treatment of ROD has focused on supressing high turnover with active vitamin D and/or calcimimetics. This approach has not been useful in reducing all‑type fracture rates. Therefore, a shift in management of CKD‑MBD is mandatory, in order to improve risk reduction of all‑type fractures. Back in 2003, the Kidney Disease Outcomes Quality Initiative guidelines did not recommended bone mineral density measurement in CKD patients, because there was a lack of studies proving the utility of a low BMD as a screening tool to identify patients at risk of fracture. In 2009, despite the emerging evidence proving the ability of low BMD to identify patients at risk, the 2009 KDIGO guidelines still did not recommend its routine use in CKD patients.
The consensus was that the risk of treating patients with drugs, such as bisphosphonates, was high and that the benefit was uncertain.
The 2017 KDIGO update in management of CKD‑MBD recommended DXA BMD testing, in patients with CKD G3a to G5D with evidence of CKD‑MBD and/or risk factors for OP to assess risk of fracture, if results will impact treatment decisions18. The purpose of this amendment is the growing evidence that DXA BMD predicts incident fractures in patients with CKD G3a‑G5D, and also might impact the decision of performing a bone biopsy.
Regarding the role of bone biopsy in management of ROD, the new update no longer recommends performing a bone biopsy before starting OP treatment in patients with CKD, low BMD and a high risk of fracture. It further states that it is reasonable to perform bone biopsy if knowledge of the type of ROD will impact treatment decision.
These modifications are the result of the lack of evidence demonstrating that antiresorptive agents induce adynamic bone disease and because of emerging studies showing that antiresorptive therapies are safe and effective in preventing fractures in patients with mild, moderate or severe renal impairment19,20. Although bone biopsy is the gold standard for diagnosis of ROD subtype and guides therapeutic decisions, it has many restrictions, such as cost, availability, time‑consuming, invasiveness and discomfort to the patient and it has never been proven to predict the risk of fracture.
The new update recommends monitoring serum levels of calcium, phosphate, PTH, and bone‑specific alkaline phosphatase activity beginning in CKD G3a, because markedly high or low values may reflect underlying bone turnover18. In the general population, patients undergoing antifracture therapy should be tested for BMD at intervals that range from 1 to 2 years. Although we lack evidence showing that improvement of BMD will translate into a reduction in fracture risk, identical intervals can be used in the population of CKD patients4.
Before initiating an anti‑resorptive or anabolic agent, we need to control the biochemical disorders that occur early in the development of chronic kidney disease, the prevalence of which increases with the worsening of renal function. These changes include vitamin D deficiency, hyperphosphatemia, and secondary hyperparathyroidism (SHPT). SHPT appears as an attempt to increase serum calcium levels, reduce serum phosphate levels, and correct vitamin D deficiency.
However, over the course of chronic kidney disease, these hormonal abnormalities become poorly adaptive, and should be corrected as part of addressing this spectrum of disease.
Regarding non‑pharmacological measures that are effective in preventing fractures, these should be used in all patients. These measures include smoking cessation, weight‑bearing exercise fall prevention, improved nutrition and moderation in alcohol consumption, and are responsible for a 60% reduction in fracture incidence, in the general population4.
BISPHOSPHONATES
Bisphosphonates are well established as safe and effective in the treatment and prevention of postmenopausal and glucocorticoid‑induced OP. Their role in decreasing osteoclastic activity is due to the inhibition of farnesyl pyrophosphate synthase, a vital enzyme in osteoclast function. Bisphosphonates have high affinity to hydroxyapatite; thus they are retained in the bone for many years. The fraction that is not retained in the bone is excreted in the kidney, via glomerular filtration and active secretion. Thus, there is potential to accumulate in patients with impaired renal function and produce greater suppression of bone remodelling and possibly impairing mineralization and bone strength. Impaired fracture healing, osteonecrosis of the jaw and adynamic bone disease (ABD) have been reported with bisphosphonate therapy21. ABD is a specific form of ROD, characterized by very low bone turnover and increased bone fragility, most likely to occur in patients with stage 4 and 5 CKD. For this reason, bisphosphonates were not recommended in patients with GFR< 30 ml/min.
Alendronate, and other bisphosphonates, have been shown to improve coronary artery calcification, intima‑media thickness at the carotid artery (CA‑IMT), brachial‑ankle pulse wave velocity (baPWV) and lipid profile (increasing HDL‑C and decreasing LDL‑C)22‑25. Miller et al analysed combined data from nine double‑blinded, controlled phase III trials, in order to understand the effect of renal insufficiency on the safety and efficacy of bisphosphonate treatment.
