English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
Permalink
Introduction
Emergency or first responders and crisis workers are required to respond to a range of emergencies with little or no prior knowledge about what they are about to encounter, and they are frequently confronted with difficult and risky situations which require rapid decision-making and action (Armstrong et al., 2014; DeJoy et al., 2017; Regehr et al., 2008). Firefighters are put in difficult emergency situations in their line of work (Jimenez-Herrera & Axelsson, 2015). The emergency care can be experienced as demanding, not just physically, but also mentally (Regambal et al., 2015), wherefore critical incidents can sometimes even diminish the firefighter’s ability to cope due to mental distress and emotional strain in a horrific situation (Tuckey & Hayward, 2011; Tuckey & Scott, 2014). This population is exposed to extreme conditions and repeated traumatic events, negatively impacting physical, psychological and emotional well-being, and therefore they are more likely to develop secondary trauma (Armstrong et al., 2014; DeJoy et al., 2017; Meda et al., 2012) and have an increased risk of experiencing compassion fatigue (Gonzalez et al., 2019).
Compassion Fatigue (CF), also known as secondary victimization, secondary traumatic stress and vicarious traumatization, is a phenomenon that can occur when one cares for others experiencing emotional pain, i.e., when a person is emotionally affected by the trauma of another, such as a client or a family member (Figley, 2002a; Sinclair et al., 2017). CF is “the final result of a progressive and cumulative process that is caused by prolonged, continuous and intense contact with patients, the use of self, and exposure to stress” (Coetzee & Klopper, 2010), or can be defined as the reduced capacity or interest in being empathetic and results in natural behaviors and emotions when knowing about a significant other who has experienced a traumatizing event (Adams et al., 2008; Nimmo & Huggard, 2013). One can be traumatized by being harmed and by witnessing and helping other people who are suffering (Figley, 2002b; Nimmo & Huggard, 2013). CF is associated with feelings of helplessness and confusion, and the prominent symptom of CF is reduced empathy for victims (Figley, 2002a; Sinclair et al., 2017). It manifest in marked physical, social, emotional, spiritual and intellectual changes that increase in intensity (Coetzee & Klopper, 2010). In other words, is the psycho-emotional distress that originates because of long-term self-sacrifice coupled with prolonged exposure to difficult situations (Cocker & Joss, 2016).
Both secondary trauma (ST) and job burnout (JB) are important features that lead to CF (Adams et al., 2006). Despite being different concepts, each has a unique effect on well-being (Adams et al., 2008). Both these components are characterized by emotional exhaustion due to working with survivors of trauma. The cumulative effects of compassion can therefore lead to secondary traumatization: those who work with traumatized subjects can have intense and painful emotional reactions which interact with factors that affect the personal characteristics of the subject himself and external stressors, such as patient satisfaction, their presence numerous and all organizational objectives (Hubbard et al., 2017; Shahar et al., 2019).
ST (Figley 1995), or vicarious traumatization (McCann & Pearlman, 1990; Regehr et al., 2002; Saakvitne & Pearlman, 1996), is related to the development of symptoms of traumatic stress, among health workers, as a consequence of working with traumatized individuals. JB is a response developed by prolonged contact with critical situations and is characterized by emotional exhaustion, depersonalization and reduced personal accomplishment (Sprang et al., 2011). This phenomenon has identical symptoms to Secondary Traumatic Stress Disorder (STSD) and Post-Traumatic Stress Disorder (PTSD), such as re-experiencing the traumatic events (e.g., recurrent and intrusive distressing recollections of the event or the client, including images, thoughts or dreams), persistent avoidance of stimuli associated with the trauma and persistent symptoms of increased arousal (e.g., difficulty falling or staying asleep, hypervigilance, exaggerated startle response) (Figley, 2002b). The literature indicates that CF is associated with a high incidence of various conditions such as depression, anxiety, interpersonal problems and psychological distress, as well as decreased well-being (Beaumont et al., 2016; Gonzalez et al., 2019; Lee et al., 2014; Sprang et al., 2011; Sun et al., 2016).
The burnout is associated with stressors present in the work environment, such as longer shifts, conflicts with colleagues, lack of personnel and consequent increase in workload (Schmidt & Haglund, 2017). The burnout occurs as a result of prolonged exposure to stressful interpersonal situations, and is characterised by emotional and physical exhaustion, job dissatisfaction (Mento et al., 2016). The symptoms experienced by professionals significantly affect work significance, functioning, since high levels emotional exhaustion, cynicism, and low perceived professional efficacy are related to poor occupational satisfaction and performance, the general consequences seem to be a reduced quality of life (Bell et al., 2019; Hannah & Woolgar, 2018; Hotchkiss & Lesher, 2018; Hunt et al., 2019).
Alexythymia and empathy are personality traits affecting the individual capacity to cope with stress (Franco et al., 2020). The empathy plays a key role in the situation of emergency, empathy, being the attitude of to take care of the pain of others and the ability to perceive their suffering, their sadness, their pain, while remaining aware of the distinction between themselves and the patient (Settineri et al., 2018). Alexithymia conveys a substantial difficulty in identifying, describing and communicating emotions, distinguishing them from bodily sensations, and an externally oriented thinking style (Hiirola et al., 2017).
