English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
Permalink
Introduction
Temperament can be defined as an early-emerging variation in emotional reactivity to internal and external stimuli that is innate, biologically determined (Rettew & McKee, 2005), and it shows solid temporal stability manifesting early in development and persisting through the lifespan (Rihmer et al., 2010). This predisposition affects the individuals’ emotional domain, activity level and related cognitions, remaining stable throughout life, even though its expression is subject to the influence of environmental experiences (Placidi et al., 1993). K. K. Akiskal and H. S. Akiskal (2005) conceptualised affective temperaments as subclinical manifestations of affective disorders and agreed with Kraepelin (1921), which asserts a continuum spectrum from affective temperaments to affective illness, ranging from adaptative to maladaptive.
In their subthreshold traits, affective disorders seem to subserve key roles in emotional communication and survival (Akiskal, 2000). An evolutionary overview across affective temperaments explains their potential social benefit when they manifest less severely. That is, the depressive or melancholic temperament, for instance, promotes sensitivity to suffering, a feature of the depressive temperament, which represents an essential attribute in a species like ours, where caring for the more vulnerable is necessary for survival (Akiskal, 2001). This temperament, which is the underlying essence of dysthymia, often leads to clinical (major) depression. On the other hand, when considering hyperthymic temperament, it is easy to understand how its characteristic (i.e., exuberant, upbeat, over-energetic and overconfident lifelong traits) might lead to social advantage and appreciation (namely in territoriality, leadership, creativity and social attractiveness) (K. K. Akiskal & H. S. Akiskal, 2005).
Current research on affective temperaments suggests that bipolarity lies along a continuum from extreme affective temperament to completely developed affective illness (Rihmer et al., 2010). Although the relationship between affective temperaments and major mood episodes is quite intricate, the current research on affective temperaments consistently shows that hyperthymic and cyclothymic temperaments are characteristic of bipolar I disorder. In contrast, a depressive temperament prevails in unipolar major depression (Rihmer et al., 2010). Far less work has been undertaken on the continuum between normal and extreme temperaments; however, the evidence that analyses that relation suggests that many temperamental traits tend to be continuously distributed (Akiskal & Akiskal, 2007; Rihmer et al., 2010; Vázquez & Gonda, 2013). This operationalisation of affective temperaments enlightens the critical role in the development of symptom formation, clinical expression, course and prognosis of affective disorders, being in many cases considered their precursors (Akiskal & Pinto, 2000; Cassano et al., 2004; Gonda et al., 2011; Mendlowicz et al., 2005). Akiskal (1992) restored the four thymic states proposed by Kraepelin (1921; i.e., depressive, manic, irritable, and cyclothymic) and developed his theory to characterise an affective trait-affective disorder continuum. The author reframed and proposed criteria to define the four temperaments (Akiskal et al., 1998) and assessed them through a psychometric instrument referred to as the Temperament Evaluation of Memphis, Pisa, Paris, and San Diego (TEMPS) (H. S. Akiskal & K. K. Akiskal, 2005), which currently exists as a semi-structured interview schedule (TEMPS-I) (Akiskal et al., 1998) and as a self-rating questionnaire (TEMPS-A) (Akiskal et al., 2005).
Light et al. (2009) developed a self-report measure of affective temperament, the Affective Temperament Questionnaire (ATQ) independently, based on the conceptualization of affective temperament by Akiskal and Mallya (1987), before the publication of the TEMPS-A. This instrument aimed to have a shorter and self-report measure of affective temperaments, and the authors minimised some sentences that represented “undesirable” traits (for example, in the subscale dysthymic, the item: “preoccupied with inadequacy, failure, and negative events to the point of morbid enjoyment of one’s failures” was rewritten as “worrying about failure.”). Subjects who participated in the original study came from a mixed sample of people from a genetics and mood disorders genetic study, which were either diagnosed with a mood disorder or where relatives of someone with a mood disorder but without a diagnosis. This sample included people with MDD (Major Depressive Disorder), Bipolar Disorder (type I and II), or never diagnosed with mood disorder (two relatives from each of the subjects were recruited prefacing 378 subjects). The questionnaire included 20 final items and a four-factor model was hypothesised including the affective temperaments: Hyperthymic, Dysthymic, Cyclothymic and Irritable. However, a 3-factor solution presented a better fit, excluding the last (and the subsequent five items), which performed poorly. Thus, Light et al. (2009) reached a final 15-item scale (ATQ) composed of three which revealed good internal consistency in Dysthymic (α=.81) and Cyclothymic (α=.83) temperaments and performing lower in the Hyperthymic (α=.68) scale. A review of the literature showed ATQ was validated and used in a wide French national study (Hantouche et al., 2002), and in some additional studies (Joyce et al., 2010), having TEMPS-A been more widely used (Vázquez & Gonda, 2013).
The impact of temperament in psychopathology (particularly mood disorders) has been described in some studies (Palagini et al., 2020; Pompili et al., 2013; Rettew & McKee, 2005). Depressive (dysthymic) temperament scored higher in people with major depressive & (MDD) and bipolar disorder (BD) (Pompili et al., 2018). Accordingly, dysthymic and cyclothymic temperaments are significantly related to depression and anxiety symptoms (Iliceto et al., 2011). On the other hand, hyperthymic temperament appears in literature positively associated with creativity (Greenwood, 2020) and extraversion, while negatively associated with depressive symptoms (Walsh et al., 2012). The present study aimed to translate and adapt the ATQ (Light et al., 2009) for the Portuguese population (PT-EU) while exploring its psychometric properties and dominant affective temperaments in two clinical samples (Major Depressive Disorder - MDD and Bipolar Disorder - BD) and a non-clinical sample. This instrument was chosen over TEMPS-A because it presents a continuous scale (instead of a dichotomic one), and it is considerably shorter and less time consuming, which can be a better option for its use in a clinical setting or wider studies with more measures. We hypothesised a 3-factor model with Hyperthymic, Dysthymic and Cyclothymic temperaments, investigated through a Confirmatory Factor Analysis (CFA). Furthermore, psychometric properties of the scale were assessed, and dominant affective temperaments were
reported and compared per diagnosis using a dimensional perspective.
