











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
Introduction
Aggression is a natural tendency that assists survival (Wrangham, 2019) and constitutes a protest against life hardships (Fonagy, 2003). In old age, aggression is a possible reaction to chronic conditions and adversities in life (Tilov et al., 2016), being more common and with a more significant impact among institutionalized older people (Léger et al., 2002). According to Buss and Perry (1992) and Bhardwaj et al. (2019), aggressiveness is a normal personality trait that represents the predisposition to express anger (emotional component), hostility (cognitive component), and involvement in physical or verbal aggression (behavioral component). Thus, aggressiveness is a personality trait that not only includes aggression as its behavioral dimension but also predisposes to aggression (Bhardwaj et al., 2019; Buss & Perry, 1992; Carli et al., 2014; Velotti et al., 2016).
In the course of aging, aggressiveness diminishes probably because changes in personality occur due to better emotional regulation and increased maturity (Daniel et al., 2019; Morales-Vives & Vigil-Colet, 2010, 2012). Although aggression is generally lower in old age, it is still a significant concern in institutional settings (Caspi, 2018; Lachs et al., 2007). Aggression in these settings is probably an indication of adaptation to institutionalization (Espirito Santo & Daniel, 2018) but could also result from a set of problems more prevalent in these contexts. All of these problems have been associated with aggressiveness and aggression (Gimm et al., 2016), such as dementia or cognitive impairment (Caspi, 2018; Lachs et al., 2007), severe depressive symptoms (Figueiredo-Duarte et al., 2021; Vicente et al., 2014), social exclusion (Twenge et al., 2001), reduced ability to perform activities of daily living (Daniel et al., 2019), or various contextual variables including territoriality (Kolanowski, 1995) and low levels of physical and cognitive activity (Daniel et al., 2019). In the Portuguese context, the results of interviews with care-home managers and care staff in institutional settings showed a bleak scenario: aggressive incidents (physical and verbal) take place daily between residents or groups of residents, and these incidents were common among residents without and with dementia (Ferreira et al., 2019).
A challenge for research in aggression and aggressiveness is understanding the key role of impulsivity. Impulsivity is a trait disposition to display spontaneous, non-planned, reckless, and potentially dangerous behaviors (Carli et al., 2014; Velotti et al., 2016). It has a strong relationship with aggressive behavior, is supposed to be an antecedent to aggression (Velotti et al., 2016), and overlaps with aggressiveness as a trait disposition towards aggression (Carli et al., 2014). Although problems with elevated impulsivity are more prevalent in adolescence-young adults and forensic populations (Carli et al., 2014; Velotti et al., 2016), to date, there is minimal research linking impulsivity with aggressiveness in older adults. However, one study Morales-Vives & Vigil-Colet, 2012) revealed that older adults have higher levels of dysfunctional impulsivity than younger adults, consistent with inhibition deficits.
Alexithymia is another key factor in understanding aggressiveness (Velotti et al., 2016). Alexithymia is a personality dimension expressed by the inability to describe and identify emotions and feelings of oneself or others (Sifneos, 1973). Due to this inability, emotional arousal problems arise, especially with stressful events and threatening situations (Velotti et al., 2016). Alexithymia is related to and predicts impulsiveness (Velotti et al., 2016). Higher levels of alexithymia are reported in old age (Mattila et al., 2006; Onor et al., 2010), mainly when cognitive impairment is present (Onor et al., 2010).
Notwithstanding its importance, research addressing the relationship between aggression, alexithymia, and impulsivity in older people is lacking. Moreover, as far as we know, there is no research concerning institutionalized older people. However, given the common occurrence of aggression in older people care homes and the threat to caregivers and other residents alike (Caspi, 2018; Ferreira et al., 2019; Lachs et al., 2007), the research on aggressiveness factors is potentially helpful in outlining adequate intervention strategies. Therefore, this study aimed to explore the influence of impulsivity and alexithymia in institutionalized older adults’ aggressiveness, considering different sociodemographic and clinical control variables. Specifically, we hypothesized that impulsiveness and alexithymia predict aggressiveness in older adults. Of note that, although we use the term ‘prediction’ and this term is commonly used in cross-sectional analyses (Hayes, 2018), we do not intend to establish a causal or temporal relationship.
Methods
Procedures and participants
Eligibility criteria for inclusion in the study included age above 60 years, the cognitive ability to understand the assessment instructions, and signing informed consent. Older adults with an identified severe neurocognitive disease, severe cognitive impairment, and/or a diagnosis of a severe organic disorder hindering their evaluation were excluded from the study.
Trained psychologists assessed volunteering participants, reading out the written informed consent and the assessment questionnaires to all participants. The questionnaires were administered individually during one or two sessions. Sociodemographic and clinical characteristics were confirmed in the medical/nursing records. For reliability analysis of some measures, we re-assessed 25 participants over one month. The study took place between October 2019 and March 2020 in the Central region of Portugal.