CF is also negatively related to empathy and positively related to alexithymia (Gleichgerrcht & Decety, 2013). In other words, workers with negative self-oriented emotions elicited by someone in pain/distress and with a diminished ability to empathize can lead to CF. Alexithymia is also associated with both aspects of CF, i.e., JB and ST, characterized by an inability to identify and describe feelings and the tendency to focus attention externally rather than on feelings (Gleichgerrcht & Decety, 2013). Alexithymic subjects may have ineffective coping strategies and lower compensation resources to face Secondary Traumatic Stress, leading to chronic compassion fatigue and eventual burnout (Franco et al., 2020).
Although men tend to experience more traumatic incidents, women have a higher incidence of PTSD (Beaumont et al., 2016) and are consequently more subject to CF, leading them also to experience more burnout (Beaumont et al., 2016; Gleichgerrcht & Decety, 2013; Thompson et al., 2014; Zeidner et al., 2013). On the other hand, as age and years of work increase, CF tends to decrease (Sprang et al., 2011; Thomas & Otis, 2010; Thompson et al., 2014). Additionally, even though critical incident responders do not experience the trauma directly, their indirect exposure to trauma can lead to CF and burnout (Figley, 2002a; Gleichgerrcht & Decety, 2013). Other factors, such as the degree of exposure, personal history, social support and environmental factors, predict the risk of experiencing CF (Adams et al., 2008; Boscarino et al., 2004).
Adams et al. (2006) were the first researchers to assess the basic psychometric properties of the 30-item Compassion Fatigue (CF) Scale-Revised (Gentry et al., 2002). This scale was developed by Figley (1995) based on clinical experience, and versions of the scale have been used in several studies (Jenkins & Baird, 2002; Stamm, 2002). Factor analysis of the 30 items in the scale was conducted, dropping items until only two factors remained, forming a Work Burnout scale (eight items) and a Secondary Trauma scale (five items), which compose the 13-item CF-Short Scale. In other countries, this scale has been applied in CF studies among emergency workers in Chinese and Euro-Asian settings, respectively, the C-CF-Short Scale (Sun et al., 2016) and the CF-SC (Dinç & Ekinci, 2019).
So far, no scale has been developed to evaluate CF in firefighters in Portugal. To fill this gap, this study aimed to adapt and explore the structure of CF and examine the psychometric properties of the Portuguese version of the CF-Short Scale. For that purpose, we used a sample of firefighters. Following prior studies, we hypothesized that CF includes two factors in Portuguese emergency workers: ST and JB.
Methods
Participants
Eligibility criteria were being a firefighter, over 18 years old, of Portuguese nationality, being active in the fire department and not having a cognitive or physical inability to prevent from independently replying to the self-report measures. The researcher invited 570 firefighters to participate in the study. Of these, following the inclusion criteria, a total of 512 Portuguese firefighters were recruited, 74% men, with an average age of 36.28 years old (range 18-63 years), 2.5% of age data missing. Most firefighters were single (43%) or married (36.5%), and the majority belonged to the Fire Department of the North (54.5%), followed by the Center (42.2%) and South (3.3%). Regarding education, 30.5% completed basic education, 49.2% completed high school, and 20.3% had higher education.
More than half the participants were volunteer firefighters (53.9%) or employees of a fire association (35%). Regarding the category of a firefighter, the majority were first, second, or third-class firefighters (71.6%), some were commander, second commander or deputy commander (7.1%) and the remainder belonged to other categories. The mean number of years of work experience was 14.27 (SD=10.996), ranging between less than a year and 47 years.
Procedure
This study was approved by the Ethics and Deontology Committee. The commanders of 41 Portuguese Fire Departments across the country were initially contacted to obtain authorization to administer the questionnaires to the firefighters at the beginning or end of an instruction/meeting or another suitable time or asked to disseminate the study. The study’s aims were explained to the commanders and firefighters, emphasizing that their voluntary cooperation and confidentiality were ensured. Paper-and-pencil and online questionnaires were the main data-collection method adopted in this study. However, the entire protocol was also available via the online server to increase the sample size since there is extensive evidence that the two forms of collection are equivalent (Gwaltney et al., 2008). The link to the online survey was also disseminated through newsletters, mailing lists and social networks. Informed consent was obtained from all participants. Data collection were between March and June of 2019.
For this study, the CF-Short Scale was first translated from English into Portuguese by an expert Portuguese-English bilingual speaker and then back-translated into English by another. 5 expert panel of psychologists and other translators evaluated discrepancies between the English and Portuguese versions. Discrepancies were gradually reduced through an iterative review process.
Instruments
Socio-Demographic Questionnaire. The sociodemographic questionnaire included items regarding age, gender, education, marital status, and other professions (in the case of being a volunteer firefighter). There were also several questions regarding the firefighter work, such as the regional location of the fire brigade, firefighter career (volunteer or professional), category or position in the fire brigade, and years of working as a firefighter.