This analysis included osteoporotic women, who received placebo or risendronate 5 mg, daily for up to 3 years, and who had renal impairment, defined as creatinine clearance (CrCl) <80 ml/min, excluding patients with ESRD. Patients were categorized as having mild (CrCl 50 to < 80ml/min), moderate (CrCl 30 to 50 ml/min), or severe (CrCl < 30 ml/min). Risendronate significantly reduced the incidence of new vertebral fractures and increased BMD, within each renal impairment subgroup. Miller et al reported that there was no difference in the frequency of overall adverse events or renal‑related adverse effects, even in women with severe renal impairment. In relation to bone adverse effects, histomorphometric data from post‑treatment bone biopsies suggest that risedronate treatment was not associated with a deleterious effect on bone strength or mineralization. While most adynamic renal bone disease occurs in patients with G5 CKD, it can also occur in patients with G4 CKD; therefore, the authors advise performing a bone biopsy in order to exclude adynamic renal bone disease when a clinician has any concern that a patient may have this specific form of renal osteodystrophy19.
More recently, Shigematsu et al analysed the data from three Japanese risendronate phase III trials, in a population of 852 patients with OP, and GFR in a range of 30 to ≥ 90 ml/min/1.73 m2. This post hoc analysis showed a significant improvement in lumbar spine and significant suppression in the bone turnover markers. Similarly, there was no significant difference in the magnitude of the increase in lumbar spine BMD, among the subgroups (GFR ≥ 30 to < 60; ≥ 60 to < 90; ≥ 90 ml/min/1.73 m2). In addition, there was no difference between subgroups in the incidence of overall adverse events and kidney function‑related adverse events26.
In a randomized controlled trial, patients with CKD stages G3‑G4, receiving 70 mg of alendronate weekly, had an increase in lumbar spine BMD (T score difference, +0.3), compared with placebo matched individuals27. In an open‑label study, ibandronate was evaluated for the treatment of reduced bone density in G5D CKD patients, with low BMD (lumbar spine T‑score <‑1.0) and elevated PTH levels (twofold the upper limit of normal). This study showed a significant increase in BMD and decrease in bone turnover after 48 weeks of treatment, while PTH levels were maintained28.
DENOSUMAB
Denosumab (DMAb) is a fully human monoclonal antibody directed against RANK‑L, with high affinity and specificity. DMAb acts as an OPG mimicker, preventing the interaction with its receptor, RANK21.
This mechanism leads to suppression of osteoclast formation, activity and survival, decreasing bone resorption, and increasing bone density3,29.
Hypocalcemia is the most common adverse event found in patients treated with DMAb, particularly in stage 4 and 5 CKD patients.
DMAb strongly blocks bone resorption and reduces release of calcium from bone, which leads to hungry‑bone‑like syndrome, and consequently hypocalcemia21,30. The Fracture Reduction Evaluation of Denosumab in Osteoporosis Every 6 Months (FREEDOM) was a randomized, placebo‑controlled trial that randomly assigned 7868 postmenopausal women with OP (T‑score < ‑2.5) to receive either 60 mg of DMAb or placebo subcutaneously every 6 months, for 36 months.
Treatment with DMAb significantly reduced vertebral, hip and non‑vertebral fracture risks. There were no cases of osteonecrosis of the jaw or impaired fracture healing, unlike bisphosphonates29. Jamal et al examined the efficacy and safety of DMAb among participants in the FREEDOM study. They stratified patients by level of kidney function, and evaluated incident fracture rate, changes in BMD, serum calcium, and incident adverse events. 73 and 2817 women in this study had creatinine clearance between 15 and 29 ml/min and between 30 and 59 ml/min, respectively. There was no interaction between treatment effect and kidney function, and adverse effects did not differ by creatinine clearance. DMAb increased BMD at the spine and hip, and resulted in 68% lower odds of vertebral fracture in subjects with a GFR of 30‑59ml/min per 1.73 m231.
A 16‑week study from Block et al found that renal function did not have a significant effect on DMAb pharmacokinetics or pharmacodynamics, when administering a single 60 mg‑subcutaneous (sc) dose in subjects with renal function ranging from normal to G5D. These findings lead to the conclusion that DMAb does not require dose adjustment to glomerular filtration, making it a useful therapeutic approach for patients with high risk of fracture and impaired renal function30. Similarly to hungry bone syndrome in the context of parathyroidectomy, after the first dose of DMAb, patients with high‑turnover bone disease, have a quick reduction in their endogenous supply of calcium from bone, while deposition of mineral (calcium and phosphate) into new matrix remains increased. This explains why hypocalcemia is a common adverse effect (15%), especially in patients with severe CKD or ESRD, due to their great dependence on PTH‑induced bone resorption. As result of these findings, the authors strongly recommend supplementation with calcium and vitamin D in patients with severe CKD or ESRD, as necessary to maintain adequate serum levels30.