Methods
Adaptation and translation of the ATQ
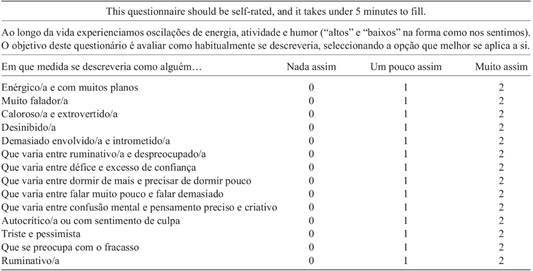
Permission to validate and translate the ATQ to European Portuguese was obtained through e-mail from the University of Otago responsible for the scale development. The translation of ATQ was conducted considering Sousa and Rojjanasrirat’s (2011) recommendations, and guidelines for best practice in validation (Boateng et al., 2018). Two clinical psychologist and one psychiatrist (Portuguese nationality with proficiency level in English) translated the scale independently. The resulting three versions were compiled into a final consensus version (see Appendix 1). Later, it was back-translated by a different health professional (psychiatrist) from English to European Portuguese, presenting good correspondence with the original. The final version was then shown to 5 health professionals (3 psychologists and 2 psychiatrists), ten people from a non-clinical sample and five people diagnosed with mood disorders, asking about the questionnaires’ clarity. The general feedback was positive (easy to understand and quick to fill); however, at least four participants commented on item 11, describing it as hard to answer because it had different ideas in the same sentence (“Quiet, passive or indecisive”). It was decided to keep the item and see how it behaved statistically.
Procedures
This study was part of a broader research project, and it was approved by the Ethics Committees of the University of Coimbra and of the Hospitals where patients were recruited, namely: Coimbra Hospital and University Centre (CHUC), Hospital Centre of Leiria (CHL), and Hospital Centre of Oeste (CHO). All participants from the clinical sample were assessed through a semi-structured Clinical Interview for Bipolar Disorders (CIBD; Azevedo et al., 2020), administered by an experienced health professional to confirm the diagnosis. The non-clinical sample was collected in the context of an unpublished master thesis (Rodrigues et al., 2018). All the participants provided written informed consent before filling in the sociodemographic data and self-report questionnaires, which were collected in paper and online (ratio 40:60; through Lime Survey). Data confidentiality and anonymity were assured, as well as clear instructions about the use and coding of the data, being treated under the GDPR (General Data Protection Regulation) and collected exclusively for research purposes.
Participants
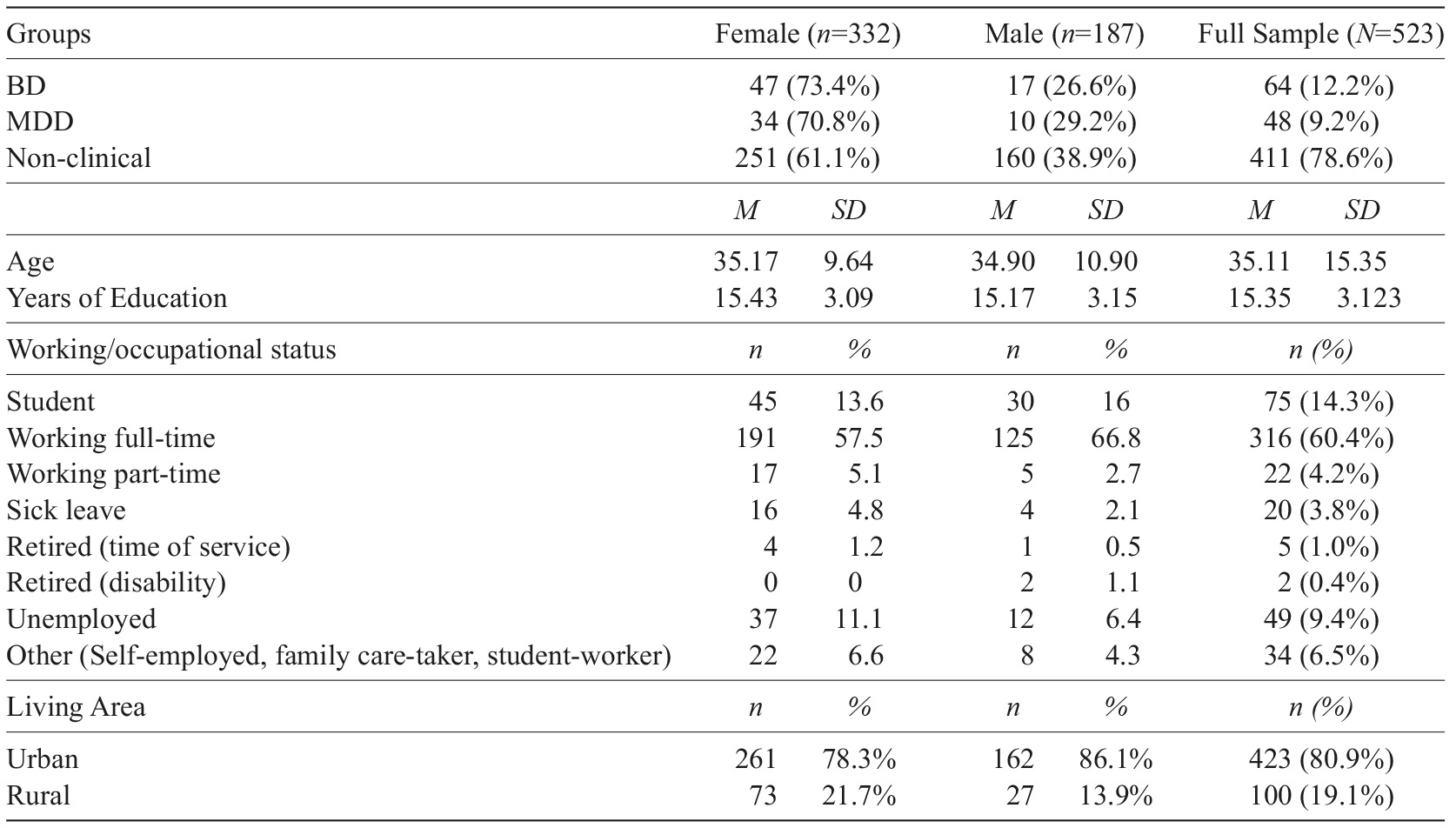
In the present cross-sectional study, data were collected in clinical and non-clinical settings: patients with BP (n=64) and with MDD (n=48) constituted the clinical sample and participants without a history of mental health illness formed the non-clinical (NC) sample (n=411). The common inclusion criteria were having between 18-65 years old, having Portuguese nationality, and knowing how to write and read Portuguese. The sociodemographic characteristics of the sample are presented in Table 1.