A pre-analysis of statistical power (G*Power software; https://bit.ly/3FZArXO, accessed October 2019) revealed that an adequate sample size to detect medium effects (w=0.3; d=0.5; f=0.25; r=0.5), a power >.80, with alpha=.05 for the respective statistical tests (chi-square, t-test, ANOVA, correlation, and regression analyses) should be over 102 subjects. Seventy-three older adults were not included in the study due to severe disease or impairment (based on participants’ clinical records, researchers’ assessment, and answers to a Sociodemographic and Clinical Data Questionnaire). Furthermore, although they were assessed, 20 subjects receiving home support were not included in the study, considering that it was not the context focused on by our research. Thus, the total sample (Table 1) included 97 institutionalized older adults (60-94 years, M±SD=81.49±7.73). This sample size allowed a statistical power >.80 except for Student’s t-test (β=75%).
Table 1 Sociodemographic and clinical characteristics and differences in the BPAQ-SF in a sample of institutionalized older adults
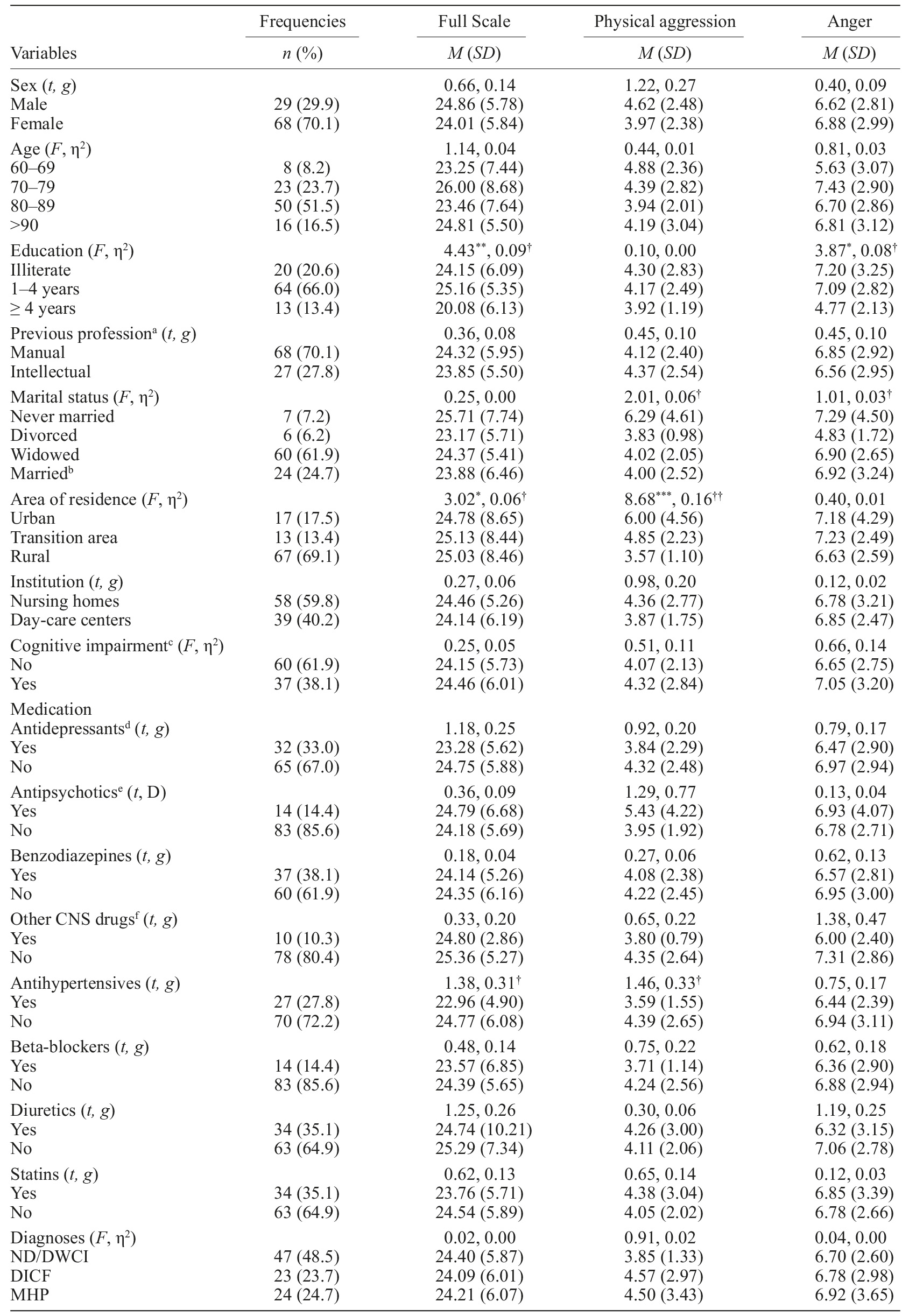
Note. N=97. BPAQ-SF=Buss-Perry Aggression Questionnaire - Short Form; CNS=central nervous system; DICF=Disease with an impact on cognitive functioning; ND/DWCI=No mental/neurological diagnosed diseases nor physical illness involving cognitive impairment. a N=95. Some participants only indicated that they were retired; bMarried or living with someone as if married; cAccording to Mini-Mental State Examination cutoff points. Although impaired, older adults presented cognitive ability to understand the study; dInclude all classes; eConventional and atypical; fAntiepileptics and antiparkinson’s drugs. ***p<.001; **p<.01; *p<.05. ††Medium effect size. †Small effect size.