Denosumab for severe hyperparathyroidism in dialysis patients
Secondary hyperparathyroidism is one of the major obstacles in patients with ESRD, and affects most patients receiving dialysis. Treatment with calcitriol can decrease intact PTH (iPTH) levels and improve bone histology. However, because of the calcium and phosphate efflux from the bone in SHPT, hypercalcemia and hyperphosphatemia usually occur, which is a limitation to the management of these patients with calcitriol or other active vitamin D analogs32‑34.
Calcimimetic agents (cinacalcet and etecalcetide) that modulate the calcium‑sensing receptor have been also used as a pharmacological option for the treatment of SHPT with an additional beneficial effect on decreasing calcium and phosphate serum levels, but there is still a lack of a therapy that can compensate for the long‑term calcium and phosphate loss from bone in these patients21,35. Therefore, these patients often require a parathyroidectomy. The success of parathyroidectomy in increasing BMD is approximately 10% after 1 year36. Unluckily, many patients are poor surgical candidates because of their multiple comorbidities and functional status.
Chen et al conducted a 6‑month prospective clinical study in 12 patients with severe SHPT on dialysis to evaluate the efficacy and safety of DMAb. All patients had iPTH > 1000 pg/ml, low bone mass (T score < ‑1.0 SD), and bone pain, and were poor surgical candidates for parathyroidectomy. All patients received DMAb (60 mg), calcitriol, phosphate binders, and dialysate calcium that were adjusted according to the biochemistry. The BMD increased in both the femoral neck and lumbar spine after 6 months. Furthermore, a large increase of BMD was found in SHPT patients having high bone turnover compared to those having moderate bone turnover. In the first month, most patients had increased iPTH levels, which dramatically decreased after increasing the calcitriol dose. Therapy with sc DMAb allowed for a more aggressive use of calcitriol to control hyperparathyroidism, because of its efficacy in controlling hypercalcemia and hyperphosphatemia.
DMAb represents a potential bridge for patients on dialysis with SHPT and very low bone mass before parathyroidectomy to improve bone mass gain, reduce bone pain and possibly decrease the incidence of severity of hungry bone syndrome. It could also be a rescue therapy to control hyperparathyroidism in patients who are poor candidates for parathyroidectomy21.
Osteoporosis and vascular calcification frequently coexist, especially in CKD patients37. The triad cytokine system, RANK‑L/RANK/OPG, is a potential mediator of bone metabolism and vascular homeostasis37.
Helas S. et al analysed the effects of RANK‑L inhibition by DMAb, on vascular calcium deposition following glucocorticoid exposure.
DMAb reduced vascular calcium deposition in glucocorticoid‑induced OP in mice. Therefore, similar to bisphosphonates, the prevention of bone loss by denosumab might also be associated with reduced vascular calcification in certain conditions37,38.
More recently, Iseri K. et al conducted a prospective three‑center study of 48 hemodialysis (HD) patients with OP, who were randomized to either DMAb or intravenous alendronate. The authors evaluated and compared the efficacy and safety of these two agents regarding OP, mineral metabolism, coronary calcification, arteriosclerosis and vascular function. They excluded patients that had received anti‑osteoporotic agents in the preceding 6 months38. DMAb and alendronate markedly decreased serum levels of bone turnover markers and increased lumbar spine BMD at 12 months compared to baseline, with no significant differences between the two groups. The incidence of adverse events did not differ between the DMAb and alendronate groups. Although all patients were supplemented with calcium and calcitriol during the initial 2 weeks, one patient in the DMAb group developed severe hypocalcemia that required additional supplementation with calcium and vitamin D receptor activators. These findings corroborate the need for close monitoring of serum Ca, when prescribing DMAb. On the other hand, they could not demonstrate benefits on coronary calcification, arteriosclerosis and vascular function compared to pretreatment in both groups. Larger sample size and long‑term study period are required in order to evaluate such beneficial effects.
Safety and efficacy of denosumab in osteoporotic hemodialysed patients
Festuccia F. et al conducted a pilot study to evaluate the efficacy and tolerability of DMAb in 12 hemodialysed patients39. Quantitative ultrasound was used for bone evaluation for fracture risk assessment, diagnosis of OP, treatment initiation and treatment monitoring. The mean T‑score went from ‑5.33 to ‑4.84 at 24 months (total reduction of 10%). Additionally, there was a total reduction of the risk fracture of 72%, not statistically significant due to the small sample. These authors highlighted the safety and efficacy of DMAb in the treatment of OP in HD patients, potentially supporting its use to reduce the burden of fractures in this patient population39.
In conclusion, the risk of hypocalcemia in HD patients is not a contraindication to the use of DMAb, and benefits of the drug prevail over risk39. To date, DMAb is not indicated as first‑line therapy and its use is limited to patients intolerant or unresponsive to bisphosphonates3.