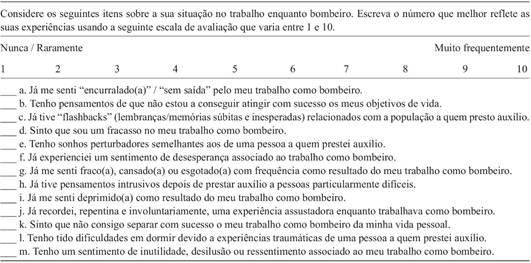
Pt-CF-Short Scale. The CF-Short Scale is a 13-item self-report questionnaire that consists of two subscales: (1) a five-item Secondary Trauma scale and (2) an eight-item Job Burnout scale (Adams et al., 2006) (Appendix 1). Respondents are asked to consider each item and indicate how closely it reflects their experience, using a ten-point Likert-type scale (1 “never or rarely” to 10 “very often”). In the study of the short-scale (Adams et al., 2006), the Cronbach α coefficient was .80 for the Secondary Trauma scale and .90 for the Work Burnout scale, and the full CF-Short Scale had a Cronbach α of .90.
This scale included a process of translation. Authorization from the authors of the original scale to disseminate the scale with their articles was obtained.
Additional scales
Kessler Psychological Distress Scale (K10) (Pereira et al., 2019). K10 is a self-report measure that assesses the frequency of non-specific psychological distress symptoms for the last 30 days and is based on questions about anxiety and depression symptoms (Kessler et al., 2002). The K10 contains ten items rated on a five-point Likert scale (ranging from 5 “all of the time” to 1 “none of the time”) (Kessler et al., 2002). The total score ranges from 10 to 50, with higher scores indicating higher levels of distress and scores higher than 22 suggesting the risk of having a mental disorder. Scores between 10 and 15 indicate “low distress”, 16 to 21 “moderate”, 22 to 29 “high” and 30 to 50 “very high” (Kessler et al., 2002). The Cronbach’s alpha of the Portuguese version (.91) confirms good internal consistency (Pereira et al., 2019).
Brief Symptom Inventory (BSI) (Canavarro, 2007). BSI is a self-report measure that assesses psychopathological symptoms across nine symptom dimensions (somatization, obsession-compulsion, interpersonal sensitivity, depression, anxiety, hostility, phobic anxiety, paranoid ideation, and psychoticism) and three global indices (global severity index, positive symptom distress index, and positive symptom total) (Derogatis, 1982). The BSI contains 53 items answered on a five-point Likert scale (ranging from 0 “not at all” to 4 “extremely”). The Cronbach’s alpha for the nine symptom dimensions ranges from .62 (psychoticism and phobic anxiety) to .80 (somatization) (Canavarro, 2007).
Impact of Event Scale-Revised (IES-R) (Matos et al., 2011). IES-R assesses the subjective suffering related to a specific life event (Weiss & Marmar, 1997). It contains 22 items distributed over three subscales: intrusion (eight items), avoidance (eight items), and hyperarousal (six items). Each item is answered using a five-point Likert scale (ranging from 0 “not at all” to 4 “extremely”) (Weiss & Marmar, 1997). The Cronbach alpha of the total scale (.96) reveals excellent internal consistency (Matos et al., 2011).
Toronto Alexithymia Scale (TAS-20) (Praceres et al., 2000). TAS-20 is a self-report instrument with 20 items distributed over three factors, according to the construct of alexithymia: difficulty in identifying feelings and distinguishing them from the bodily sensations of emotions, difficulty in describing feelings to others, and externally oriented cognitive style of thinking (Bagby, Parker et al., 1994; Bagby, Taylor et al., 1994). Each item is answered on a five-point Likert scale (ranging from 1 “strongly disagree” to 5 “strongly agree”) (Bagby, Parker et al., 1994; Bagby, Taylor et al., 1994). The Cronbach alpha of the total scale (.79) shows appropriate internal consistency (Praceres et al., 2000).
Interpersonal Reactivity Index (IRI) (Limpo et al., 2013). IRI is a measure of empathy consisting of 24 statements about feelings or thoughts that a person may or may not have experienced (Davis, 1980, 1983). It has four subscales (perspective taking, fantasy, empathic concern, and personal distress), each with six items. The items are answered on a five-point Likert Scale (ranging from 0 “does not describe me well” to 4 “describes me very well”). The Cronbach’s alphas for the four subscales range from .74 (perspective taking) to .83 (fantasy) (Limpo et al., 2013).
World Health Organization Quality of Life-Bref (WHOQOL-Bref) (Serra et al., 2006). WHOQOL-Bref is an instrument that measures the quality of life (The WHOQOL Group, 1998). It is organized into four domains: physical, psychological, social relationships, and environment. This instrument comprises 26 items, answered on a five-point Likert Scale, with two items corresponding to the general perception of the quality of life and the remaining 24 items corresponding to the four domains. Cronbach’s alpha of 26 items (.92) confirms good internal consistency (Serra et al., 2006).