The duration of institutionalization was 34.13 (SD=57.59 months), and older people were recruited from nursing homes (59.8%) and day-care centers (40.2%) - all private organizations subsidized by the Portuguese government.
Instruments
In addition to a Sociodemographic and Clinical Data Questionnaire, the current study incorporated the following measures:
Buss-Perry Aggression Questionnaire - Short Form (BPAQ-SF; Bryant & Smith, 2001; Simões, 1993) is a 12-item Likert scale ranging from 1 (never) to 5 (always) that assesses physical and verbal aggression, anger, and hostility. The full scale of scores ranges from 12 to 60 (higher aggression), and its subscales range between 3 and 15. In the previous validation studies, BPAQ-SF Cronbach’s alpha varied between .68 and .86 (Bryant & Smith, 2001) and .89 (Simões, 1993). Given the reliability values in this study, we used the full scale, physical aggression (BPAQ-SF-PA), and anger (BPAQ-SF-A) subscales (psychometric properties in Table 2). The other two subscales presented unacceptable reliability values (Cronbach’s αverbal aggression=.66; Cronbach’s αhostility =.49).
Table 2 Descriptive statistics and psychometric properties for study variables
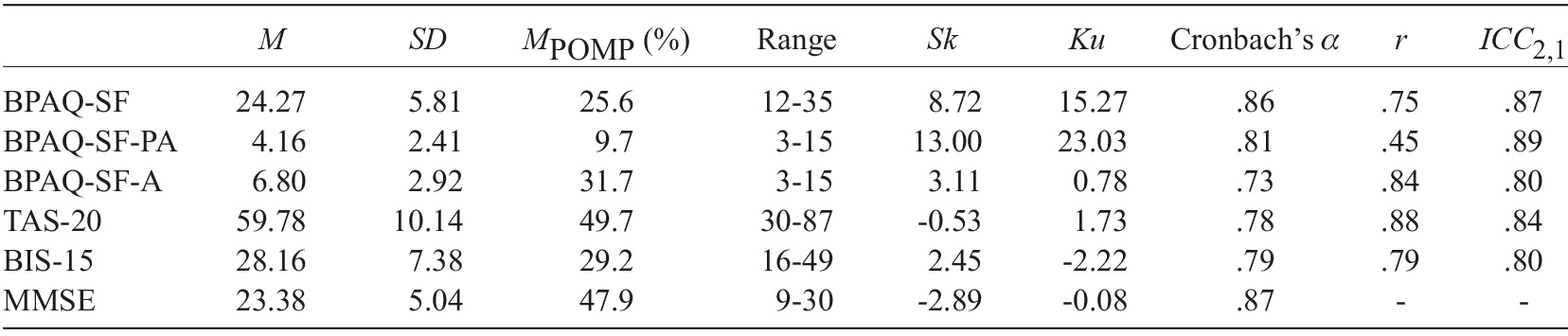
Note. N=97. BPAQ-SF=Buss-Perry Aggression Questionnaire - Short Form; BPAQ-SF-PA=BPAQ-SF physical aggression; BPAQ-SF-A=BPAQ-SF anger; TAS-20=Toronto Alexithymia Scale; BIS-15=Barratt’s Impulsiveness Scale; MPOMP=percent of the maximum possible: (M - minimum possible score)/(maximum possible score - minimum possible score)x100. Sk=Skewness; Ku=Kurtosis; r=Test-retest reliability correlation; ICC 2,1=Intraclasse correlation coefficient with the same set of tests.
Twenty-Item Toronto Alexithymia Scale (TAS-20; Bagby et al., 1994; Praceres et al., 2000) assesses alexithymic features through 20 items answered on a five-point Likert scale from 1 (completely disagree) to 5 (completely agree). The total score interval is 20-100 (more alexithymia). Internal consistency reliability was 0.81 in the original study (Bagby et al., 1994), .79 in the Portuguese validation, and .78 for the present study (Table 2).
