











 Português (pdf)
Português (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
INTRODUCTION
Food allergies are the main cause of anaphylaxis in children1,2. Cow’s milk is the main trigger, followed by egg3, which affects 1-2% of children4.
The current strategy regarding immunoglobulin E (IgE) mediated food allergies is allergen avoidance, symptom recognition in case of allergic reaction, and the administration of injectable adrenaline when needed1,3-8.
Oral immunotherapy (OIT) has shown promising results. This involves the regular administration of small amounts of the allergen that are progressively increased to a maximum tolerated dose. The aim is to desensitize patients, i.e., to achieve a state of food tolerance while the allergen is administered on a regular basis and, if possible, to achieve a state of sustained food tolerance after the end of immunotherapy(6-8). Since young children have a high likelihood of developing spontaneous tolerance2,5-7 the right time to start OIT may be around 4-5 years of age7.
So far, there are no standardized OIT protocols for allergy to egg white. Therefore, after reviewing the recent advances on OIT, the authors decided to create an original and careful protocol to apply to their patients. Its aim was to achieve the ingestion of an entire egg, without adverse reaction, with the use of pasteurized egg white (PEW) (allergenicity equivalent to a natural raw egg)(8 over eight medical visits, which took place two weeks apart and were carried out in the outpatient department (Table 1). During each visit there was a progressive increase in the amount of PEW offered to the children, and between visits a daily maintenance dose was administered at home. In the last visit, the children ingested a total amount of PEW that roughly corresponds to the amount of egg white of an entire egg (15ml + 15ml of PEW = 40g of egg white). Finally, the next day, desensitization was confirmed with the ingestion of an entire boiled egg under medical supervision. Upon conclusion of the protocol, children may ingest egg ad libitum but must keep the ingestion of an entire egg (cooked or raw) on alternate days.
Table 1 Egg white oral tolerance induction protocol. Each visit takes place two weeks apart with the exception of visit 9 that happens the next day after visit number 8.
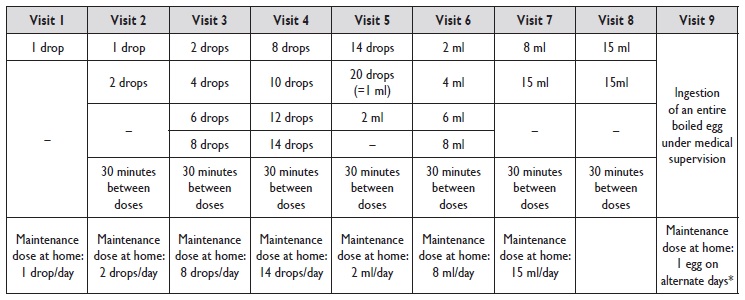
*At home children must eat an egg on alternate days; if more than 48 hours pass between egg ingestions, children must go to the day hospital to ingest an egg under medical supervision.
The procedure was approved by the hospital ethics committee. An informed consent was obtained from the children’s parents. Parents and their children were taught to recognize any symptoms of an allergic reaction and to administer adrenaline immediately, if needed.
CLINICAL CASES
Three children with persistent IgE mediated egg white allergy, with history of anaphylaxis, were submitted to the protocol (patients’ characterization is summarized in Table 2). All tolerated egg yolk. If present, asthma was well controlled. Their food allergy diagnosis was based on clinical history, skin prick tests (SPT), serum specific IgE levels and oral food challenges (with boiled egg). SPT were performed according to the European Academy of Allergy and Clinical Immunology recommendations, on the forearm with commercial extracts and a synthetic lancet. A negative (saline 0,9%) and a positive (histamine 10mg/mL) control tests were used. SPT were considered positive if a ≥ 3mm wheal diameter was reported after 15 minutes. Serum specific IgE levels to egg white were determined by an immunoenzymatic assay (UniCAPFEIA), and results were expressed in KU/L, positive cutoff ≥ 0,35KU/L. Two children completed the protocol with success (results are described in Table 2).
Table 2 Patients’ characterization (age of egg allergy diagnosis, clinical presentation, allergological assessment and accidental exposures) and oral tolerance induction protocol to egg white results.
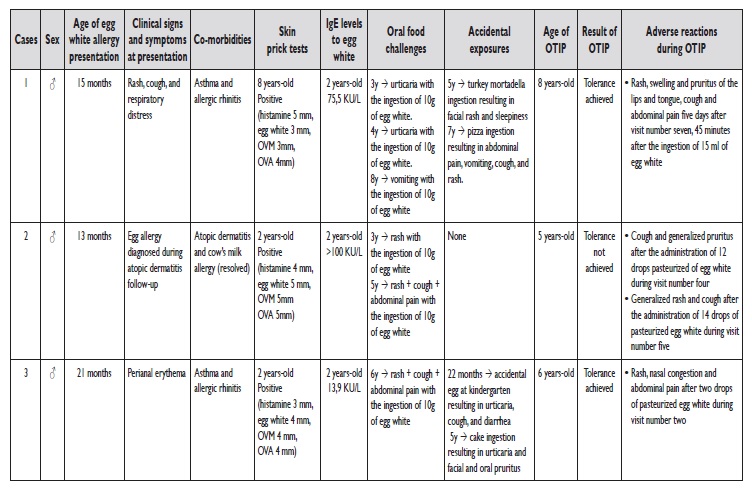
OTIP - oral tolerance induction protocol; OVA - ovalbumin; OVM - ovomucoid
The first child who initiated the protocol was an eightyear-old male. He had an anaphylactic reaction at home, 45 minutes after 15 ml of PEW five days after visit number seven, and adrenaline was administered. No triggering factor such as exercise, non-steroidal anti-inflammatory drugs intake or infection was identified. At this point, the protocol was readjusted. The maintenance dose of the PEW he was ingesting at home was reduced to 10 ml. On his eighth visit, he ingested 10 ml, followed by 15 ml with tolerance, so he kept 15 ml at home. At the ninth visit he ingested 15 ml plus 15 ml, 30 minutes apart, without eliciting symptoms and so, the next day, he ingested a boiled egg under medical supervision, without any complication.