PARATHYROID HORMONE
Teriparatide in postmenopausal women with osteoporosis and mild or moderate renal impairment
Two biological PTH molecules are available for clinical use. One, the full‑length recombinant human PTH, is used in the treatment of patients with hypoparathyroidism3. The other one, the N‑term recombinant human PTH (teriparatide), is a recombinant peptide of the first 34 amino‑terminal residues of PTH. Teriparatide was the first Food and Drug Administration (FDA)‑approved osteoanabolic agent to treat OP and prevent fractures in both age‑related and glucocorticoid‑induced OP. PTH secretion is stimulated by decreases in serum ionized calcium, which in turn increases calcium reabsorption in the renal tubule and bone40. In addition, they stimulate the conversion of 25‑hydroxyvitamin D to 1,25‑dihydroxyvitamin D, thus increasing intestinal absorption. PTH1R is expressed in osteoblasts and stimulates its proliferation and activity; therefore an anabolic action is invariably attributed to PTH41,42. However, the promotion of osteoblast activity and number stimulates RANK‑L synthesis and activation of osteoclasts and reabsorption, thus balancing the two processes of bone formation and resorption. Intermittent secretion is anabolic, while chronic stable secretion is catabolic. Considering the short half‑life of teriparatide (1.2‑5h, depending on the level of renal impairment), its daily administration as a drug resembles a pulsatile secretion and, not surprisingly, resulted in anabolic effects with increments in the BMD in pre‑clinical and clinical studies. The stimulation of bone formation occurs earlier than bone resorption; therefore the rate of BMD increment is predictably higher in the first months of therapy and expected to plateau as osteoclasts also become recruited. The final balance will reset at a value a little bit higher. Hypercalcemia, hypercalciuria, hyperuricemia and hypotension are the most common short‑term adverse events, while osteosarcoma is a long‑term adverse event, found in rats. Miller P. et al, using data from a double‑blinded trial (Fracture Prevention Trial), explored the safety and efficacy of teriparatide in 1637 postmenopausal women with OP and various degrees of renal function (normal: GFR≥ 80 ml/min/1.73 m2; mildly impaired: GFR 50‑79 ml/min/1.73 m2; moderately impaired: GFR 30‑49ml/min/1.73 m2)43.
Patients were randomized to receive daily sc injections of placebo, teriparatide 20 mcg/day or teriparatide 40 mcg/day, with daily calcium (1000 mg) and vitamin D (400‑1200 U). Inclusion in the study required serum creatinine concentrations ≤ 2.0 mg/dl and normal serum PTH concentrations. Compared with patients with normal renal function, patients with renal impairment were older, shorter, weighed less, had been postmenopausal longer and had lower baseline lumbar and femoral neck BMD. Teriparatide (20 or 40 mcg) significantly increased lumbar spine BMD within each renal function subgroup, and femoral neck BMD only in subgroups of normal and mildly reduced GFR. In the same way, teriparatide effectively prevented vertebral and non‑vertebral fractures in patients with CrCl < 80 ml/min compared with > 80 ml/min. Regarding the adverse effects, teriparatide‑treated patients experienced an increased incidence of 4-6h postdose serum calcium > 10.6 mg/dl, in all renal function categories, in particular at lowest levels of creatinine clearance. However, teriparatide 20 mcg was not associated with significant increase of 4‑6h postdose serum calcium >11 mg/dl in any category of renal impairment. Increased incidence of hyperuricemia also occurred, which was greatest in patients with moderate renal impairment, and in those receiving teriparatide 40 mcg. However, there were no significant between‑group differences in the incidence of gout or arthralgia or of nephrolithiasis.
Limited data were available for patients with severe renal impairment.
Teriparatide in hemodialysis patients
Bone resistance to PTH is one of the first manifestations of ROD, in the early phases of renal failure. ABD is either caused by reduced PTH or downregulation of PTH receptors in osteoblasts44. In ABD there is a reduced PTH effect on osteoblasts. Therefore, some authors assumed that exogenous administration of PTH would abolish the relative or absolute PTH deficiency and stimulate bone formation. Besides decreased BMD, patients with ABD often suffer from hypercalcemia and hyperphosphatemia due to a reduced uptake of calcium and phosphate in bone. Hyperphosphatemia in turn induces transformation of vascular smooth muscle cells into osteoblast‑like cells. In the presence of hypercalcemia, the transformed cells then actively deposit calcium and phosphate into the vascular wall. This process appears to be predominant in ABD since the extent of vascular calcification is greater in low turnover than in normal or high turnover45.
Cejka D. et al administered 20 μg teriparatide daily for 6 months to seven ESRD hemodialysis patients with ABD (determined by bone biopsy or iPTH < 100 pg/ml). Serologic bone markers, BMD and coronary artery calcification were measured at baseline and after 6 months.