Clinical-sample
Our clinical sample included individuals diagnosed with either Bipolar Disorder (BD; n=64) or Major Depressive Disorder (MDD; n=48) that had no other identified co-morbidities and/or medical conditions. Patients were referenced through their psychiatrist, and had no modifications in their medication for the last 3 months before assessment (for MDD and BD, respectively), in order to decrease the likelihood of bias due to changes in medication.
Non-clinical sample
Our non-clinical sample (NC) was collected in the general community (n=411), and college setting, both in paper and online (40:60 ratio), and we considered as exclusion criteria: diagnosed or reported psychological disorder or any medical condition and/or undergoing any psychological or psychiatric treatment.
Assessment and measures
The clinical sample was assessed through the Clinical Interview for Bipolar Disorders (CIBD; Azevedo et al., 2020), designed for the diagnose of BD and related disorders through standardised questions based on the DSM-5 criteria. All subjects filled in a sociodemographic questionnaire and the following self-report questionnaires.
Affective Temperament Questionnaire (ATQ; Light et al., 2009) is a self-report instrument composed of 15 items organised into 3 subscales (Hyperthermia, Cyclothymic and Dysthymic). Each item is rated in a 3-point scale (0=not at all; 1=somewhat; 2=very much so), thus having a score between 0-30. The psychometric properties of this measure are discussed in the current study.
Hospital Anxiety and Depression Scale (HADS; Zigmond & Snaith, 1983; Portuguese version by Pais-Ribeiro et al., 2007) is a 14-item scale divided equally into two subscales, created to briefly evaluate anxiety (HADS-A) and depression (HADS-D). Scoring for each item ranges from zero to three, with three denoting the highest anxiety or depression level. A total subscale score of >8 points out of a possible 21 denotes significant symptoms of anxiety or depression. Initially designed to be used in clinical settings, it has now been widely used in primary care and community settings, and therefore, it was considered appropriate for the present study. Regarding the psychometric qualities for the Portuguese population the subscale anxiety (HADS-A) presented acceptable reliability (α=.76) and good reliability for the subscale depression (HADS-D) (α=.81). In the current study Cronbach’s alpha was good for both HADS-D (α=.84) and HADS-A (α=.84).
Altman Self-Rating Mania Scale (ASRM; Altman et al., 1997 and with the portuguese version of Shansis et al., 2003) is a short 5-item questionnaire scored from 0 to 5 (range: 0-20) to assess the presence and severity of manic or hypomanic symptoms (factors: mania, psychotic symptoms, and irritability) over a week with a cut-off score of 5 or higher indicating possible need for treatment of hypo/mania symptoms. The original version had an internal consistency of α=.89, and in the Portuguese version a α=.88 was found. In our study the internal consistency was α=.69 (including both clinical and non-clinical population).
Positive and Negative Affect Schedule-Trait (PANAS; Watson et al., 1988; Portuguese version of Galinha and Pais-Ribeiro, 2005) is a 20-item scale with two factors used assess positive affect (PA) and negative affect (NA) traits using a 5-point scale (1=very slightly or not at all; 5=extremely). The NA scale showed a good internal consistency in the original version with α=0,88, and α=0,86 in the Portuguese version and a Cronbach’s alpha of α=0,87 for the PA in the original version, and α=0,89 in the Portuguese validation study (Galinha & Pais-Ribeiro, 2005). In the current study, Cronbach alpha was excellent for the PA (α=.90) and good for the NA (α=.89).
Statistical analysis
This study had a cross-sectional design, and data were analysed using SPSS (Statistical Package for the Social Sciences, version 22; SPSS Inc, Chicago, IL, USA) and AMOS 24.0 software (Analysis of Moment Structures). The internal consistency of the scales was assessed using Cronbach’s alpha with the following threshold:>.60 is inadmissible, between .60 and .70 is weak, between .70 and .80 is acceptable, between .80 and .90 is good, and above .90 is very good (Peterson, 1994).
There was less than 1% of missing data; therefore, an expectation-maximisations analysis was used to determine if data were missing in a random pattern (Little’s MCAR test: χ 2 =171.37; df=166; p=.37). Missing values were then replaced by imputed values (Arbuckle, 2015). According to Mahalanobis distance provided by AMOS, 4 outliers were removed in the context of modification indices (Byrne, 2010). Normality was assessed through the Kolmogorov-Smirnov test, and Skewness and Kurtosis values, homogeneity of the variance using Levene’s test showed homogeneous variance and independence of the errors using Durbin-Watson statistics was assessed showing values ranging between 1.96 and 2.09, fulfilling the required assumption (Upton & Cook, 2008). We assessed for multicollinearity through VIF (Variance Inflator Factor), which showed it was non-existent (VIF<5).
Model fit was considered adequate using the cut-offs suggested by Hair et al. (2010): RMSEA<.07; CFI>.90; TLI>.90; SRMR<.08 and parsimonious fit is determined by using the normed Chi-square, with the cut-off value bellow 5.0. It is expected that all items presented factor loadings of λ≥.4 (Stevens, 2002).
Correlation coefficients between .10 and .30 were considered low, between .30 and .50, moderate and above .50 were assessed as high (Cohen, 1988).
Comparison and dominant affective temperaments measurement
A one-way ANOVA was undertaken to identify significant differences between scores across the mood disorders diagnosis groups and the non-clinical group. Significant differences (p≤.05) identified in these analyses of variance were further explored using post-hoc analysis to understand differences within the groups. In order to compare the affective temperament differences between clinical and non-clinical samples a propensity score matching was performed for age, schooling and gender to find matched healthy participants (who did not report any previous health condition). This procedure was an attempt to reduce bias due to confounding variables (age, schooling and sex).
