











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
Introduction
The COVID-19 pandemic, caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), exposed global health systems to critical challenges in terms of preventing infections and ensuring effective strategies to protect public health (Legido-Quigle et al., 2020; World Health Organization, 2020). The severity of infection, with the associated risk of death, and the social isolation and socioeconomic insecurity resulting from lockdown measures led the global population to fear for and worry about both their personal safety and the future (Holmes et al., 2020; Hossain et al., 2020; Nicola et al., 2020). In the general population, the COVID-19 pandemic has been shown to be associated with an increased susceptibility to adverse mental health (MH) events in both individuals with a prior history of psychiatric disorders and those who had never previously suffered from MH issues (Lei et al., 2020). Furthermore, the persistent stress due to the risk of contracting the infection, the disruption of normal life as a result of government-imposed lockdown measures, and the conversion of health facilities into COVID-19 centres has resulted in shortcomings in the management of chronic health conditions and an increased risk of mental illness (Holmes et al., 2020; Nicola et al., 2020).
In Italy, at the beginning of the pandemic, more than 60 million people were subjected to lockdown measures in the effort to stop the spread of COVID-19; on 21 March 2020, all non-essential businesses and industries were closed, and citizens were told not to leave their homes without a documented reason (“phase one” of the Italian lockdown). In the subsequent phase two, between the end of May and 4 July, restrictions began to be eased, and freedom of movement across regions and to other European countries was restored.
One of the first surveys of the psychological impact of the COVID-19 pandemic on the general population of Italy revealed that an anxious temperament was a predictor for mild psychological distress during phase one of lockdown (Moccia et al., 2020). Another early survey, the COVID Mental Health Trial (COMET) (Fiorillo et al., 2020), investigating a large sample of Italians during phase one, found that 12.4% of the study participants reported severe or extremely severe depressive symptoms, 17.6% anxiety symptoms, and 41.6% felt at least moderately stressed. Females were twice as likely to be affected as males, while other risk factors for depression, anxiety and stress symptoms were: existing MH issues, having been infected by COVID-19, and a pre-existing physical disease. Social isolation and feelings of loneliness have also been cited as relevant risk factors for MH issues in relation to COVID-19 (Ciaramella et al., 2021; Giallonardo et al., 2020). While the above-mentioned studies demonstrated associations between psychosocial variables and MH in the general population during phase one, very few investigations into phase two of the COVID-19 lockdown in Italy have been published (Capuzzi et al., 2021). Therefore, there is scarce evidence on the associations between the various demographic, socioeconomic, biological/clinical history and perceived risk, general health and quality of life appraisals, worry, interference of COVID-19 in life, life satisfaction, perceived happiness and MH in the opening-up phase (Fiorillo et al., 2020; Moccia et al., 2020). According with the 2001 definition of MH by the World Health Organization (WHO), it should be emphasized that in a general population survey, it is necessary to investigate protective psychosocial dimensions as well as risk factors, because MH risk could be counterbalanced by protective factors such as adaptive coping skills, resilience, wellbeing and a strong support network (Giallonardo et al., 2020).
Hence, the aim of this study was to investigate the role of demographic (i.e., age, sex, marital status, education, composition of the household), medical/clinical history (i.e., being infected by COVID-19 or cohabiting with individuals infected by COVID-19, being at risk of COVID-19 in the family or having friends infected by COVID-19, having a chronic disease or pain), socioeconomic (i.e., current employment, family income contribution, family income changes, monthly expenses, occupation, job change, hours of daily work), and psychological factors (i.e., perceived risk of contracting COVID-19, perception of COVID-19 severity, worry and life interference, life satisfaction, perception of happiness, general health and quality of life appraisals) in MH and its dimensions (i.e. sadness, demoralization, nervousness, loss of calm) during phase two of the COVID-19 lockdown in Italy, when restrictions began to be eased.