To avoid the development of osteomalacia, calcium‑phosphate binders and/or calcitriol were administered to all patients. Therapy with teriparatide improved the monthly change in BMD at both the spine BMD and the hip and did not affect changes in coronary artery calcification scores44. These data suggest that teriparatide might be osteoanabolic in ESRD patients with serum iPTH below the recommended levels. This supports the hypothesis of relative PTH deficiency in ABD and the possibility of overcoming this deficiency by exogenous administration of PTH. Despite all patients being treated with calcium‑based phosphate binders and/or calcitriol, significant changes in serum calcium levels were not found. Teriparatide treatment was found to significantly decrease serum phosphate levels. Decreasing serum phosphate levels have been suggested to protect arteries from pathological calcium phosphate deposition. Therefore, teriparatide therapy may ameliorate vascular calcification and improve mortality outcomes in EDRD patients. The mechanism behind the reduction in serum phosphate levels may be the stimulation of FGF‑23, which is known to reduce serum phosphate by supressing intestinal phosphate and proximal tubular phosphate reabsorption. In conclusion, patients with ESRD and ABD showed increases in lumbar BMD after treatment with teriparatide. Further studies are warranted to determine the impact of teriparatide treatment on bone metabolism, bone architecture and fracture incidence in patients with ESRD. Sumida et al administered 56.5‑μg teriparatide once‑weekly to 22 hemodialysis patients with hypoparathyroidism and low bone mass (T score ≤ ‑2.5 at the spine, hip or forearm or a T‑score between ‑2.5 and ‑1.0 with a prevalent fracture). Therapy with teriparatide significantly increased lumbar spine BMD at 48 weeks. Additionally, bone formation and resorption markers increased, serum calcium levels decreased, and bone‑specific phosphatase alkaline was positively associated with the 48‑week percentage in lumbar spine BMD. However, no changes in femoral BMD was found, thus confirming the site‑specific effects. Serum PTH levels increased at week 4 and remained higher up to week 24. However, discontinuation of treatment because of adverse events was frequently observed, with transient hypotension being the most common adverse effect. Careful monitoring for adverse events should be required.
Summarily, teriparatide could decrease fracture risk in patients with early to moderate CKD, as well as increase BMD of trabecular bone. Post‑menopausal women with mild CKD, low turnover and no biochemical evidence of SHPT are more likely to benefit from this effect. In addition, teriparatide could increase lumbar BMD in HD patients with low levels of PTH and hypothetical adynamic bone disease.
Theoretically, teriparatide is indicated in patients with low bone volume and turnover, without osteomalacia, and should be avoided in other types of ROD.
ROMOSOZUMAB
Inhibitor of Wnt Signaling: Sclerostin
Canonical Wnt signalling plays a crucial role in bone metabolism, as it stimulates osteoblast differentiation and proliferation. Sclerostin is a 23 kDa glycoprotein, product of the SOST gene, synthetized mainly in osteocytes that plays a major role in blocking osteoblast differentiation and function, via Wnt antagonism. In addition to inhibiting bone formation, sclerostin also increases RANK‑L expression in osteoblasts, and consequently stimulates bone resorption by osteoclasts46. In a murine knockout model, sclerostin deficiency was associated with high bone mass phenotypes, while low bone mass phenotypes were found in sclerostin overexpression47.
Therefore, inhibiting sclerostin via human monoclonal antibodies, romosozumab, could be a promising alternative therapy for kidney‑induced OP, as its use is not related to induction of low turnover bone disease4. Nonetheless, sclerostin effects are not limited to the bone compartment; therefore caution should be taken regarding the effects that targeting sclerostin may induce in other systems. This is particularly important in CKD‑MBD patients, where skeletal (renal osteodystrophy), hormonal (hyperparathyroidism) and vascular (calcification) changes may occur46. McLung et al showed a greater increase in BMD in patients treated 12 months with romosozumab, compared to alendronate and teriparatide48. In a phase 3 trial, the Fracture Study in Postmenopausal Women with Osteoporosis (FRAME) trial, 6390 postmenopausal osteoporotic women, receiving either romosozumab or placebo, were evaluated after 12 months of treatment. The romosozumab group had a significantly reduction of vertebral fracture risk and less clearly non‑vertebral fracture risk compared with the placebo group49.
Saag et al conducted a phase 3 trial, the ARCH trial, involving postmenopausal women with OP and a history of fracture. In this study, the risk of new vertebral fractures was 48% lower in the romosozumab‑followed‑by‑alendronate group (127 of 2047 patients) compared with the alendronate‑followed‑by‑alendronate group (243 of 2047). Furthermore, the risk of hip fractures was 38% lower in the former group (41 of 2046 patients), compared with the latter (66 of 2047 patients).
More importantly, this study showed an increase in cardiac ischemic and cerebrovascular events that have not been reported in previous studies50. In conclusion, romosozumab increases bone formation and decreases bone resorption, leading to a lower risk of vertebral and clinical fractures in postmenopausal women. This drug could be used in CKD patients, particularly in adynamic bone disease. However, there is a lack of studies regarding pharmacokinetics in patients with reduced GFR and a concern with the potential negative effect on vascular calcifications.