Data analysis
Statistical analysis was performed with Statistical Package for Social Sciences, version 26 (SPSS Inc., Chicago) and Analysis of Moment Structures (AMOS), version 26. Descriptive statistics (means, standard deviations, frequencies) summarize the participants’ sociodemographic information. We didn’t have outliers nor missing values. To examine the goodness-of-fit of different factor models, AMOS Graphics™ software v.26 was used. All the analyses were performed according to the Maximum Likelihood Estimator Type. To test the factorial structure of the Pt-CF-short scale, we used a confirmatory factor analysis (CFA) to verify if the solution of the original model (Adams et al., 2006) would obtain an acceptable fit. Tabachnick and Fidell (2013) suggested that a minimum sample size of 300 or more is necessary to perform a confirmatory factor analysis, providing adequate statistical power for data analysis. An a priori power analysis was also conducted to determine the sample size required to detect a meaningful effect. Data revealed that the sample size of 288 would be sufficient to detect medium to large effects [effect size=0.50, power=0.95, Free Statistics Calculators 4.0] at a significance level of 0.05. The chi-square test (χ²) was reported to assess the magnitude of the discrepancy between hypothesized and observed model. However, the χ² statistic is sensible to large samples (Kelloway, 1995). We also evaluated other fit indexes recommended by Kline (2005): (i) the Comparative Fit Index (CFI), which compares the sample covariance matrix with an independence model (all indicators’ variables were zero), (ii) the Root-Mean-Square Error of Approximation (RMSEA), which demonstrates how the estimation of the parameters would fit the population covariance matrix, and (iii) the Standardized Root Mean Square Residual (SRMR), an absolute measure of fit and defined as the standardized difference between the observed correlation and the predicted correlation. An acceptable-fit model was determined if RMSEA≤.08, CFI>.90, and SRMR<.10 (Kline, 2005). Alternative factor models were generated and tested according to the modification indexes (MII>11).
So, three models were tested, being (i) a model with two factors involving secondary trauma and job burnout dimensions, derived from the original model (Sun et al., 2016), (ii) a unidimensional model considering strong correlations between the items, and (iii) a second-order factor model, allowing covariance of errors, also with two first-order factors (ST and JB), proposed by Dinç and Ekinci (2019).
Following the model specification, reliability was investigated using (a) Cronbach’s alpha coefficient. Normality was tested using visual methods such as histogram and box plot and the Kolmogorov-Smirnov statistical test. The Spearman correlation coefficient was used since the normality assumptions were violated for all scales included in this analysis. Convergent validity was assessed by exploring Spearman’s rank correlations between Pt-CF-Short Scale and K10, BSI, IES-R, TAS-20, IRI, and WHOQOL-Bref measures, using IBM SPSS version 26 (IBM Corp., Armonk, USA). The correlations were classified as weak (0-.3), moderate (.3-.7), and strong (>.7-1.0) (Ratner, 2009). Also composite reliability and inter-item correlation was calculated.
Finally, to examine discriminant validity differences in the demographics, variables such as gender, age, work experience, and perception of trauma level were analyzed. Thus, independent-samples t-tests and one-way analyses of variance (ANOVA) were used. ANOVA with three levels (years of experience), and multiple comparisons were used to understand which levels differ from each other when the result was significant. The results were considered statistically significant if the p-value was <.05.
Results
CFA comparing alternative models
Three alternative models were tested using CFA. We estimated (i) a model with two factors involving secondary trauma and job burnout dimensions, (ii) a unidimensional model, and (iii) a second-order factor model, allowing covariance of errors, also with two first-order factors (ST and JB). Chi-square values were significant, rejecting the models. However, we know that this statistic is sensitive to sample size. Therefore, other fit indexes were analyzed following the cut-off criteria (Kline, 2005) considered indicators of the model’s good fit.
The two-factor solution derived from the original model demonstrated a marginal fit, since CFI=.903, RMSEA=.088 and SRMR=.0515. In this framework, the model did not pass the RMSEA criterion. The standardized factor loadings ranged from .654 to .722 for the ST dimension and from .488 to .736 for the JB dimension (see Table 1). High correlations between factors were observed (r=.92). Based on this strong association, a single latent model where the factor CF loads on all 13 items were tested. Higher error covariance was observed in more than half the items. Therefore, no additional covariance paths were allowed between error terms. The two-factor structure was substantially better than the one-factor model (see Table 1). However, the results confirmed the poor fit of the one-factor and two-factor solutions. For this reason, a second-order factor model was also examined, showing slightly better fit indexes.
Table 1 Confirmatory Factor Analysis (CFA): Fit indexes for each model tested (n=512)

Note. ***p<.001; aAdded path between error terms for items c and j, e and j, b and m; χ²=Chi-square; df=degrees of freedom; CFI=Comparative Fit Index; RMSEA=Root Mean Square Error of Approximation, SRMR=Standardized Root Mean Square Residual.
A second-order factor called CF (see Table 1), integrating secondary trauma and job burnout as first-order factors, was examined. Based on the high modification indices (MII>11) in this model, we allowed errors to covary for items c and j, e and l, b and m and improved the model fit. The covariance between c and j was already been allowed. Correlations between the errors of items e and l and b and m were conceptually justified. This last solution was the one with the best fit, compared to the others (see Figure 1).