Methods
Participants
A total of 300 adults responded to an online survey, which included questions about demographic, medical/clinical history, socioeconomic, psychological factors during phase two of the COVID-19 lockdown in Italy. Of those, only 195 completed it, responding to the section on mental health, and were therefore included in this study. The inclusion criteria for participation in the study were: (1) living in Italy during phase two of lockdown; (2) being 18 years or older; (3) being able to read and write in Italian; (4) having access to the internet; and (5) providing informed consent.
Procedure
The research was conducted in accordance with the Declaration of Helsinki ethical principles for research involving human subjects. Participants were asked to respond to an anonymous online survey, and to provide informed consent; the survey included an introductory section describing the aims of the study and asking for consent before proceeding. Participants could interrupt the survey at any point, without having to provide an explanation.
The survey was distributed across northern and central Italy via an online survey platform using a link disseminated through social media, with non-sponsored ads on Facebook and Instagram.
Responses were collected from 26 May to 4 July 2020, and pertain to the Italian sample from a multicentre investigation approved by the ISPA Research Center - Instituto Universitário ethics committee (ref. I/033/04/2020).
Variables and measures
Sample characteristics. Participants were asked to provide information on the following variables:
Sociodemographic: age, sex, marital status, education, household composition.
Socioeconomic: current employment, family income contribution, family income changes, monthly expenses, occupation, job change, hours of daily work.
Biological/Clinical history: whether they had had COVID-19, the risk of COVID-19 in the family, if they were cohabiting with those infected by COVID-19, having friends infected by COVID-19, having a chronic disease (and if so, what type of disease), having chronic pain (according the International Association of Study of Pain 2020 criteria) (Raja et al., 2020), and if so, pain duration, pain intensity and pain relief medication.
Psychological: items on perception of risk of contracting COVID 19, interference of COVID on life, worry, life satisfaction and perceived happiness, as well as mental health, as described below.
COVID-19 Risk perception. We used three questions to measure participants’ perceived risk of COVID-19. Specifically, they had to respond to: (1) Perceived severity of COVID-19; (2) Perceived risk of infection; and (3) Trust in the National Health System to handle the pandemic. Respondents were asked to rate their own perceptions on the following items:
On a scale of 0 to 10, on which 0 means “Not serious at all” and 10 means “Very serious”, how would you rate the disease COVID-19?
Indicate, on a scale from 0 to 10, on which 0 indicates “No risk” and 10 indicates “High risk”, how would you rate your risk of getting COVID-19?
How much confidence do you have in the national health system to deal with the COVID-19 pandemic? 0=no confidence; 5=total confidence.
Interference with life. Another section (developed ad hoc for this study) investigated interference from the COVID-19 lockdown. Participants were asked to indicate how much the COVID-19 situation had interfered with the following: their life in general; interpersonal relationships; work activity in general; productivity and motivation to work; satisfaction with life in general; and happiness. They were asked to rate this interference on a scale of 0 to 10, on which 0=“no interference at all” and 10=“total interference”.
In addition, participants were asked whether they adhered to social isolation measures, the reasons for their social isolation, and the number of times they left the house per week.
Worry. Participants were also asked to respond to questions (developed ad hoc for this study) on their level of concern. Specifically, they were asked to rate “How worried do you feel?”, as well as their concerns regarding their health, food, job, rent/mortgage, fixed costs, income, children’s education, relationships, supporting others, being supported, and the future, on a scale of 0 to 10, on which 0 corresponded to “not worried at all” and 10 “extremely worried” (for details see Appendix 1).
Life satisfaction and perceived happiness. Respondents were asked to score their life satisfaction on an 11-point numerical rating scale from 0=“totally unsatisfied” to 10=“totally satisfied”. As for their perception of unhappiness, this was measured on a 4-point Likert-type scale (from 1=very happy to 4=unhappy).