CONCLUSIONS
Over the last century, the development of technology has allowed a better comprehension of bone disease in CKD patients. We now know that CKD‑MBD is a true systemic disease with effects on the bone and cardiovascular system. Patient‑centric and individualized approach is the future in the field of CKD‑MBD management. Nephrologists should evaluate the benefit of administering one of the new anti‑osteoporotic agents used for the treatment of OP in the general population (teriparatide, denosumab and romosozumab). However, there is still a lack of studies showing skeletal and non‑skeletal safety and anti‑fracture efficacy of such anti‑reabsorptive and anabolic therapies in CKD patients. Therefore, there is a need for randomized controlled clinical trials in CKD patients, evaluating the efficacy and safety of these compounds on reducing fracture risk and also its effects on cardiovascular events. These changes in the management of CKD‑MCD will allow nephrologists to improve short and long‑term patient clinical outcomes.
FUTURE DIRECTIONS
In the "TMV" system, bone volume has not been used to define types of renal osteodystrophy. Patients can present with high, low or normal bone volume with each of the forms of renal osteodystrophy.
There is growing recognition of the importance of low bone density in the pathophysiology of fractures in the CKD population. We suggest considering OP, with high or low turnover, a form of renal osteodystrophy, or at least a major risk factor for fracture in CKD.
In the future, the therapeutic strategies for the treatment of CKD‑MBD should aim at the control of bone remodelling and at the same time target bone volume, bringing to clinical practice the current and new therapies for OP.
References
1. Ott SM. Renal Osteodystrophy‑Time for Common Nomenclature. Curr Osteoporos Rep. 2017;15(3):187‑93. [ Links ]
2. Cozzolino M, Pasquali M. Where is the link between mineral bone markers and cardiovascular disease in CKD? Clinical kidney journal. 2015;8(6):729‑31. [ Links ]
3. Tartaglione L, Pasquali M, Rotondi S, Muci ML, Covic A, Mazzaferro S. Positioning novel biological in CKD‑mineral and bone disorders. J Nephrol. 2017;30(5):689‑99. [ Links ]
4. Khairallah P, Nickolas TL. Management of Osteoporosis in CKD. Clin J Am Soc Nephrol. 2018;13(6):962‑9. [ Links ]
5. Malluche HH, Mawad HW, Monier‑Faugere MC. Renal osteodystrophy in the first decade of the new millennium: analysis of 630 bone biopsies in black and white patients. J Bone Miner Res. 2011;26(6):1368‑76. [ Links ]
6. Moe SM, Nickolas TL. Fractures in Patients with CKD: Time for Action. Clin J Am Soc Nephrol. 2016;11(11):1929‑31. [ Links ]
7. Jamal SA, Hayden JA, Beyene J. Low bone mineral density and fractures in long‑term hemodialysis patients: a meta‑analysis. Am J Kidney Dis. 2007;49(5):674‑81. [ Links ]
8. Nickolas TL, Leonard MB, Shane E. Chronic kidney disease and bone fracture: a growing concern. Kidney Int. 2008;74(6):721‑31. [ Links ]
9. Miller AP, Huff CM, Roubin GS. Vascular disease in the older adult. J Geriatr Cardiol. 2016;13(9):727‑32. [ Links ]
10. Turner CH. Biomechanics of bone: determinants of skeletal fragility and bone quality. Osteoporos Int. 2002;13(2):97‑104. [ Links ]
11. NIH Consensus Development Panel on Osteoporosis Prevention D, and Therapy. Osteoporosis prevention, diagnosis, and therapy. JAMA. 2001;285(6):785‑95. [ Links ]
12. West SL, Lok CE, Langsetmo L, Cheung AM, Szabo E, Pearce D, et al. Bone mineral density predicts fractures in chronic kidney disease. J Bone Miner Res. 2015;30(5):913‑9. [ Links ]
13. Mazzaferro S, Pasquali M, Pirro G, Rotondi S, Tartaglione L. The bone and the kidney. Arch Biochem Biophys. 2010;503(1):95‑102. [ Links ]
14. Suda T, Takahashi N, Udagawa N, Jimi E, Gillespie MT, Martin TJ. Modulation of osteoclast differentiation and function by the new members of the tumor necrosis factor receptor and ligand families. Endocr Rev. 1999;20(3):345‑57. [ Links ]