The second child was a five-year-old male but, unfortunately, the protocol had to be stoped following two anaphylactic reactions. The first one occurred on the fourth visit, after the administration of 12 drops of PEW. The protocol was adapted and he kept a daily dose of 10 drops per day at home. On his adapted fifth visit, he started with the 10 drops that he was tolerating at home, followed by 12 drops that he also ingested without any symptoms. However, on this same medical visit, he had another anaphylactic reaction with the administration of 14 drops of PEW, so the protocol was interrupted.
The third child was a six-year-old male. He had an anaphylactic reaction during his second visit, after two drops of PEW, and adrenaline was used. The protocol was adapted, and the child went home with a maintenance dose of one drop of PEW per day. On his third visit, the administered doses were as referred in Table 1 for visit number 2. Since there were no more symptoms, the protocol followed as planned from that point forward and tolerance to egg was successfully achieved.
The two children that completed the protocol with success currently maintain egg ingestion as pleased, with the mandatory ingestion of an entire egg (either cooked or raw) on alternate days, without any other complications so far. They both concluded the protocol three years ago. The protocol had to be extended by two weeks for the two children that completed it. All children had at least one anaphylactic reaction during the protocol.
DISCUSSION
So far, avoidance diets are the only approved therapeutic option for food allergies6. Although apparently simple, these diets may have various implications for the quality of life of patients. There is therefore interest in novel strategies that allow the possibility of food tolerance(7). OIT, although logistically demanding and timeconsuming, has been tested and satisfactory results have been reported1,3-6,9.
According to the Cochrane review on OIT for egg white, that included 10 studies, 45% of the children receiving OIT were able to tolerate a full serving of egg compared to 10% of the control group(6). However, the existing studies involve small sample sizes, adverse allergic reactions occur in virtually all participants treated, and the evidence quality is low6. The egg OIT protocols differ in several aspects: egg preparation; place where the amount of egg preparation is increased (home versus day unit); dose escalation and duration of OIT to achieve desensitization (2.5 to 22 months)6. More recently, Martin-Muñoz et al.9 desensitized 81% of the patients submitted to their OIT protocol9.
In the protocol we present, the amount of PEW was always increased in the outpatient department, which, in the authors’ opinion, confers greater safety to the procedure.
However, it is not risk-free. All children experienced anaphylaxis, one of them even experienced an anaphylactic reaction with the maintenance dose at home. The authors
could not identify any potential triggering factor to explain this reaction. Adverse reactions in children undergoing food specific immunotherapy are not rare6-8. Most of them are mild and self-limited, however, more serious adverse reactions may occur7,8). It is extremely important that parents understand the risks of the protocol and are taught to recognize any symptoms suggestive of an anaphylactic reaction so that they can act quickly and accordingly.
This protocol was expected to last 105 days, but it was prolonged due to adverse reactions. The optimal duration of immunotherapy to achieve desensitization has not been established6,7. Faster protocols have been associated with more frequent and severe adverse reactions, while slower protocols could reduce treatment adherence1,9. The fact that all of the children submitted to our protocol presented anaphylaxis, leads us to question whether further adjustments to the protocol should be made, including more gradual increases in the doses of PEW offered to children.
Although sustained tolerance has not been assessed, the fact that these children were desensitized to egg white, even if it involves its regular intake is, in itself, beneficial for patients and their caregivers.
It is not clear whether the results are due to a desensitization state, or to a sustained tolerance state3. Some studies seeking to assess the induction of a sustained tolerance through OIT have shown that its effects may persist over time3,5,10. Martin-Muñoz et al.10 observed that one year of OIT with at least 6 months maintenance and dose equivalent to one pasteurized egg white improved the effectiveness of the egg OIT and allowed ad libitum egg consumption.
They also concluded that two egg serving per week ensures the persistence of total desensitization in most patients 6 months after ending a year of OIT10.
This study has some limitations, namely its small sample, which makes it difficult to generalize the results and no control group was included.
Although questions concerning its safety and its potential for developing long-term immunological tolerance remain, OIT is a promising therapy for food allergies. The induction of oral tolerance to egg white allows a less restrictive diet and greater safety preventing anaphylaxis, improving the quality of life of patients and their caregivers. The development of standardized protocols would help to incorporate desensitization into general clinical practice.