A group of 130 people (without statistical mean differences between age, gender and schooling years) was selected through this method, however, when using Levene’s test, we noticed that the subscale Hyperthymic could not be considered homogeneous across groups. Thus we selected post-hoc test Games-Howell (Shingala & Rajyaguru, 2015).
The dominant affective temperament was calculated according to the original authors’ suggestion (M+SD), and the higher score was considered the dominant affective temperament (AT). If there were two or more equally high affective temperaments (at least one SD above M), the individual would be considered as having two or more dominant temperaments. If, on the other hand, neither of the AT was at least one SD above M, it would be coded as “without dominant affective temperament”. The values considered to group individuals into a dominant affective temperament were (M+SD): hyperthymic≥7.12; cyclothymic≥5.869; and dysthymic≥6.835. In order to compare groups smaller than 30, the Man-Whitney U non-parametric test was used to compare means and post-hoc Bonferroni correction to analyse between-groups differences.
Results
Confirmatory factor analysis
A CFA was performed using a conjoint sample (n=527) of mood disorders (n=112) and non-clinical participants (n=411). A 3-factor structure model was tested (based on the ATQ factorial structure; Light et al., 2009), with 15 items, which presented a poor fit (χ 2 /df=3.809; CFI=.88; TLI=.86; RMSEA=.073). After analysing the factor loadings (FL) and the impact on the internal consistency of the scales after the removal of the items presenting FL<|0.4|, we decided to remove item 11 (Figure 1). Although loading values were unacceptable for items 5 and 11 (FL<|0.4|), we noticed that if item 11 was removed (“Quiet, passive or indecisive”; FL=|0.36|), the internal consistency of the subscale would considerably improve (see Table 2). After the removal of item 11 and applying the suggested modification indices (the correlation of errors that had theoretical support and belonged to the same dimension and the removal of three outliers), we achieved a final model, which is presented in Figure 1.
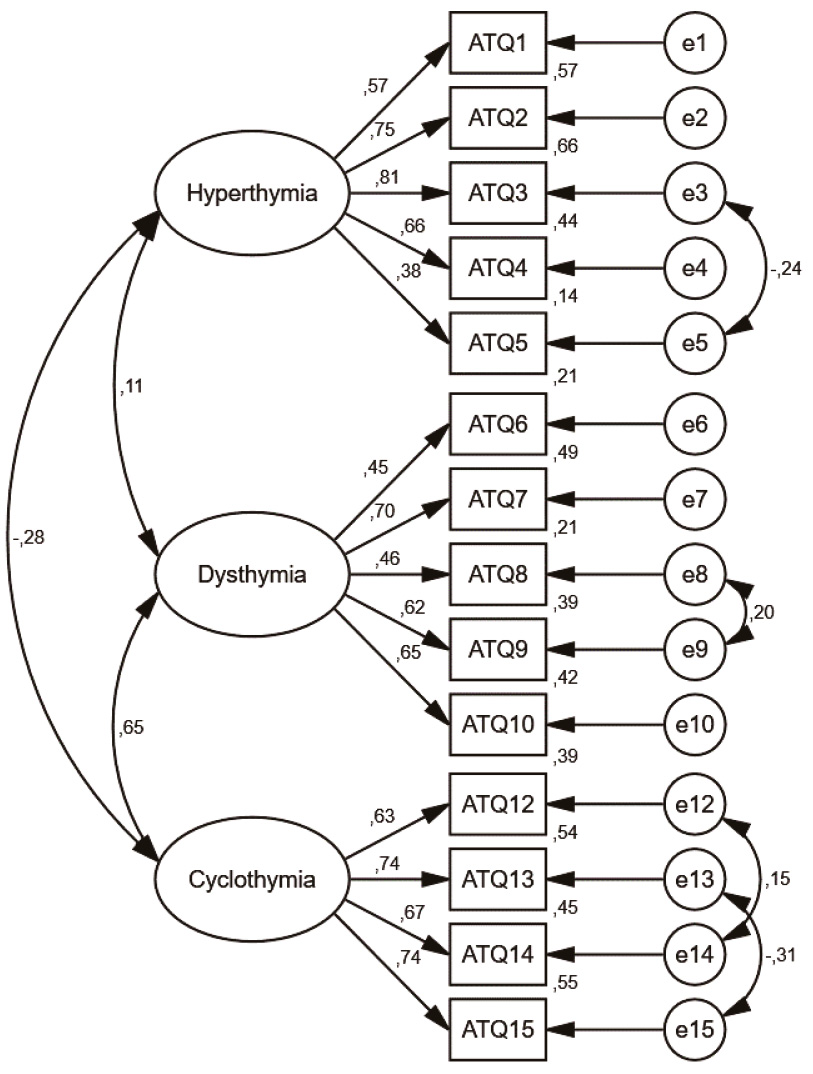
Table 2 Descriptive statistics and internal consistency of ATQ (N=523)
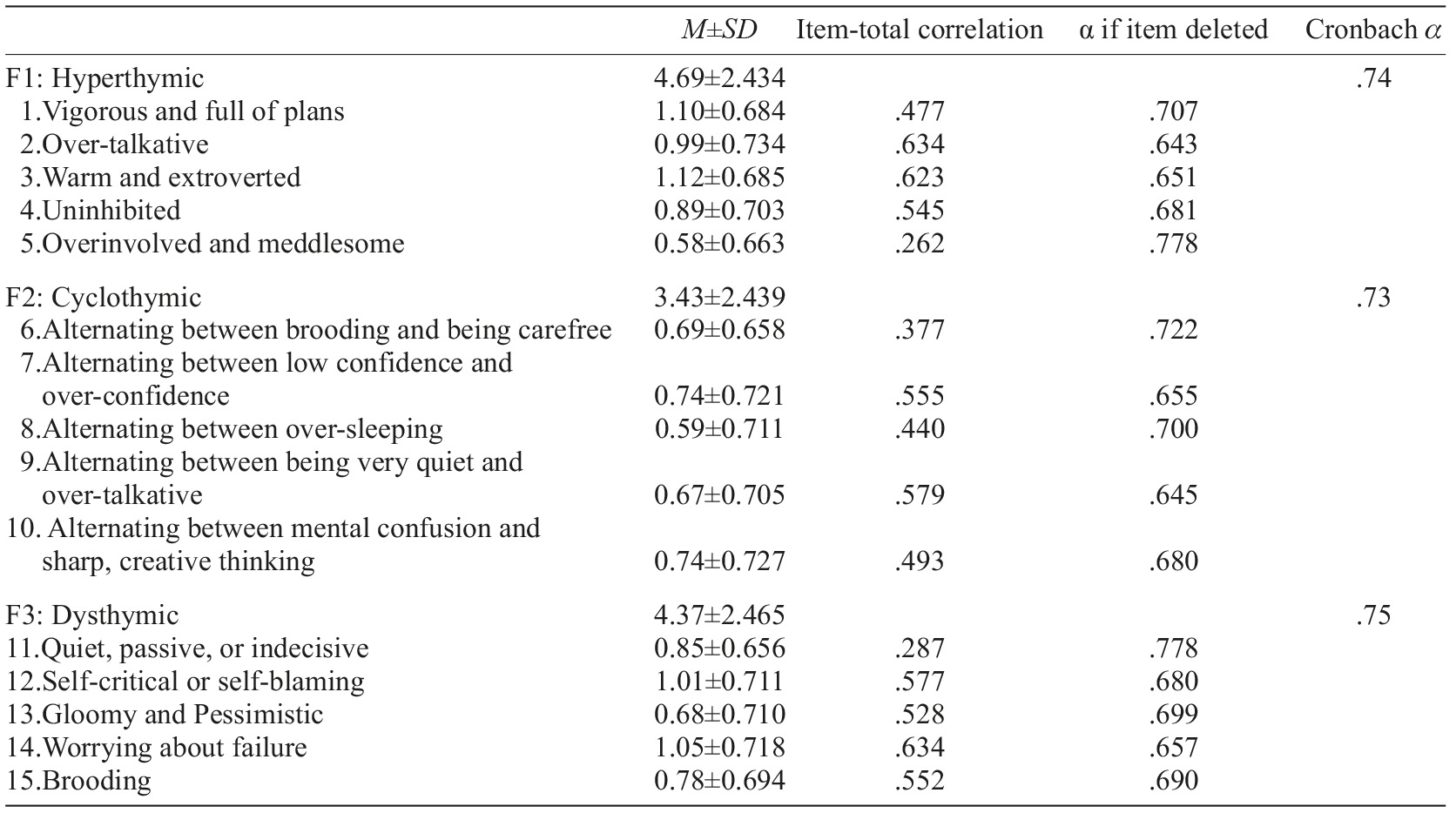
Note. M=Mean; SD=Standard Deviation.