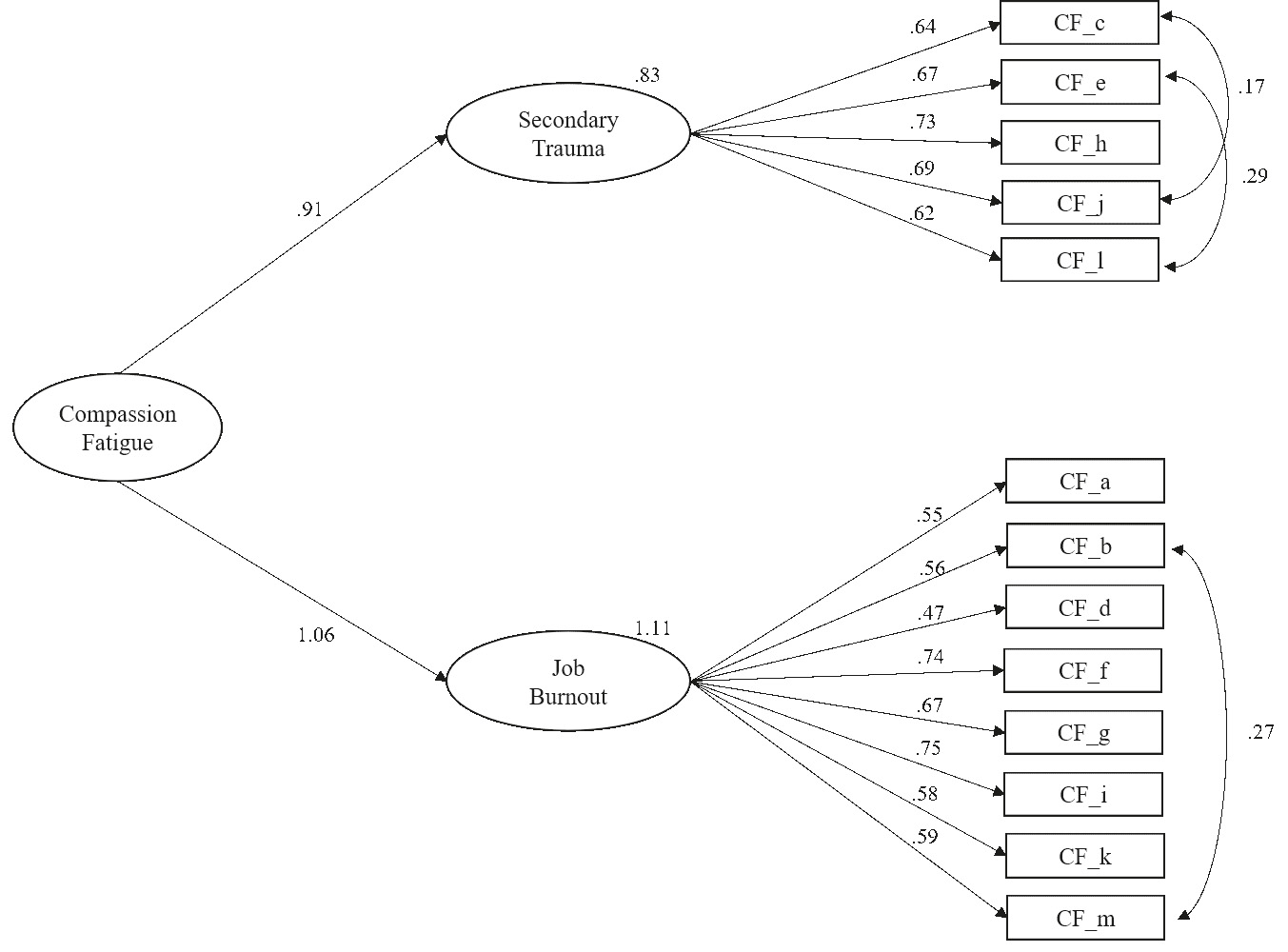
In this modified model, all standardized factor loadings of the item parcels were statistically significant, ranging from .620 to .729 for the ST dimension and from .474 to .746 for the JB dimension, showing that question items were good indicators for each first-order latent factor (p<.001). All the first-order factors loaded significantly on the second-order factor (CF). The constrained structural weights from CF to ST and JB were high (ƴ=.909, ƴ=1.055, p<.001, respectively).
Internal consistency and composite reliability
To examine the reliability of the scores on the final model, we used Cronbach’s alpha coefficient and composite reliability. Good internal consistency was obtained in the higher-order construct (α=.892). More specifically, ST and JB presented alpha values of .805 and .831, respectively. Composite reliability coefficients assumed values of 0.803 and 0.831, for factors with content related to ST and JB, respectively. Inter-correlations among all items were significant and no multicollinearity was obtained (.185≤r≤.585).
Convergent and discriminant validity
The Portuguese version of the Pt-CF-Short Scale was compared to other self-report measures (see Table 2). The CF scale and ST and JB subscales correlated positively, moderately, and significantly, with the K10, with the subscales anxiety, depression, and interpersonal sensitivity of BSI, with the IES-R and the TAS-20. Regarding the IRI, all subscales had a low, significant correlation with the CF scale and ST and JB subscales, except for the perspective-taking subscale. Moderate to low negative but significant correlations were found between CF total and its subscales and all dimensions of the WHOQOOL-Bref.