Barratt’s Impulsiveness Scale-15 items (BIS-15; Spinella, 2007) comprises 15 items on a four-point Likert scale from 1 (never or seldom) to 4 (almost always/always), measuring attentional, motor, and non-planning impulsivity. Scores range from 15 to 60 (higher impulsivity). BIS-15 was adapted for this study following the International Test Commission (2017) guidelines: (1) an English fluent speaker translated the original BIS-15 items to Portuguese; (2) another team member, fluent in both languages, independently back-translated to English; (3) the remaining research team members compared the translated and back-translated versions, checking item’s content equivalence, and minimal revisions were made; (4) the final version was pretested on six older adults who reported no difficulties regarding items’ clarity and comprehensibility. BIS-15’s internal consistency and test-retest reliability were both .79, and ICC 2,1 was .80. In its original abbreviated version, Cronbach’s alpha was also .79 (Spinella, 2007).
Mini-Mental State Examination (MMSE; Folstein et al., 1975; Guerreiro et al., 1994) includes 30 questions assessing six areas of cognitive ability for a maximal score of 30 points. Depending on the education level, scores less than 27 (>11 years of education), 22 (1-11 years of education), or 15 points (illiteracy) indicate cognitive impairment (Santana et al., 2016)].
Statistical analysis
We used the IBM SPSS Statistics 26 software. Preliminarily, instruments’ reliability was analyzed, considering a Cronbach’s alpha of .70 as the minimum acceptable, and Pearson correlation and intraclass correlation coefficients (ICC) were used to determine test-retest reliability.
Next, descriptive statistics (means, standard deviations, and frequencies) were applied to expound the sample and study variables. Scores of study variables were then converted into the percent of the maximum possible, according to Cohen et al. (2010). Their equation allows for direct comparisons of scores of instruments assessing the same construct of previous research: M POMP=(M - minimum possible score)/(maximum possible score - minimum possible score)x100.
Student’s t-tests for independent samples and analyses of variance (ANOVA) were applied to detect potential differences in study variables between participants categorized according to sociodemographic and clinical variables. Pearson correlation coefficients were computed to assess the relationship between predictors (TAS-20; BIS-15) and the outcome variables (BPAQ-SF, BPAQ-SF-PA, and BPAQ-SF-A). A hierarchical multiple regression method was used to examine the models’ ability to predict levels of general aggressiveness, physical aggression, and anger beyond relevant demographic covariates and clinical variables. An assumption check on outliers, normality, and multicollinearity was performed for these predictive analyses. Sociodemographic and clinical covariates were chosen based on mathematical results and entered as a control in Block 1, followed by TAS-20 and BIS-15 in Block 2.
Hedge’s g, Cohen’s d, or Glass’s delta was used to assess the Student’s t effect size according to Cohen’s (1988) criteria (0.20-0.49 small, 0.50-0.79 moderate, 0.80-1.29 high). Eta-squared (η2) was calculated to assess the analysis of variance effect size, also following Cohen’s (1988) criteria (.02-.12 small, .13-.25 medium, ≥.26 large). Finally, the coefficient of determination was calculated for the correlational analysis (r 2 x100). Regarding predictive analyses, the R 2 change (ΔR 2) was used to indicate the variance of the outcome variable explained in each block. Within each block, the standardized regression weights were presented to indicate the relative contribution of individual predictors.
Results
Preliminary analysis
Scores distribution analysis and of the study variables showed non-normal distributions for BPAQ-SF and BPAQ-SF-PA (Table 2). Other descriptive statistics are presented in Table 2. According to MMSE cut-off scores, 37 older adults had cognitive impairment (38.1%).
Sociodemographic and clinical differences in the BPAQ-SF
Table 1 also shows sociodemographic and clinical differences in BPAQ-SF and its subscales scores. The only statistically significant differences were found in BPAQ-SF according to the residency area and educational levels and in BPAQ-SF-PA according to the residency area.
Correlations Between the BPAQ-SF, TAS-20, and BIS-15
For Pearson correlations analysis, given the presence of outliers in study variables, we changed values to less extreme values (BPAQ-SF-A, TAS-20, and BIS-15) or transformed the variable as a remedy for both the presence of outliers and severe violation of normality (BPAQ-SF-PA) according to Tabachnick and Fidell’s suggestion (2014). Hence, BPAQ-SF and its subscales correlated positively with TAS-20 (R 2 between 4.4-17.8%) and BIS-15 (R 2 between 9.0-17.8%). Other correlations are presented in Table 3.