The 3-factor model yielded a highly significant chi-square (χ 2 =221,998; df=70; p<.001), due to a large sample size. Regarding the remaining fit indexes assessed, we found a good fit (χ 2 /df=3.171; GFI=.95; CFI=.93; TLI=.90; RMSEA=.065) showing satisfactory construct validity. Items’ factor loadings (λ) were analysed to understand the amount of variance explained by the observed variable. Only item 5, did not meet the assumption of λ≥.4.
Items’ properties and internal consistency
In Table 2, item means, standard deviations and statistics (alpha if item deleted) are exhibited. The ATQ revealed acceptable internal consistency levels in all subscales with α>.70 (Hyperthymic=.74; Cyclothymic=.73; Dysthymic=.75) in the complete sample. We also assessed the internal consistency by groups, dividing the sample into a group with mood disorder (BD + MDD; n=112) and without mood disorder (n=411). The subscales Hyperthymic and Cyclothymic showed better internal consistency (Hyperthymic=.80; Cyclothymic=.73; Dysthymic=.70) in the clinical sample than in the non-clinical sample (Hyperthymic=.72; Cyclothymic=.68; Dysthymic=.72). The removal of item 11 improved the Dysthymic subscale to an α of .78, considering the complete sample.
Convergent validity
Convergent validity was assessed by analysing correlations between the ATQ temperaments (Hyperthymic, Dysthymic and Cyclothymic) and anxiety (HADS-A), depression (HADS-D), positive and negative affect (PANAS-NA; PANAS-PA) and a self-rating hypo/mania scale (ASRM). Support for the convergent validity was found with significant and positive correlations between dysthymic and depression, r=.57, anxiety r=.59, and negative affect, r=.59, and a significant positive correlation between hyperthymic and positive affect, r=.36, and mania r=.36 (all p≤.001). Cyclothymic presented significant positive correlations with depression r=.32, anxiety, r=.40, and negative affect, r=.37 (all p≤.001). All the reported correlations were highly significant and can be seen in detail in Table 3 (significance level at p<.01), except for the negative correlation between Hyperthymic temperament and negative affect, which was significant at p<.05, r=-.11, p=.015, and for the correlation between Cyclothymic and mania that was not significant r=.08, p=.116.
Table 3 Pearson’s correlations coefficients between affective temperaments and related variables (N=523)
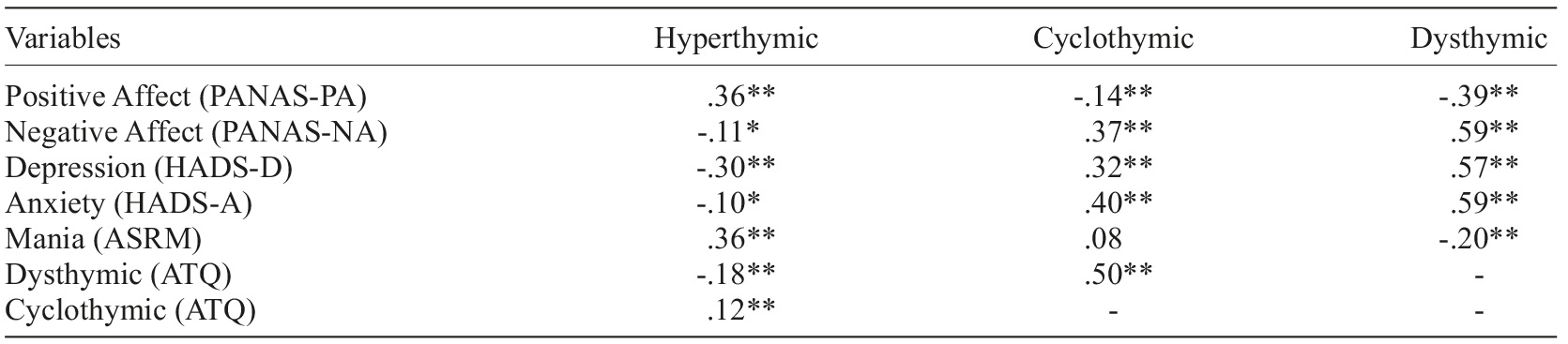
Note. *p≤05, **p≤.01; PANAS=Positive and Negative Affect Scale; PA=Positive Affect; NA=Negative Affect; HADS= Hospital anxiety and depression scale; D=depression; A=Anxiety; ASRM=Altman Self-Rating Mania; ATQ=Affective Temperament Questionnaire.