Table 2 Convergent validity: Spearman’s correlations between the K10, BSI dimensions, IES-R, TAS-20, IRI and WHOQOOL-Bref
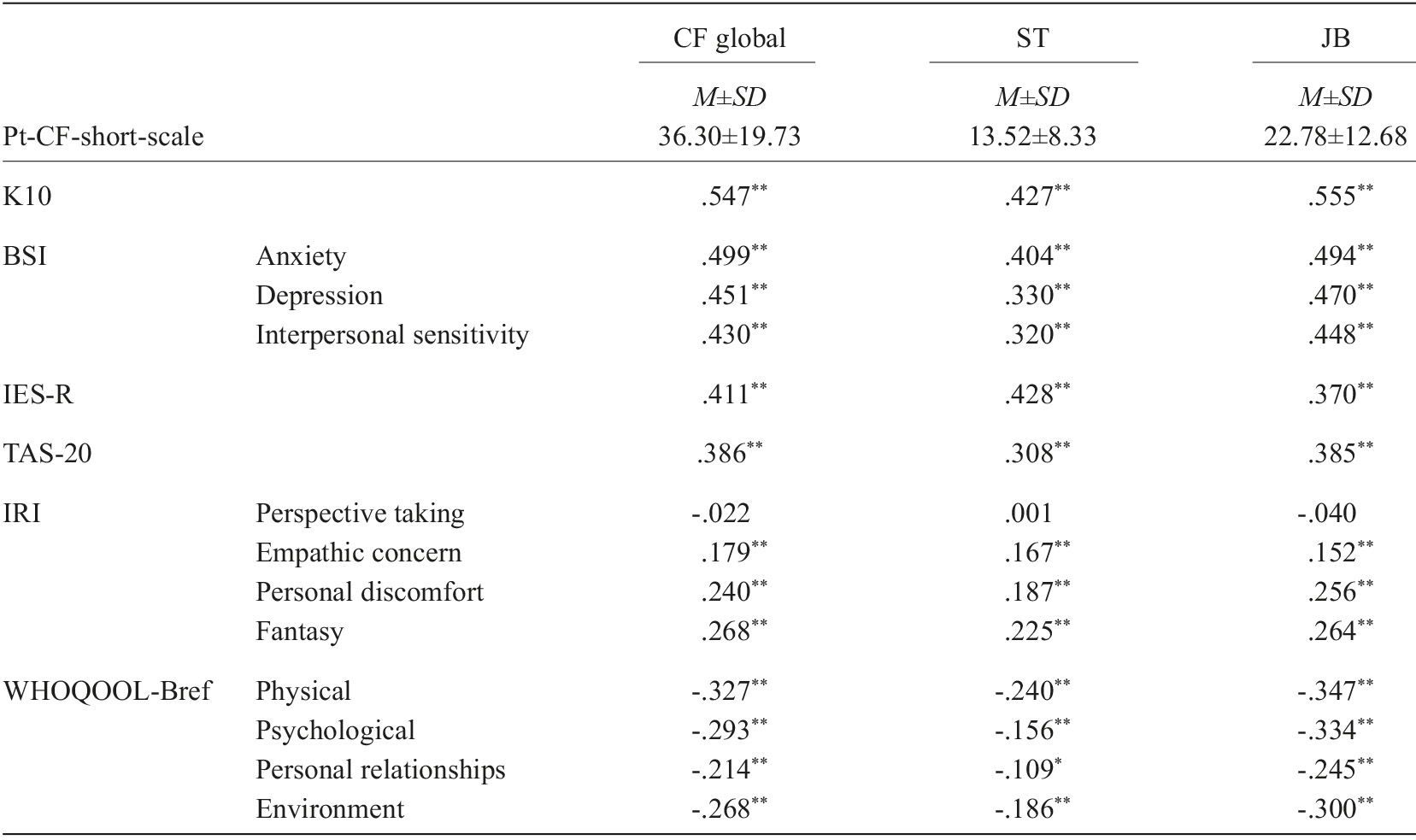
Note. K10=Kessler Psychological Distress Scale; BSI=Brief Symptom Inventory; IES-R=Impact of Event Scale-Revised; TAS-20=Toronto Alexithymia Scale; IRI=Interpersonal Reactivity Index; WHOQOOL-Bref=World Health Organization Quality of Life-Bref; ST=Secondary Trauma; JB=Job Burnout; M=Mean; SD=Standard Deviation; **p<.01; *p<.05.