General health and quality of life appraisals. The survey also included two items assessing the appraisal of health and quality of life (QoL) in the preceding weeks on a scale of 1 to 5, with the highest score (5) corresponding to poor, and the lowest score (1) to excellent, as detailed in the Appendix 1. These two items are extrapolated in the World Values Survey (http://www.worldvaluessurvey.org/)
Mental health. The Mental Health Inventory-5 (MHI-5) section of the Italian version of the SF-36 Health Survey (SF-36) (Apolone & Mosconi, 1998; Strand et al., 2003), was used as a measure of mental health. The MHI-5 has five items, specifically: How much of the time during the last 4 weeks, have you: (1) Been a very nervous person? (2) Felt so down in the dumps that nothing could cheer you up? (3) Felt calm and peaceful? (4) Felt downhearted and blue? and (5). Been a happy person? Each item has six possible responses (from 1 “all of the time” to 6 “at no time”). The total MHI-5 score ranges from 5 to 30, and is transformed via standard linear transformation into a variable ranging from 0-100, with a score of 100 representing optimal mental health (Thorsen et al., 2013). The MHI-5 has shown good reliability (Cronbach’s alpha=0.82) and good validity for psychopathology with the SCL-25 as a comparison scale (Strand et al., 2003). In our study, the Cronbach’s alpha of the MHI-5 was 0.82.
Statistical analysis
Data was analysed using IBM SPSS Statistics version 21 (IBM Corp. Released, 2012). After application of the Kolmogorov-Smirnov test - which gives details about the Gaussian distribution of the data - we computed descriptive statistics (means and standard deviations for continuous variables and numbers and percentages for dichotomous variables) to describe the participant sample and the study variables. Several categorical variables (i.e., education, unhappiness, appraisals) were transformed into dummy variables to perform Pearson correlation analyses and t-test analysis.
Since the worry and interference dimensions were composed of numerous variables, a factorial analysis was performed to search for latent variables through the Varimax extraction with Kaiser’s normalization; two factors for the “worry” dimension were identified: Sustenance (variables pertaining to worry about food, work, mortgage, fixed costs, income and future) and Family Wellbeing (concerns about health, food, children’s education, relationship, supporting others, and being supported). These two factors included “worry” variables whose factor saturation in the factorial analysis was found to be significant (>.40). In this study, both factors showed good to excellent internal consistency (Family Wellbeing factor: Cronbach’s α=.83; Sustenance factor: Cronbach’s α=.91). As with the “worry” variables, a factorial analysis was performed on the “interference” item responses. This identified only one factor, Interference (details in Appendix 1), which demonstrated acceptable internal consistency with Cronbach’s α=.86.
To examine the association of MH with sociodemographic variables, a t-test analysis was performed to study sex differences in responses to the MHI-5 items and total score. A Pearson bivariate correlation was also performed on the MHI-5 total score and age, and each of the items that showed statistical significance, set at p<0.05.
Relationships between MH and demographic, medical/clinical history, socioeconomic and psychological variables were investigated using partial correlation analysis, controlling for sex and age.
In order to evaluate the strength of the associations between MHI-5 score and all the variables explored, a hierarchical multiple regression analysis was performed, extracting only those statistically significant and with an r at least >.30 in the partial correlation, expressing at least moderate effect size (Cohen, 1988).
Results
Participants
Of the 300 subjects that responded to survey only 195 completed it by replying to the section dedicated to MH. Subjects who completed the MH section were older (t=5.27, p=.000), with a higher degree of education (t=5.28, p=.000), with a higher prevalence of married people (χ 2 =16.12; p=.001), who together with their partner, were responsible for the family income (χ 2 =26.43; p=.000) compared to subjects who did not complete the MH section. No other sociodemographic and economic differences we have found between the two groups.
Detailed information on the 195 subjects who responded to the MH section is provided in Appendix 1, which includes all variables explored. Appendix 1 replaced data availability.
Associations between sociodemographic variables and perceived mental health during phase two of the lockdown in Italy
There were strong and statistically significant associations between age and mental health, positive for items 1, 2 and 4 and total MHI-5 score (r=.79, p<.001; r=.85, p<.001; r=.81, p<.001; r=0.15, p=.03 respectively), and negative for items 3 and 5 (r=-.79 and r=-.81, respectively; ps<.001). The t-test revealed no differences in mental health in relation to sex. Education also showed a moderately significant positive association with MH (see Table 1).