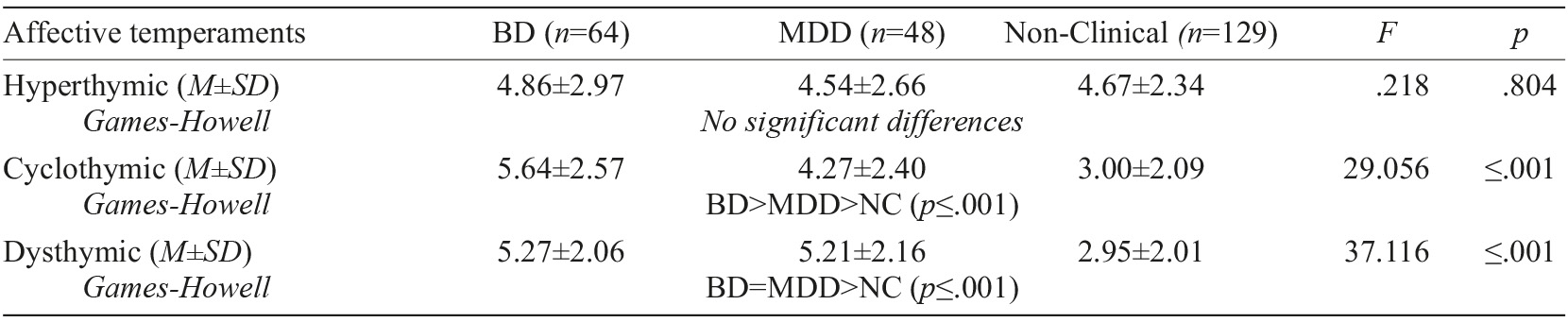
Affective temperament scores by diagnosis
Descriptive statistics of affective temperaments across mood disorders and a paired non-clinical sample (selected based on similar age, years of schooling and gender) is reported in Table 4, with the results of a one-way ANOVA, performed to compare how affective temperament differed across groups (BD, MDD and Non-clinical). This test revealed there were no significant differences within groups regarding hyperthymic affective temperament (F (2,238)=.218, p=.804), and there was a significant difference in Cyclothymic (F (2,238)=29.056, p<.001), and Dysthymic (F (2,238)=37.116, p<.001) affective temperaments. Results showed a significant difference between the mood disorders groups (BD+MDD) and non-clinical individuals regarding the dysthymic temperament, with the first (BD) presenting the highest score and MDD followed with the second-highest score. However, there were no significant differences within the mood disorder groups (BD vs. MDD). We also found significant differences regarding the cyclothymic affective temperament across the three groups, with BD scoring significantly higher than the rest and MDD scoring significantly higher than the non-clinical sample.
Dominant affective temperament by diagnosis
Participants were categorised as with or without dominant affective temperament inside their specific group (BD, MDD or Non-Clinical) as presented in Table 5, in each AT (hyperthymic, dysthymic or cyclothymic). Differences were found for dysthymic and cyclothymic dominant temperaments across groups through a Kruskal-Wallis test. Post-hoc Mann-Whitney tests using Bonferroni-adjusted alpha level of .017 (3/0.05) were used to compare all pairs of groups. The difference between mood disorders and non-clinical groups regarding dysthymic and cyclothymic remained significant, with BD showing a higher percentage of dominant cyclothymic in comparison with MDD (p≤.001), and also when compared with NC (p=.002).
Table 5 Dominant affective temperaments percentage and comparison by diagnosis (N=523)
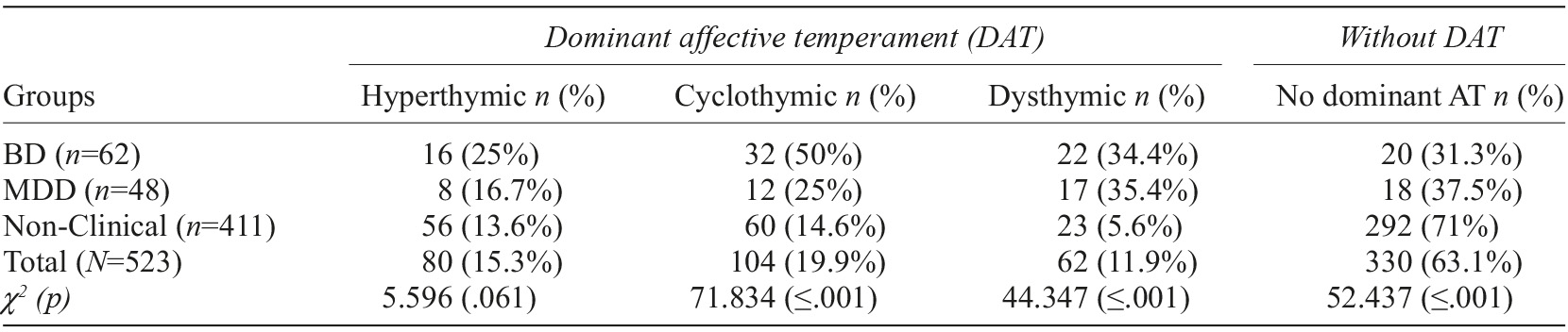
Note. BD=Bipolar Disorder; MDD=Major Depressive Disorder; AT=Affective Temperament.
There were significant differences concerning the absence of dominant AT, with 31% of BD and MDD with no dominant AT identified, in contrast with 71% of the non-clinical sample without one dominant AT (Table 5).