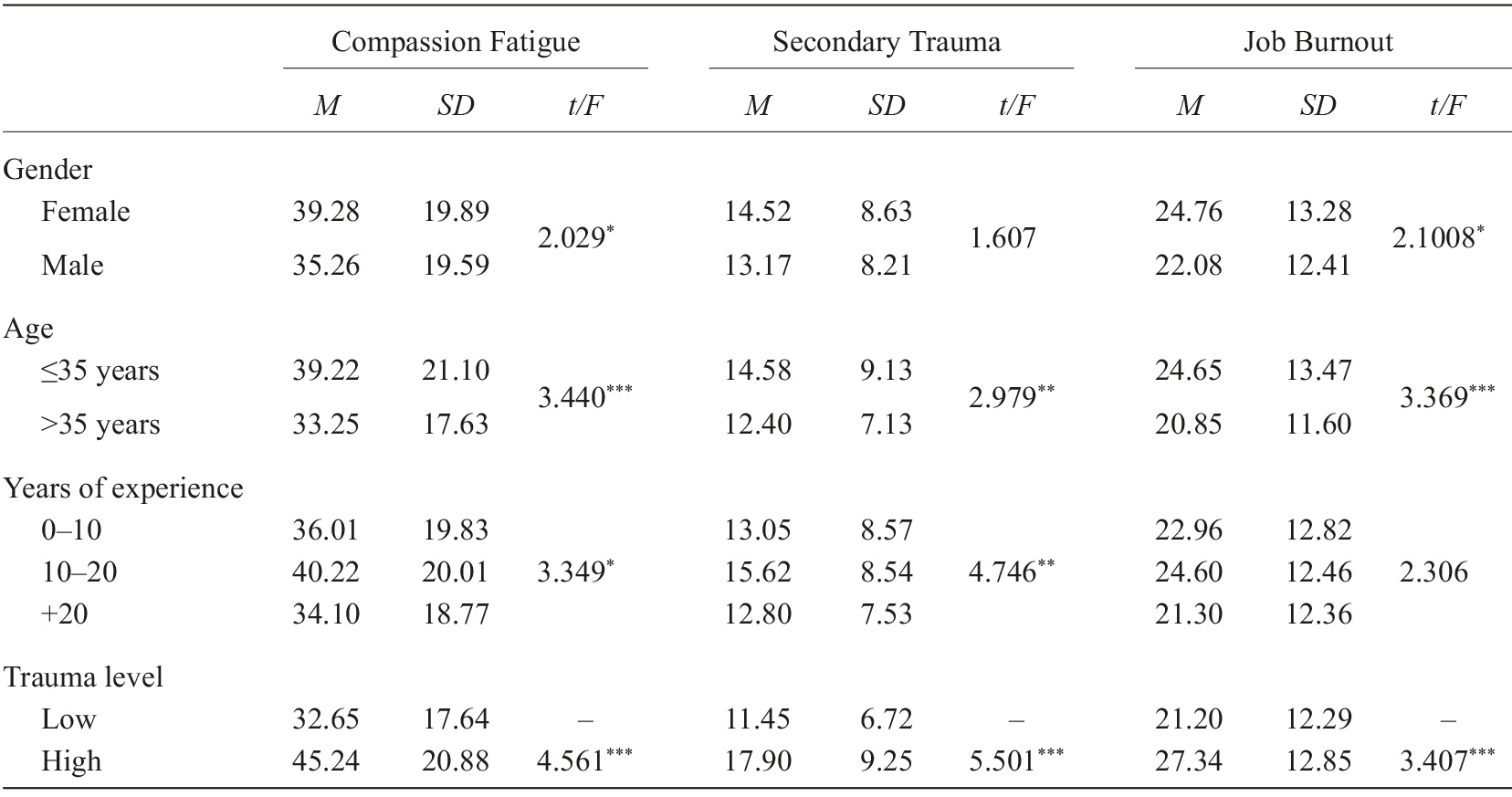
Concerning the domains of this scale, there were differences in CF scores between groups considering sociodemographic characteristics. Women had significantly higher mean levels of CF and JB than men. Firefighters under the age of 35 had significantly higher scores in all domains of CF than older firefighters. People between 10 and 20 years of work experienced more CF and ST, followed by those with little experience and those with more than 20 years as a firefighter, who registered the lowest CF. We observed that a higher perception of trauma is related to higher scores in all dimensions of CF and that these differ significantly from those who perceived a low level of trauma, who showed a lower score in all domains of CF. Table 3 presents the results from these analyses, which show that adequate discriminant validity was obtained.
Discussion
Emergency and crisis professionals are deployed to assist individuals affected by traumatic events, and these responders may experience the harmful effects of indirect trauma exposure. CF is one of these harmful effects, which lessens firefighters’ ability to fulfill their role as trauma responders and may even compromise their physical, psychological, and emotional health (Gleichgerrcht & Decety, 2013). Therefore, caring for others can result in frustration and helplessness, often causing professionals to dissociate from their own emotions.
Our data using 512 firefighters showed that the Portuguese version of the Pt-CF-Short Scale is a valid tool to assess CF in this population. Our comprehensive approach confirmed the strong construct validity of this version. This research showed that neither the one-factor nor the two-factor solutions were adequate for the Portuguese version of the CF-short scale administered to Portuguese firefighters. However, the second-order factor model, allowing covariance of errors, with two first-order factors, ST and JB, presented a good fit. The items were good indicators for each first-order latent factor. The standardized factor loadings were higher considering ST and JB as latent factors. Our findings proposed a modified model as a conceptually justified solution. Items e and l are related to sleep problems due to traumatic experiences and, for this reason, is acceptable to allow their correlation. Similarly, items b and m are both associated with beliefs of inefficacy/inutility.