Table 3 Pearson correlations among study variables
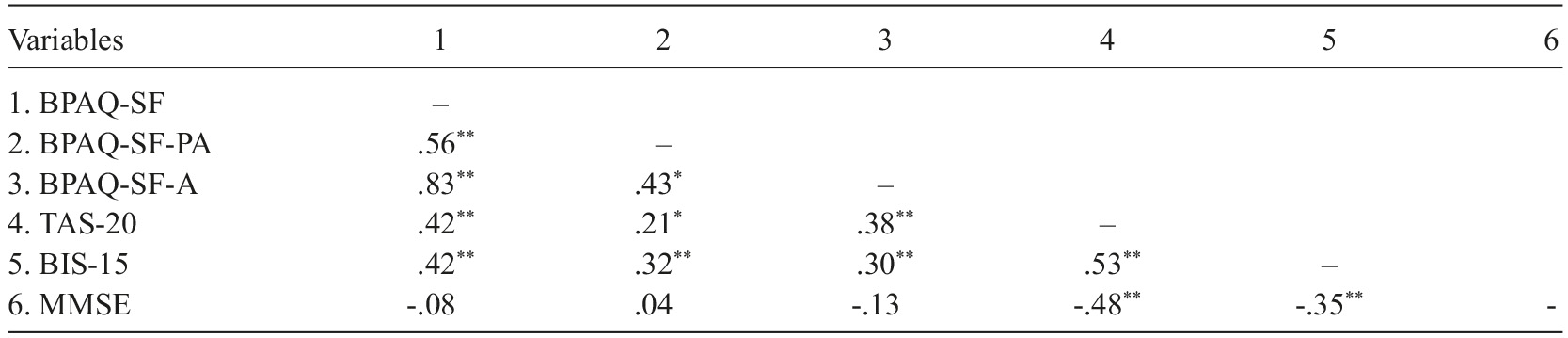
Note. N=97. BPAQ-SF=Buss-Perry Aggression Questionnaire - Short Form; BPAQ-SF-PA=BPAQ-SF physical aggression; BPAQ-SF-A=BPAQ-SF anger; TAS-20=Toronto Alexithymia Scale; BIS-15=Barratt’s Impulsiveness Scale; MMSE=Mini-Mental State Examination. **p<.01; *p<.05.
Predictors of reported aggressiveness, physical aggression, and anger
Preliminarily, to ensure data was suitable for regression analyses, collinearity diagnostics showed no issues among the control variable and the predictors (tolerance>0.01, VIF<10). Normality was tested by histograms and Q-Q plots of residuals and was found to be acceptable. No outliers were detected in the scatterplots of the standardized residuals, and Mahalanobis distance values (BPAQ-SF: 0.48-10.84; BPAQ-SF-PA: 0.55-9.82; BPAQ-SF-A: 0.02-8.28) were under the critical value (Tabachnick & Fidell, 2014). Cook’s Distance values were very low (BPAQ-SF: 0.00-0.11; BPAQ-SF-PA: 0.00-0.10; BPAQ-A: 0.00-0.10), indicating few points with undue influence.
Regarding BPAQ-SF, given preceding analyses, area of residence and educational level were entered at the first step as control variables (Table 4). They explained 5.5% of the total variance of BPAQ-SF scores [F (1,94)=0.91, p=.070]. Given Velotti et al. (2016) findings, in a second step, TAS-20 was entered as the first predictor of BPAQ-SF scores: the total variance explained by the model as a whole was 18.1% [F (3,93)=6.86; p<.001] and the beta value was statistically significant (Table 4). Then BIS-15 was entered in a third step, explaining 24.6% of the total variance with a statistically significant and higher standardized beta coefficient (Table 4).