Table 1 Partial correlations of sociodemographic and medical variables with MHI-5 dimensions in 195 Italian subjects (controlling for age and sex)
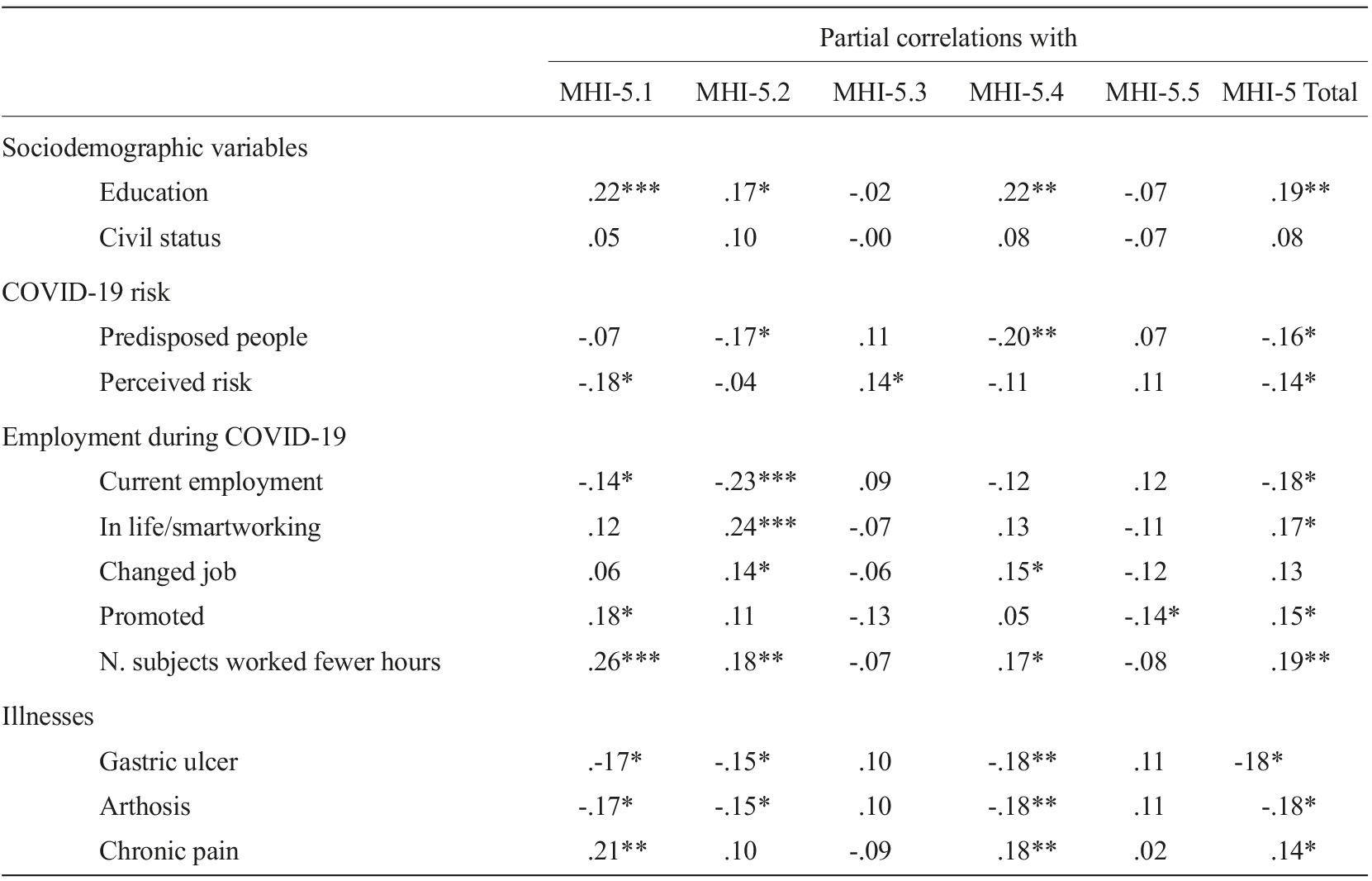
Note. MHI-5: Mental Health Inventory-5; it has been select variables which partial correlations reached at least one statistical significance; *p<.05; **p<.01; ***p<.001.