Discussion
Growing interest in affective temperaments has translated into an increasing number of studies across the years, contributing to an understanding of variance in clinical and non-clinical samples and with different views from an evolutionary, to a clinical and more symptom-focused perspective. Research describes affective temperaments as subclinical trait-related manifestations and often precursors of both unipolar and bipolar mood disorders (Akiskal & Akiskal, 2007; K. K. Akiskal & H. S. Akiskal, 2005; Gonda et al., 2011; Iliceto et al., 2011). Hence, the investigation of affective temperaments has an important role in the understanding of the clinical development of major mood disorders, including mood polarity and symptom formation. Current research highlights that there is still a need for further studies regarding the connection with psychopathological indicators, and with positive variables as well (Greenwood, 2020; Vázquez & Gonda, 2013; Walsh et al., 2012). Affective temperaments can also significantly affect the long-term course and outcome of affective illness. Therefore, studying them could expand the knowledge on the nosography of affective disorders and other mental disorders.
Our study indicates that the Affective Temperament Questionnaire (ATQ; Light et al., 2009) is a valid and reliable alternative to TEMPS-A (a dichotomic 110 items questionnaire; H. S. Akiskal & K. K. Akiskal, 2005) which, from our knowledge, was the only instrument validated to the Portuguese population to assess affective temperaments (Figueira et al., 2008). After testing the factorial structure through CFA, we confirmed our initial hypothesis of a three-factor model with hyperthymic, dysthymic and cyclothymic affective temperaments. The model differed from the original by removing item 11 “Quiet, passive or indecisive” from the Dysthymic affective temperament subscale. The decision to eliminate the item was based on its poor psychometric properties, and lack of clarity (as previously described by people queried about clarity and acceptability of the questionnaire). This exclusion improved the overall adjustment of the model. We followed a conservative step-by-step approach in applying modification indexes to our three-factor hypothesised model, following the recommendations to correlate errors from items that we considered to have a shared variance and a theoretical justification. Thus, we correlated each of the four errors, considering their conceptual similarity (errors of items 3 and 5 from hyperthymic, errors 8 and 9 from dysthymic and pairs of errors 12-14 and 13-15 from cyclothymic). After correlating these four pairs, as suggested by AMOS, and extracting outliers according to Mahalanobis distance, a final adjusted model was achieved, supporting structural validity to the ATQ with 14 items: 5 for hyperthymic, 5 for cyclothymic and 4 for dysthymic. Overall, the model presented a good fit with an adequate chi-square under 5, confirming its parsimonious fit, even though it was a highly significant result that can be easily justifiable by the large sample. The remaining reported and advised fit indexes including root mean square error of approximation (RMSEA), comparative fit index (CFI), and Tucker-Lewis index (TLI) supported a satisfactory construct. The contribution of each item was analysed by verifying their factor loadings (λ) to understand the amount of variance in the observed variable that the underlying construct was able to explain. From this analysis, it was possible to verify that all items, except for item 5 “Overinvolved and meddlesome”, met the assumption of λ≥.4 and therefore represent an important contribution to the factor that they belong to. In this respect, Stevens (2002) recommends interpreting factor loadings with an absolute value greater than |.40| (which explains around 16% of the variance in the variable); however, he also argues that in a large sample, lower values can also be significant. In our sample of 523 an item with loading of |.38| is significant, according to those same principles. The decision to keep item 5, nonetheless, was also based on the item’s relevance and recognised contribution to the hyperthymic temperament (Pompili et al., 2018).
Furthermore, the descriptive statistics analysis for the 14 final items and the three affective temperaments in the ATQ revealed acceptable internal consistency across the three dimensions. These results were different from those found in the original investigation, which obtained a value of internal consistency of α=.68 bellow recommended for Hyperthymic dimension, while in the current study was acceptable. Nevertheless, it must be considered that the original study was conducted with a family-based sample of individuals with MDD and BD, which might have affected the hyperthymic traits. According to a recent study, those traits differ quite significantly across bipolar family-based samples (Greenwood, 2020).
Additionally, support towards convergent validity was corroborated by our findings, with significant correlations between .30 and .70 as desirable between the ATQ subscales and the selected variables, behaving in the expected direction across variables. Dysthymic AT was positively correlated with depression as expected, supporting the idea of this being a precursor of major affective episodes. Yet, the correlation was only moderate, pointing to a differentiated construct from depression even so. Anxiety correlated higher than depression with dysthymic AT, consistent with previous studies (Harnic et al., 2013; Iliceto et al., 2011; Pompili et al., 2013). The study of Pini and collaborators (1997) analysed the relevance of anxiety disorders in bipolar depression, unipolar depression and dysthymia, revealing a strong association between dysthymia and anxiety spectrum disorders and especially generalised anxiety disorder. Our results are in line with the conclusions obtained in this study, since we found a high association between Dysthymic temperament and anxiety. Concerning Hyperthymic temperament, a negative association with depression and anxiety was found, which was expected according to several studies that emphasise ant point hyperthymic traits as protective and more helpful, correlating with positive traits (Greenwood, 2020; Harnic et al., 2013). Morvan and collaborators (2011) described hyperthymic temperament as being associated with a decreased likelihood of depression, consistent with views of these psychological traits’ positive and potentially protective nature. These considerations are also consistent with our results, which reveal a positive correlation between hyperthymic temperament and positive affect and also with hypo/mania symptoms. Cyclothymic, on the other hand, revealed a positive correlation with negative affect, depression, and anxiety, showing that cyclothymic temperament seems to be associated with higher levels of psychological distress. An inverse relation with positive affect was found, with low magnitude (having presented a low negative correlation). These results were also consistent with previous studies that discuss strong correlations between cyclothymic temperament and psychopathological symptoms (Akiskal et al., 2003; Perugi et al., 2015; Walsh et al., 2013).