Table 4 Predictors of aggressiveness, physical aggression, and anger (BPAQ-SF) in an institutionalized older adults sample
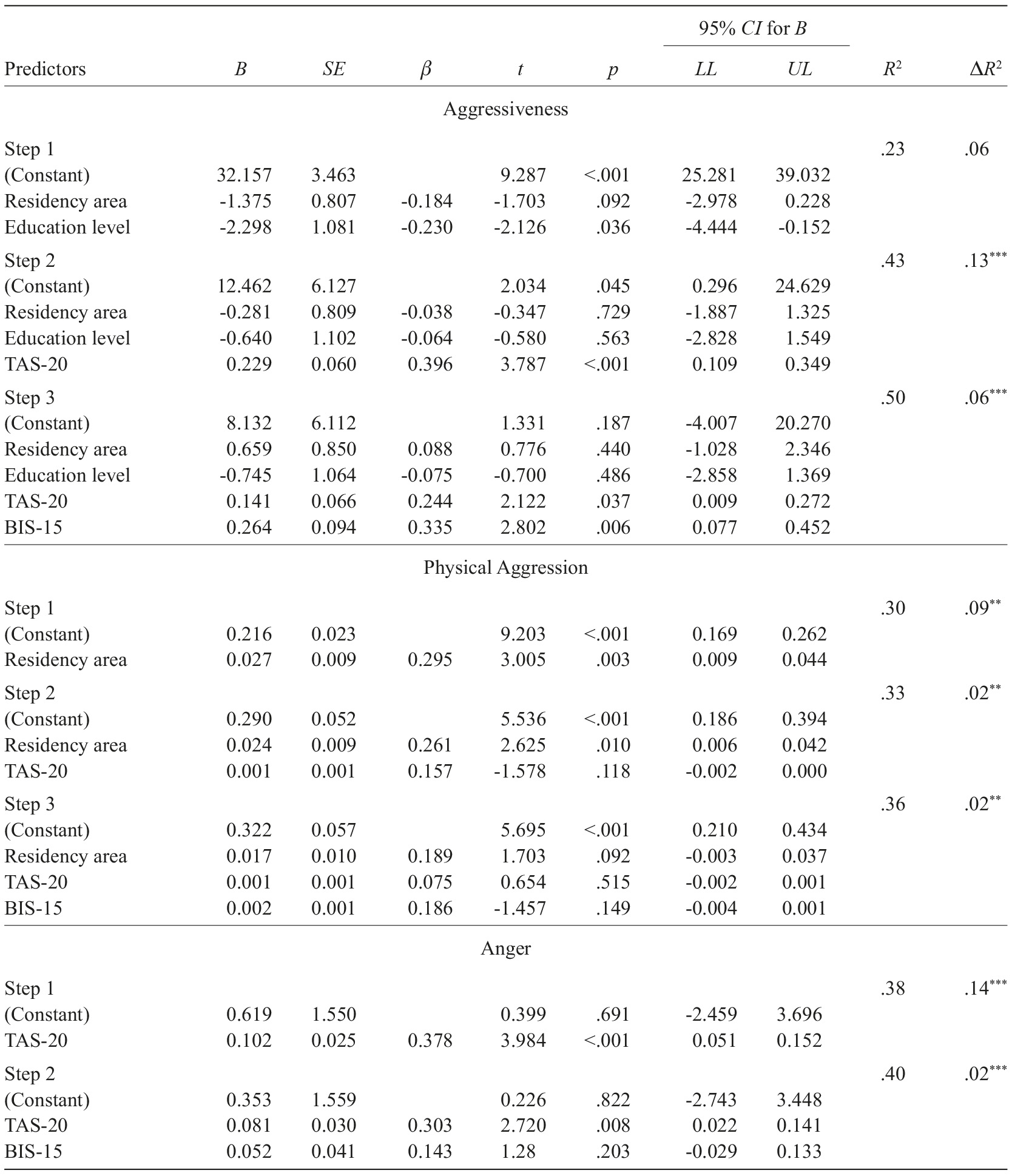
Note. N=97. BIS-15=Barratt’s Impulsiveness Scale; BPAQ-SF=Buss-Perry Aggression Questionnaire - Short Form; TAS-20=Toronto Alexithymia Scale; LL=Lower limit; UL=Upper limit.
In what concerns BPAQ-SF-PA, the area of residence explained 8.7% of its total variance [F (1,95)=9.03, p<.01]. After controlling for its effect, the model as a whole with TAS-20 as predictors explained 11.0% of the total variance [F (3,94)=5.83; p<.01], but its beta value was not significant. In the next step, BIS-15 explained 13.0% of the total variance with an also non-significant beta value (Table 4).
TAS-20 was the only predictor of BPAQ-SF-A (Table 4), explaining 14.3% of its variance, with the full model containing the two predictors being statistically significant [F (1,94)=8.81, p<.001].
Discussion
Previous research showed that both alexithymia and impulsivity play an important role in aggressive behavior. Although aggressiveness is less common in older adults, it is an essential aspect that lacks research compared to other age groups (Morales-Vives & Vigil-Colet, 2012). Regarding older adults, aggressive behavior might also be associated with neuronal degeneration and functional limitations, which could then possibly be linked to maladaptation to chronic conditions and life adversities (Caspi, 2018; Tilov et al., 2016). This study examined the predictive role of impulsiveness and alexithymia on institutionalized older adults’ aggressiveness while controlling for the sociodemographic variable that was shown to be relevant.