There was a statistical relationship between current employment status and MH scores. In particular, significant negative correlations between nervous (MHI-5.1) and sad (MHI-5.2) MHI-5 items were found with current employment. Subjects who continued to work at their place of occupation during the COVID-19 outbreak reported better MH than those who worked from home (Table 1). However, all correlation coefficients <.30, were indicative of a low effect size.
Associations between biological/clinical history variables and perceived mental health
Table 1 shows the relationships between the presence of a chronic disease and MH during phase two of the COVID-19 lockdown. Participants with gastric ulcer, arthrosis and chronic pain had worst MH. The “nervous” and “sad” MHI-5 items were associated with illness and expression of greater suffering, related to anxious and depressed mood. Nevertheless, as with the sociodemographic variables, correlation coefficients showed weak associations with low effect size between medical factors and MH.
Associations between psychological variables and perceived mental health
As reported in Table 2, the psychological dimensions, rather than the socioeconomic ones, had a greater impact on MH, and the correlations were stronger, reaching values of >.50. Life satisfaction turned out to be the dimension most positively related to MH. All of these correlations exceeded .30, with all MHI-5 items reaching the value of .30.
Table 2 Partial correlations between MHI-5 items and psychosocial factors during COVID-19 outbreak (controlling for age and sex)
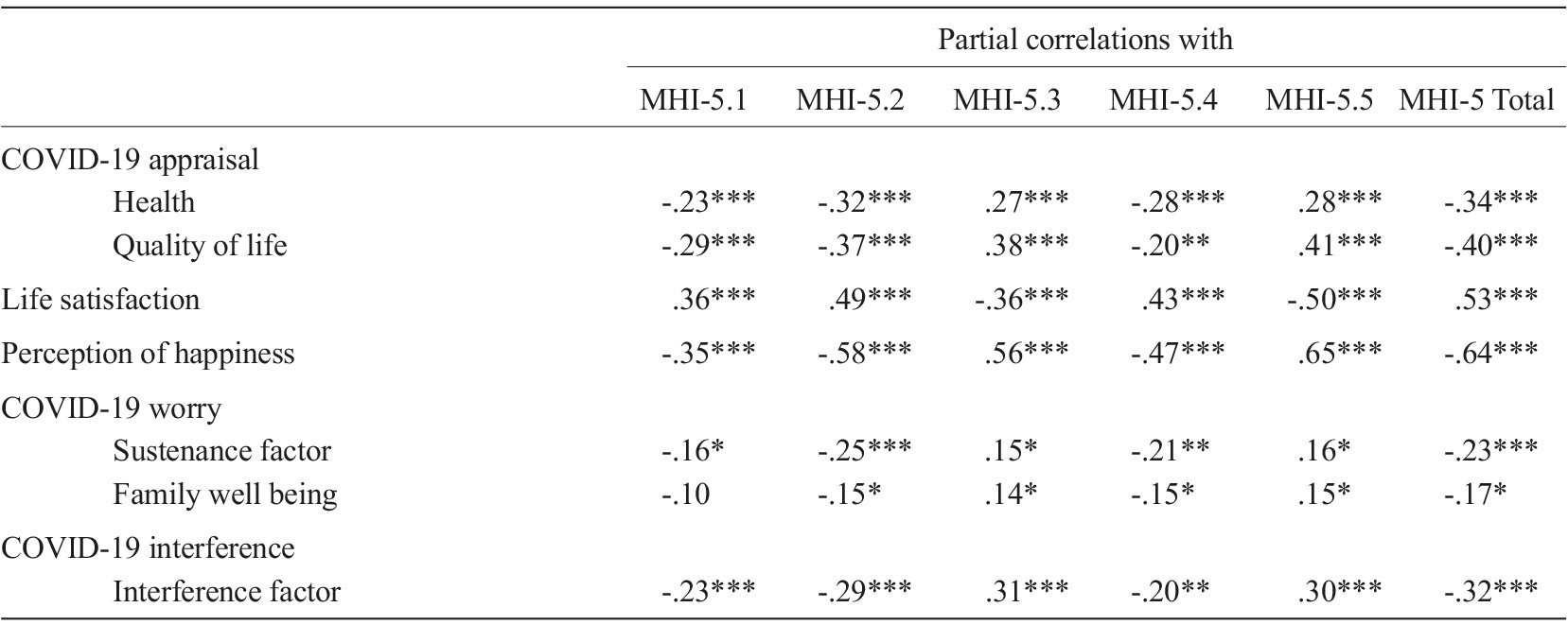
Note. MHI-5: Mental Health Inventory-5; it has been selected variables which partial correlations reached at least one significance; *p<.05**p<.01; ***p<.001.