Concerning convergent validity, correlations between the CF indices and other scales reinforced the convergent validity of the measure. Several studies point to positive correlations with psychological distress, depression, anxiety, and interpersonal problems and negative correlations with quality of life and well-being (Adams et al., 2006, 2008; Beaumont et al., 2016; Figley, 1995, 2002a; Miller & Mcgowen, 2000; Sonneck & Wagner, 1996). Among them, anxiety showed the highest moderate association with the CF dimensions. Also, CF and subscales are associated with the scales of trauma (IES-R) and alexithymia (TAS-20) (Gleichgerrcht & Decety, 2013). Nevertheless, the empathy scale (IRI) and its subscales showed only a low association with the CF scale and its subscales (and for the perspective-taking subscale, this association was not significant).
If the healthcare professionals is unable to differentiate their feelings, from feelings their patients, can be result in ties and confused roles, and exposure to suffering, and distress. The distress is associated with negative cognitions and negative mood, and this condition gives rise to the risk of secondary traumatization (Hannah & Woolgar, 2018; Mento et al., 2016; Settineri et al., 2018). Conversely, personality traits involved in emotional regulation, such as alexithymia and empathy, still deserve investigation. Alexithymic subjects display difficult interactions with others, including interpersonal ambivalence, poor sociability and the need for social approval and alexithymia is associated with negative affective states, especially depression and anxiety (Franco et al., 2020; Hiirola et al., 2017). This can potentially affect the performance at work, particularly in the emergency professions, leading to a decreased individual satisfaction and increased burnout susceptibility. It is not surprising that alexithymia is linked to deficits in empathy, defined as the ability to share and understand another’s state-of-mind/intention or emotion. In the healthcare environment, effective emphatic communication can enhance the therapeutic effectiveness of the clinician-patient relationship (Hiirola et al., 2017).
In terms of discriminant validity, as found in our results, previous research also suggested that women are more susceptible to CF than men, and experience more burnout (Beaumont et al., 2016; Gonzalez et al., 2019; Sun et al., 2016; Turgoose & Maddox, 2017) although women are more able to use coping strategies to reduce burnout (Gonzalez et al., 2019). Studies also indicate that more ample professional experience was associated with lower CF (Thomas & Otis, 2010; Thompson et al., 2014). One of the explanations is related to the most experienced individuals being in supervisory roles and, therefore, less directly exposed to clients’ trauma. It is also likely that those with more experience deal with more cases of the most challenging, than those less experienced. So, it is possible that, with their experience, they have learned more effective ways of coping and are then not as likely to develop CF (Turgoose & Maddox, 2017). CF tends to decrease with age (Cohen et al., 2006; Thomas & Otis, 2010), with younger professionals being more likely to report it (Sprang et al., 2011). Here, we can reasonably assume that age is directly associated with the length of professional experience. However, experienced firefighters who deal with rescue operations need a great deal of resources since they are exposed to different kinds of traumatic experiences such as traffic accidents, building collapses, natural disasters, and others. Also, their vacation time may be shortened. Thus, CF may contribute to the subsequent depletion of their internal resources, decreased performance, and negative health outcomes such as psychological distress, anxiety, depression, and somatic complaints (Beaumont et al., 2016; Sun et al., 2016).
This study proposes the European Portuguese version of the CF-short scale as a valid and reliable tool to assess CF among firefighters. Our comprehensive approach to validation of the CF-Short Scale goes beyond other validation studies developed with Western (Dinç & Ekinci, 2019) or non-Western (Sun et al., 2016) samples of emergency professionals, which mainly focus on the measure’s operating characteristics. This study examines the dimensional structure of the measure, specifically in the population of firefighters.
Thus, our findings suggest the importance for psychologists and researchers of using the Pt-CF-Short Scale as an instrument. For a better conceptual understanding of CF, they must consider the ST and JB dimensions as consistent indicators of CF. An assessment using this instrument may allow identification of CF levels in this population, specifically to know the risk of secondary trauma and job burnout, and allow the design of proper treatment. This view of the broad clinical domains reported by firefighters may lead to better clinical judgment than a single CF score derived from the CF total scale.
Even though these critical incident responders do not experience trauma directly, their indirect exposure can often lead to CF and burnout (Figley, 2002a; Sprang et al., 2007), as well as inhibiting them from effectively assisting and care demanded by their profession (Badger et al., 2008; Boscarino et al., 2004). Ultimately, the positive psychological construct of compassion may enhance overall psychological well-being and significantly to diminish the experience of the negative psychological consequences of ST, such as CF and JB. Thus, actions from the professional training of these professionals should be included as well as psychological intervention or treatment must focus on coping strategies and the development of tools for trauma management and must be delivered to firefighters who face emergencies directly and those who respond indirectly to situations. Nevertheless, our conclusions should be interpreted cautiously since the underrepresented female firefighters limit them in the sample and the diversity of firefighter categories.
Future studies should include a more representative sample, with more women, to examine the factor structure of the Pt-CF-Short Scale. Although we know that less experience is related to more CF, there is no known association between CF and employees’ workload. This parameter was not assessed in this study but will be an interesting point to study in the future. A proposal for future studies may involve adapting and validation of the scale for other help professionals in Portugal, such as doctors, nurses, psychologists, etc.
In conclusion, the findings suggest that the Pt-CF-Short Scale has good psychometric properties and can be applied to study Portuguese emergency workers, especially firefighters, and can serve as a good tool for monitoring and managing the mental health of this emergency workers.