Reported aggressiveness levels were lower than those revealed in other studies with community older people (Morales-Vives & Vigil-Colet, 2010: M POMP=30.6%), with adults from the community (M age=36.88) and psychiatric (M age=43.89) (Velotti et al. 2016: M POMP=30.6%; 44.4%), with young adults from the community (Buss, 1992: M POMP=30.6%-36.0%), and another study involving psychiatric inpatients (De Schutter et al., 2016: 32.6%). The fact that our older adults have lower levels of aggression than younger people, including psychiatric patients, is in line with findings that aggression decreases with aging (Morales-Vives & Vigil-Colet, 2010, 2012). However, it is unanticipated that the levels of aggressiveness noted in our study are lower than that reported in community-dwelling older adults; more so as other studies pointed out that aggression is common among institutionalized older people (Caspi, 2018; Ferreira et al., 2019; Lachs et al., 2007; Léger et al., 2002). Moreover, our result is surprising considering that in institutionalized contexts, it is more likely to find high levels of symptoms of depression (Figueiredo-Duarte et al., 2021; Vicente et al., 2014), more functional impairments (Daniel et al., 2019), more cognitive impairment or dementia (Caspi, 2018; Lachs et al., 2007). All these aspects have been linked to aggression (Gimm et al., 2016). Perhaps this finding can be better explained by sample characteristics (e.g., high levels of medication in the institutional context), situational variables (more supervision), specific health status (more frailty; Daniel et al., 2019), or social desirability. Reinforcing the social desirability hypothesis is the percentage of the maximum possible found for physical aggression (an externalized component of aggression), which was much lower than that for anger which is an internalized phenomenon and, therefore, potentially more accepted by the self. Considering the number of aggressive incidents reported by Ferreira et al. (2019) in institutional settings, the discrepancy between physical aggression reported by older people and what is observed strengthens the social desirability hypothesis. Our institutionalized older adults indicated higher levels of alexithymia compared to another study with community older adults (Onor et al., 2010; M POMP=21.3%). However, Onor et al.’s (2010) study, the mean age was much lower (M=64.4; SD=7.4), and they excluded older adults with even very mild cognitive impairment. Thus, by including older adults also with cognitive impairment (only excluding those with severe impairment), our result seems to confirm the link between alexithymia and cognitive impairment explored in other studies (Mattila et al., 2006; Onor et al., 2010). This link was also found in our study. However, the higher levels of alexithymia do not explain why aggressiveness was low in our study, pointing to the other explanation possibilities indicated above. An additional explanation is the common use of several drugs in institutional settings (De Fazio et al., 2014). The sedation resulting from the combination of drugs (Gillies et al., 2013) could explain the low levels of physical aggression and high levels of difficulties in identifying and verbalizing feelings and emotions. The impulsivity level was comparable to the values reported by Morales-Vives and Vigil-Colet (2012: M POMP=32.8%). Their study involved a similar sample (Mage=77.2) partially recruited from Spanish “retirement homes” but also from “senior community centers”. Both theirs and our impulsivity levels are slightly higher than those reported in a few younger samples (Morales-Vives & Vigil-Colet, 2012: MPOMP between 21.3%-29.0%). Higher impulsivity does not explain why levels of aggressiveness (especially physical aggression) are low because both phenomena are related, and the medication should also reduce impulsiveness (Gillies et al., 2013). Since the BIS-15 includes items that assess non-planning impulsivity and that people in an institution are not given much chance to plan, the slightly high values on the scale may stem from this aspect.
Regarding sociodemographic differences, there was no difference between sexes in aggressiveness as in previous studies and per the sexual selection theory (Morales-Vives & Vigil-Colet, 2010, 2012) (Morales-Vives & Vigil-Colet, 2010, 2012). However, this could be more true in the institutional context because older people do the same basic activities and cease to perform activities related to the stereotypical gender roles. Therefore, the traditional gender gap is probably narrowed among older institutionalized people; consequently, differences in aggression may decline. Age showed no significant relationship with reported aggression, denoting that aggression levels are stable throughout age groups among institutionalized older people. This result is somewhat surprising given that the abovementioned aspects linked to aggression problems are more likely present in institutionalized contexts with the oldest-olds (Caspi, 2018; Daniel et al., 2019; Lachs et al., 2007; Vicente et al., 2014). Furthermore, we have involved older adults with diseases that impact cognitive functioning; consequently, older adults should have higher reported aggressiveness (Caspi, 2018; Lachs et al., 2007). However, according to the sexual selection theory (Archer, 2009), the competition for reproduction and physical fitness in old age is generally lower than in other age groups, resulting in similar aggressiveness levels over the years (Morales-Vives & Vigil-Colet, 2010, 2012). Aggressive levels did not differ between marital status, but regardless of their marital status, they are in an institution, share similar aggression-related problems (Caspi, 2018; Daniel et al., 2019; Lachs et al., 2007; Vicente et al., 2014), and are about the same age. The only sociodemographic variable associated with aggressiveness was the area of residence. We can only assume that this result might be due to stressors experienced in daily life in cities that modulate how older adults relate to others during their lives. Another possible explanation is that city life can affect staff members’ stress levels, affecting their interaction with older people and contributing to higher levels of aggression among them. Regarding medication, we expected to see a correlation between aggressiveness and antipsychotic drugs, benzodiazepines (Gillies et al., 2013), and antidepressants (Bond, 2005) since these are commonly used in institutionalized older adults (De Fazio et al., 2014). Again, having similar aggression-related problems (Caspi, 2018; Daniel et al., 2019; Lachs et al., 2007; Vicente et al., 2014) and being about the same age could explain the results.
Aggressiveness, alexithymia, and impulsiveness were linked as expected (de Schutter et al., 2016; Velotti et al., 2016) with medium, positive correlations between the BPAQ-SF and the other two study variables. In the De Schutter et al. (2016) study, there was no correlation between aggression and alexithymia, and the correlation between aggression and impulsivity was higher (R 2 =17.6%). However, De Schutter et al.’s (2016) studied younger participants (M age =37.5). In Velotti et al.’s (2016) study, also with younger participants (M age =36.88), the BPAQ-SF shared variance with alexithymia was lower (R 2 =15.2%) and with impulsivity was higher (R 2 =16.8%). This data seems to fit the previously postulated idea that alexithymia’s relationship with aggressiveness is higher throughout the aging process, explainable by the deterioration of cognitive abilities.