Negative correlations were revealed between MHI-5 items, total score, and health and quality of life appraisals (QoL) (Table 2). In addition, the latent variables extracted from “worry” dimensions via factorial analysis demonstrated a negative correlation with items 1, 2, and 4 and MHI-5 global score. Therefore, worry about household finances, as opposed to the real socioeconomic variations due to national COVID-19 restrictions, seemed to be negatively associated with MH.
As regards the “interference” of the COVID-19 lockdown, this was found to be negatively and strongly correlated with MH. Greater Interference scores indicated that the COVID-19 national restrictions which interfered with life, relationships, work, motivation to work, life satisfaction and happiness were associated with worse MH. A negative correlation with happiness was also demonstrated by negative correlations between MHI-5 items 1 (nervous), 2 (sad), 4 (demoralised) and MHI-5 total scores and perceived happiness dimensions, as shown in Table 2.
Finally, a hierarchical regression analysis was used to study the contribution of the psychological variables in the levels of MH. This showed that the perception of unhappiness, poor life satisfaction and, to a lesser extent, worry about household income during phase two of the COVID-19 lockdown in Italy were associated with poor MH when corrected for age and sex (Table 3).
Table 3 Hierarchical regression analysis explaining mental health
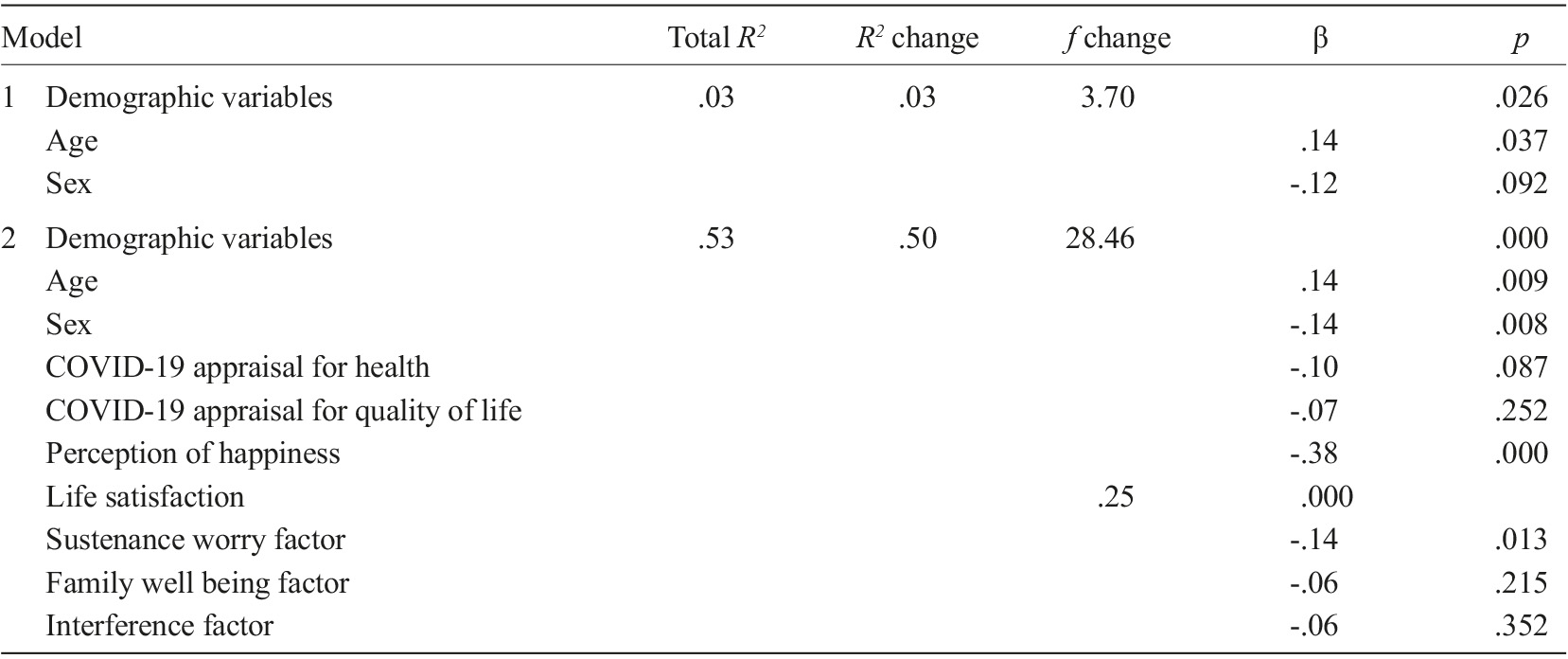
Note. Factor analysis: Sustenance worry factor (food+work+mortgage+fixed cost+income+future); Family well being factor (health+food+children education+relationship+support others+being supported+other); Interference factor (life in general+relationships+work+motivation to work+life satisfaction+happiness).
Discussion
The aim of this study was to investigate the association of demographic, medical/clinical history, socioeconomic, and psychological factors with MH and its dimensions during COVID lockdown easing in Italy. It revealed two emergent dimensions associated with MH, namely life satisfaction and perception of happiness. Often, in conditions of mental distress, scholars focus their attention on the search for pathological conditions and/or the presence of symptoms, focusing on negative mood and state of mind, while ignoring or forgetting that the loss of happiness and good mood and lack of satisfaction can by themselves contribute to mental distress (Kogler et al., 2015; Visser et al., 2017).