Affective temperaments manifested weak to moderate correlations with one another, being the highest correlation of .50 between cyclothymic and dysthymic temperaments, which is understandable as they are expected to partially overlap due to cyclothymic comprising a variation between high and low mood states, and similar results were found in TEMPS-A Portuguese validation study (Figueira et al., 2008). Hyperthymic and dysthymic temperaments correlation were low and negative. Though this occurred on a lower magnitude than the one described in the international study of Vázquez and collaborators (2012), differences might be due to the fact that their results were obtained through TEMPS-A, and even though ATQ is based on TEMPS, it suffered considerable changes in the reformulation of items and type of answer; thus, a direct comparison cannot be assumed. On their study, conducted in 6 countries including Portugal, these affective temperaments were moderately and negatively correlated. Finally, a positive and low correlation was found between Hyperthymic and Cyclothymic temperaments. Even though Hyperthymic temperament could be expected to equally overlap Cyclothymic temperament, it is also understandable that its relationship is in fact weaker, since within cyclothymic temperament research has revealed higher prevalence of periods of dysthymia and association with dysthymic traits, rather than hyperthymic (Innamorati et al., 2015; Perugi et al., 2015; Pompili et al., 2009).
When looking at the affective temperament differences across groups, it is plausible to say that there are consistent differences concerning cyclothymic and dysthymic affective temperaments, pointing toward the specificity and potential capacity of the ATQ to discriminate between clinical and non-clinical samples. However, the same differences were not found regarding hyperthymic temperaments, and that might be due to a higher mean and standard deviation of our non-clinical group than the one presented in Light and collaborators (2009), which is quite close to people with mood disorders in this study. Several explanations can be discussed about the reason for those similarities. On the one hand, hyperthymia has always been difficult to measure, with self-rating scales described as unreliable (Sajatovic et al., 2015). On the other hand, hyperthymic temperament might be scored similarly by people with and without affective disorders; nevertheless, being felt with a different intensity that the questionnaire might not be sensible to detect, which raises the need for more sensitive items. It is important to understand if this lack of specificity comes from the adaptation of the items translated to Portuguese, as people might be overrating the items or admitting the possibility that cultural differences might also impact the way people perceive themselves.
We also analysed dominant affective temperaments across groups taking a dimensional approach, based on the highest score that each individual achieved on every single AT, if it was at least one standard deviation above the mean. We categorised participants as having dominant temperament or not having one, thus generating a significantly disproportionate distribution of dominant temperament types relative to mood disorder diagnosis. The outcomes presented an expected distribution consistent with clinical understanding. Findings disclosed that the percentage of hyperthymic temperaments did not differ significantly across groups, which is consistent with the previously described comparisons, being - 25%, 16.7%, and 13.6% among individuals with BP, MDD, and NC, respectively. Our results presented slightly higher percentages than the original authors of the ATQ. The dysthymic temperament was more prevalent in people with MDD, as expected, even though it was only slightly superior to people with BD and when compared with Light and collaborators (2009) scores. Our outcomes thus revealed a distribution regarding a dominant dysthymic temperament of - 35.4%, 34.4%, and 5.6% among individuals with MDD, BP, and NC, correspondingly. According to previous studies of Mitchell and Malhi (2004), these results are not surprising, having demonstrated how depression frequently presents as subsyndromal, minor or dysthymic depression in bipolar disorder. The cyclothymic dominant temperament within our study constituted half of BP individuals, 25% of MDD individuals, and around 15% of the non-clinical sample. Contrastingly and as expected, 71% of the non-clinical sample did not present any dominant affective temperament, while BD and MDD, in turn, varied between 31% and 37%. This is coherent with the findings of Light and collaborators (2009) and Akiskal and Pinto (2000), even though our percentages are marginally superior in mood disorders.
An interesting and puzzling paradox surrounds bipolar disorder (and other psychotic disorders) from an evolutionary point of view: why would traits related to substantial social and cognitive impairments and increased mortality be maintained, even though they affect fitness, fertility, and survival. A possible explanation discussed by Greenwood (2020) reflects on Paracelsus (doctor and philosopher) sentence “the dose makes the poison”, pointing out how mild manifestation of such temperaments as hyperthymic and cyclothymic have been positively associated with leadership skills, disinhibition, thrive to success and creativity, which are well suited for nowadays work and social challenges. Thus, the study of temperament as a continuum between healthy and affective disorders helps understand the vulnerability and risk factors, at the same time it can highlight positive traits and creativity, leading to innovative societal contributions. Greenwood (2020) argues that a moderately elevated mood may increase fluency and divergent thinking; however, extreme elevations in mood may hinder creative accomplishments. Milder presentations of symptoms in the form of bipolar spectrum traits, such as cyclothymic temperament and hypomanic traits, appear to confer increased creativity and/or productivity less dramatically and more consistently. These and other shared vulnerability traits point to the possibility of positive adaptive traits under a balancing selection that maintains bipolar disorder in the population despite the inherent disadvantages of the illness.
Clinical implications
Approaching affective temperaments as a continuum and look at mood disorders as part of that spectrum can help us interpret the variation of temperaments as a possible vulnerability, but also as part of a variety of possible presentation of traits, that can indicate both risk and benefit if well regulated. Thus, a quick and short scale like the ATQ might facilitate further research and would allow the identification of early signs of affective vulnerability for developing clinical forms of affective and mood disorders in clinical setting and primary care. Furthermore, considering the relationship between affective temperaments and other mental illnesses, it might be possible to gauge the subjects’ susceptibilities and to work towards reducing risk factors in other areas of mental health as well.
Limitations and future suggestions
One of the limitations of this study relies on its transversal design, which makes it difficult to establish a causal relationship between the variables under analysis and potential longitudinal changes of temperament scores across time. Also, test-retest reliability was not assessed, which would be important to further attest for the stability of the scores and the stability of the constructs. Moreover, the non-clinical sample was partially collected in a college setting, which makes it different from the clinical samples, forming 14.3% of the total sample.
Future research should try to find different ways to assess hyperthymic temperaments, either by adding other items or by cross analysing with TEMPS-A and different self-rating hypomania scales, to enhance the discriminant validity of the Portuguese questionnaire. Overall, future research should seek to assess the ATQ in different samples, in different moments across time, to contribute and explore how people with dominant affective temperaments develop in time (starting with younger cohorts and assessing them later in a different age and moment in life).
Conclusion
The ATQ is a valid and reliable self-report measure to assess affective temperament in clinical and non-clinical samples, thus providing a shorter and more practical alternative to TEMPS-A, the only known validated self-report option to assess affective temperament in the Portuguese population (Figueira et al., 2008).