15. Pixley FJ, Stanley ER. CSF‑1 regulation of the wandering macrophage: complexity in action. Trends Cell Biol. 2004;14(11):628‑38. [ Links ]
16. Teitelbaum SL. Bone resorption by osteoclasts. Science. 2000;289(5484):1504‑8. [ Links ]
17. Li X, Zhang Y, Kang H, Liu W, Liu P, Zhang J, et al. Sclerostin binds to LRP5/6 and antagonizes canonical Wnt signaling. J Biol Chem. 2005;280(20):19883‑7. [ Links ]
18. Ketteler M, Block GA, Evenepoel P, Fukagawa M, Herzog CA, McCann L, et al. Executive summary of the 2017 KDIGO Chronic Kidney Disease‑Mineral and Bone Disorder (CKD‑MBD) Guideline Update: what's changed and why it matters. Kidney Int. 2017;92(1):26‑36. [ Links ]
19. Miller PD, Roux C, Boonen S, Barton IP, Dunlap LE, Burgio DE. Safety and efficacy of risedronate in patients with age‑related reduced renal function as estimated by the Cockcroft and Gault method: a pooled analysis of nine clinical trials. J Bone Miner Res. 2005;20(12):2105‑15. [ Links ]
20. KDIGO 2017 Clinical Practice Guideline Update for the Diagnosis, Evaluation, Prevention, and Treatment of Chronic Kidney Disease‑Mineral and Bone Disorder (CKD‑MBD). Kidney Int Suppl2011. 2017;7(1):1‑59. [ Links ]
21. Chen CL, Chen NC, Hsu CY, Chou KJ, Lee PT, Fang HC, et al. An open‑label, prospective pilot clinical study of denosumab for severe hyperparathyroidism in patients with low bone mass undergoing dialysis. J Clin Endocrinol Metab. 2014;99(7):2426‑32. [ Links ]
22. Ariyoshi T, Eishi K, Sakamoto I, Matsukuma S, Odate T. Effect of etidronic acid on arterial calcification in dialysis patients. Clin Drug Investig. 2006;26(4):215‑22. [ Links ]
23. Celiloglu M, Aydin Y, Balci P, Kolamaz T. The effect of alendronate sodium on carotid artery intima‑media thickness and lipid profile in women with postmenopausal osteoporosis. Menopause. 2009;16(4):689‑93. [ Links ]
24. Igase M, Kohara K, Tabara Y, Ohara M, Takita R, Ochi M, et al. Change in arterial stiffness associated with monthly bisphosphonate treatment in women with postmenopausal osteoporosis. Menopause. 2014;21(9):962‑6. [ Links ]
25. Okamoto K, Inaba M, Furumitsu Y, Ban A, Mori N, Yukioka K, et al. Beneficial effect of risedronate on arterial thickening and stiffening with a reciprocal relationship to its effect on bone mass in female osteoporosis patients: a longitudinal study. Life Sci. 2010;87(23‑26):686‑91. [ Links ]
26. Shigematsu T, Muraoka R, Sugimoto T, Nishizawa Y. Risedronate therapy in patients with mild‑to‑moderate chronic kidney disease with osteoporosis: post‑hoc analysis of data from the risedronate phase III clinical trials. BMC Nephrol. 2017;18(1):66. [ Links ]
27. Toussaint ND, Lau KK, Strauss BJ, Polkinghorne KR, Kerr PG. Effect of alendronate on vascular calcification in CKD stages 3 and 4: a pilot randomized controlled trial. Am J Kidney Dis. 2010;56(1):57‑68. [ Links ]
28. Bergner R, Henrich D, Hoffmann M, Schmidt‑Gayk H, Lenz T, Upperkamp M. Treatment of reduced bone density with ibandronate in dialysis patients. J Nephrol. 2008;21(4):510‑6. [ Links ]
29. Cummings SR, Martin JS, McClung MR, Siris ES, Eastell R, Reid IR, et al. Denosumab for Prevention of Fractures in Postmenopausal Women with Osteoporosis. N Engl J Med. 2009;361(8):756‑65. [ Links ]
30. Block GA, Bone HG, Fang L, Lee E, Padhi D. A single‑dose study of denosumab in patients with various degrees of renal impairment. J Bone Miner Res. 2012;27(7):1471‑9. [ Links ]
31. Jamal SA, Ljunggren O, Stehman‑Breen C, Cummings SR, McClung MR, Goemaere S, et al. Effects of denosumab on fracture and bone mineral density by level of kidney function. J Bone Miner Res. 2011;26(8):1829‑35. [ Links ]
32. Neves KR, Graciolli FG, dos Reis LM, Graciolli RG, Neves CL, Magalhaes AO, et al. Vascular calcification: contribution of parathyroid hormone in renal failure. Kidney Int. 2007;71(12):1262‑70. [ Links ]