Positive appraisals seem to contribute to homeostasis, representing a signal indicating to the body to return to equilibrium (Burgdorf & Panksepp, 2006). Positive appraisal, a domain covering happiness and life satisfaction, is associated with success across life domains, including social, occupational, physical and psychological health (Wang et al., 2021). Positive appraisals seem to build the physical, intellectual and social capacity to promote long-term survival (Alexander et al., 2021). Hence, a state of wellbeing being undermined by events such as the COVID-19 lockdown can compromise mental and physical homeostasis, which is expressed as a loss of MH. From a homeostatic and biopsychosocial perspective of MH, it appears from our results that life satisfaction and perceived happiness represent important mental resources for counteracting the effects of lockdown on MH.
Correcting for age and sex, we also found that a negative appraisal of health and QoL were associated with worse MH during phase two of COVID-19 lockdown in Italy. With a moderate-high effect size, our study demonstrates a strong correlation between the perceived loss of wellbeing (positive appraisal and health/QoL) and mental health risk. It is important to note, however, that the perceived MH risk was not correlated with the real level of poverty, as demonstrated by weak correlations between socioeconomic factors and MH.
Appraisal is the cognitive evaluation of events and situations, and integrates mental representations of multiple kinds of information, including precognitive associations, long-term memories, expectations, goals, representations of others’ mental states, and interoception of internal bodily states (Roy et al., 2012). Appraisals include perceptions and interpretations of events with personal meaning, relevant for one’s self and future wellbeing (Ashar et al., 2017). Several lines of research have proposed neurocognitive and biological models for the relationship between negative appraisal of events and emotion (Folkman et al., 1986; Lazarus, 1991; Scherer et al., 2001), and a cognitive model that links negative appraisal of life events to depression has been put forward (Sander et al., 2018; Wang et al., 2021). In this context, our results showed that negative appraisals of experience and body interception are associated with worse MH.