Additionally, aggressiveness was not correlated with MMSE scores, which could be explained by excluding older adults with severe cognitive impairment and having only 38% of older adults with cognitive impairment. This non-correlation seems to contradict the above postulated idea that aging strengthens the alexithymia-aggressiveness relationship. However, a correlation between BPAQ-SF and MMSE would probably occur if the sample included adult people younger than 60 and people with worse cognitive functioning (hence greater heterogeneity in MMSE scores).
Consistent with our starting hypothesis, alexithymia and impulsiveness predicted reported aggressiveness. This result adds to what was found in Veloti et al.’s (2016) study with a psychiatric and younger community sample. Thus, the idea that poor awareness of emotions and a diminished ability to think and talk about feelings (alexithymia) is a mechanism that precedes aggression is reinforced. It also underpins the idea that people with a tendency to act spontaneously, unplanned and unthinking (impulsivity) will likely fail to inhibit aggressive tendencies, most likely because they are in the context of institutionalization. Potentially threatening and painful situations tend to trigger negative emotional arousal (Bousardt et al., 2016). Institutions can be categorized as such due to issues related to territoriality: disputes due to invasions of personal space or competition for objects are commonly observed in these contexts (Kolanowski, 1995). However, why do alexithymia and impulsivity not predict physical aggression? One hypothesis will again have to do with age itself. Greater frailty is more frequent in the institutional setting (Daniel et al., 2019), likely preventing physical displays of aggression even if the older adult is alexithymic and/or impulsive. Anger was only predicted by alexithymia, with impulsivity not showing to be a predictor. This is an expected result, considering that anger is the emotional component of aggression. Hence, it is unsurprising that poor awareness and ability to think and talk about emotions predicts anger, and impulsivity does not.
Study limitations and research implications
The current study has some limitations that should be acknowledged. First, this is not a population-based study, and the sample does not represent the Central region population. Consequently, larger studies involving participants from other districts and regions must be conducted. Second, given the volunteer nature of participation, the reliability of the study may be affected because results may not be consistently reproduced. Third, in light of the relatively small number of subgroups’ participants, future studies should involve larger samples to provide more evidence. Fourth, though the analyses suggest causal relationships, the cross-sectional nature of our study cannot address causality. As such, future work should assess older adults at the time of institutionalization and plan follow-ups. Fifth, self-report measures may produce socially desirable responses, particularly regarding aggressiveness; thus, future studies should include social desirability in the statistical models and incorporate observational measures of physical and verbal aggression. Finally, future research should control the influence of the potential confounding role of emotional dysregulation (Velotti et al., 2016), depressive symptoms (Heeren et al., 2003), and other cognitive or interpersonal factors (Gómez-Leal et al., 2022).
Conclusion and clinical implications
Our sample reported low aggressiveness levels, consistent with the idea that it declines with aging but contradicting previous evidence pointing to more aggressive incidents in institutional settings. These levels derive mainly from the scores of physical aggressions. However, one should not overlook the possibility of a divergence between what older people indicate as physical aggression and what is observed. In fact, many older adults express that they feel anger, the emotional component of aggressiveness. Moreover, the role of medication in these settings should not also be ignored.
Furthermore, our study is consistent with previous studies analyzing the role of alexithymia and impulsiveness in aggressiveness. According to our findings, older people with high levels of poor awareness, poor ability to reflect upon emotions and feelings (alexithymia), and a high tendency to act spontaneously, unplanned, and unthinkingly (impulsivity) tend to be more aggressive. Thus, deficits in the awareness and ability to think about feelings could explain why some older adults are more prone not to control their impulses and, consequently, be more aggressive. This is consistent with the theory of mentalization (Fonagy, 2003). Therefore, understanding the mechanisms predicting aggressiveness is an important measure toward preventing or reducing this phenomenon, which would benefit victims, aggressors, and institutions.
Our findings reinforce the idea (Garofalo et al., 2018) that intervention programs aiming at reducing aggressiveness should focus on the development of skills to: recognize and talk about emotions and feelings; identify potentially stressful situations and the arousal of negative emotions and feelings; accept emotions and feelings, especially negative ones; identify consequences of actions; select the adequate emotion regulation strategies. Emotion-regulation interventional approaches, such as emotion-focused therapy (Greenberg, 2004) or mindfulness-based psychotherapies (Kishita et al., 2017), are possibilities as they improve awareness of present experiences and emotion regulation. Based on the theory of mentalization, an alternative is the mentalization-based psychotherapy, as it improves awareness of self and others (Bateman & Fonagy, 2010).