33. Bleyer AJ, Burkart J, Piazza M, Russell G, Rohr M, Carr JJ. Changes in cardiovascular calcification after parathyroidectomy in patients with ESRD. Am J Kidney Dis. 2005;46(3):464‑9. [ Links ]
34. Andress DL, Norris KC, Coburn JW, Slatopolsky EA, Sherrard DJ. Intravenous calcitriol in the treatment of refractory osteitis fibrosa of chronic renal failure. N Engl J Med. 1989;321(5):274‑9. [ Links ]
35. Tsuruta Y, Okano K, Kikuchi K, Tsuruta Y, Akiba T, Nitta K. Effects of cinacalcet on bone mineral density and bone markers in hemodialysis patients with secondary hyperparathyroidism. Clin Exp Nephrol. 2013;17(1):120‑6. [ Links ]
36. Chou FF, Chen JB, Lee CH, Chen SH, Sheen‑Chen SM. Parathyroidectomy can improve bone mineral density in patients with symptomatic secondary hyperparathyroidism. Arch Surg. 2001;136(9):1064‑8. [ Links ]
37. Helas S, Goettsch C, Schoppet M, Zeitz U, Hempel U, Morawietz H, et al. Inhibition of receptor activator of NF‑kappaB> ligand by denosumab attenuates vascular calcium deposition in mice. Am J Pathol. 2009;175(2):473‑8. [ Links ]
38. Iseri K, Watanabe M, Yoshikawa H, Mitsui H, Endo T, Yamamoto Y, et al. Effects of Denosumab and Alendronate on Bone Health and Vascular Function in Hemodialysis Patients: A Randomized, Controlled Trial. J Bone Miner Res. 2019;34(6):1014‑24. [ Links ]
39. Festuccia F, Jafari MT, Moioli A, Fofi C, Barberi S, Amendola S, et al. Safety and efficacy of denosumab in osteoporotic hemodialysed patients. J Nephrol. 2017;30(2):271‑9. [ Links ]
40. Brown EM. Four‑parameter model of the sigmoidal relationship between parathyroid hormone release and extracellular calcium concentration in normal and abnormal parathyroid tissue. J Clin Endocrinol Metab. 1983;56(3):572‑81. [ Links ]
41. LUND B, SØRENSEN OH, LUND B, BISHOP JE, NORMAN AW. Stimulation of 1,25‑Dihydroxyvitamin D Production by Parathyroid Hormone and Hypocalcemia in Man*. The Journal of Clinical Endocrinology & Metabolism. 1980;50(3):480‑4. [ Links ]
42. Black DM, Greenspan SL, Ensrud KE, Palermo L, McGowan JA, Lang TF, et al. The Effects of Parathyroid Hormone and Alendronate Alone or in Combination in Postmenopausal Osteoporosis. N Engl J Med. 2003;349(13):1207‑15. [ Links ]
43. Miller PD, Schwartz EN, Chen P, Misurski DA, Krege JH. Teriparatide in postmenopausal women with osteoporosis and mild or moderate renal impairment. Osteoporos Int. 2007;18(1):59‑68. [ Links ]
44. Cejka D, Kodras K, Bader T, Haas M. Treatment of Hemodialysis‑Associated Adynamic Bone Disease with Teriparatide (PTH1‑34): A Pilot Study. Kidney Blood Press Res. 2010;33(3):221‑6. [ Links ]
45. London GM, Marty C, Marchais SJ, Guerin AP, Metivier F, de Vernejoul MC. Arterial calcifications and bone histomorphometry in end‑stage renal disease. J Am Soc Nephrol. 2004;15(7):1943‑51. [ Links ]
46. Brandenburg VM, Verhulst A, Babler A, D'Haese PC, Evenepoel P, Kaesler N. Sclerostin in chronic kidney disease‑mineral bone disorder think first before you block it! Nephrol Dial Transplant. 2019;34(3):408‑14. [ Links ]
47. Kramer I, Loots GG, Studer A, Keller H, Kneissel M. Parathyroid hormone (PTH)‑induced bone gain is blunted in SOST overexpressing and deficient mice. J Bone Miner Res. 2010;25(2):178‑89. [ Links ]
48. McClung MR, Grauer A, Boonen S, Bolognese MA, Brown JP, Diez‑Perez A, et al. Romosozumab in Postmenopausal Women with Low Bone Mineral Density. N Engl J Med. 2014;370(5):412‑20. [ Links ]
49. Cosman F, Crittenden DB, Adachi JD, Binkley N, Czerwinski E, Ferrari S, et al. Romosozumab Treatment in Postmenopausal Women with Osteoporosis. N Engl J Med. 2016;375(16):1532‑43. [ Links ]
50. Saag KG, Petersen J, Brandi ML, Karaplis AC, Lorentzon M, Thomas T, et al. Romosozumab or Alendronate for Fracture Prevention in Women with Osteoporosis. N Engl J Med. 2017;377(15):1417‑27. [ Links ]
Ana Beatriz de Oliveira Pereira
E‑mail: beatrizpereira@live.com.pt
Disclosure of potential conflicts of interest: none declared
Received for publication: Dec 9, 2019
Accepted in revised form: Mar 25, 2020


{kind=link}