Furthermore, our study reveals that in Italy during phase two of the COVID-19 lockdown, rather than the real impact that COVID-19 restrictions generated on employment or economic resources, what really impacted on MH was worry about economic conditions. The associations between worry and negative appraisal and worse MH were statistically strong, and not necessarily linked to the actual situation (as evidenced in Table 1). Worry is a state of mental distress or agitation due to concern about an impending or anticipated event, threat, or danger (Sander et al., 2018). Therefore, worsening of MH in this case seemed to be associated with concern for what was happening added to a negative evaluation of the experience.
Finally, our survey administered during the second phase of the COVID-19 lockdown in Italy, when restrictions were easing (i.e., 26 May to 4 July 2020), showed that the most influential factor in terms of MH worsening was age. The large effect size we found demonstrates that age is positively correlated with dimensions of MH; specifically, older people seem to suffer less mentally than younger people from the impact of the pandemic and associated restrictions.
It is also interesting to note that the level of education appeared to play a protective role for MH during the COVID-19 outbreak. Higher education was positively correlated with better MH, indicating that more education and older age seem to be the sociodemographic variables that best protected MH against the impact of COVID-19 lockdown. These results are confirmed by other international studies (Gloster et al., 2020).
Despite basic and experimental research highlighting the role of sex in predisposing to poor MH (Kogler et al., 2015), our statistical analysis did not find any relationship between MHI-5 items and sex. However, the role of sex was manifested when we included the relationships between life satisfaction and happiness and MH in the analysis. In this case, in fact, sex and age seem to play an important role, as shown in Table 3. Thus, sex does not seem relevant per se, but did appear to play a major role in modulating the impact that health satisfaction and perception of happiness have on MH during the pandemic.
From a biopsychosocial perspective, the results of our study suggest future avenues for research into the association between the COVID-19 pandemic and MH, exploring the different weights that the loss of positive psychological factors and the onset of negative ones had on MH during the COVID-19 pandemic. In particular, we found that, rather than the onset of psychological symptoms, it is the loss of some positive psychological factors that is associated with mental distress.
Limitations and conclusions
The most important limitation of this study is the somewhat small sample size. Hence, our sample was too small to state that our results are representative of the Italian population as a whole. Furthermore, it should be noted that the majority of the sample came from north-central Italy, and only a few subjects from the south - characterized by a very different socioeconomic context - were recruited. That being said, productivity is predominantly concentrated in the northern and central regions of the country, and therefore the economic ramifications of the COVID-19 pandemic are likely to have been more pronounced in these regions. Nevertheless, our results indicate that, in the second phase of pandemic measures, when people had undergone economic changes due to COVID-19, mental health had not been strongly affected. However, it is possible that the MH effects of such economic uncertainty may manifest more clearly afterwards. Therefore, longitudinal studies are needed in order to evaluate this issue.
Another limitation is the sampling technique. Not everyone uses social media, and this may have biased participants in ways that we are not aware of. However, having also received responses from older subjects, less accustomed to using social media, could indicate that perhaps the sample was more representative than the method of contacting respondents might immediately suggest. Another, related limitation was a potential selection bias; we are unable to state how many individuals the survey reached, and who or what proportion responded.
That being said, this study indicates that younger individuals are the most vulnerable to mental health risks in life-changing events such as the COVID-19 pandemic, and that this vulnerability increases if they have a negative appraisal of their health and QoL, as well as worry about making a living. All of these dimensions, along with reduced positive appraisal, are likely to lead to changes in future self-perception; the persistence of under-threshold low mood with negative appraisal and an increase in associated worry could increase the risk of mental health issues like depression or stress-related disorders. Other than age, education seems to be the factor most protective of MH, and, together with perceived happiness and life satisfaction (less evident in females in our results), supports good mental homeostasis. Hence, a health system that takes care of mental health and programmes aimed at promoting health should be encouraged accordingly, as suggested by the WHO. Mental and physical wellbeing programmes should be established in public institutions, particularly schools, and included in health and hygiene regulations.

